
Trends and Distribution of Snakebite Incidence, Uganda, 2020–2024: An Analysis of District Health Information Software Surveillance Data
Authors: Martha Dorcas Nalweyiso1*, Justine Wobusobozi1, Aminah Namwabira1, Patricia Eyu1, Richard Migisha1, Benon Kwesiga1, Emmanuel Obuya2, Isaasi Fred2, David Were Oguttu3, Charles Kennedy Kissa3 Institutional affiliations:1Uganda National Institute of Public Health, Kampala, Uganda 2Department of Integrated Epidemiology, Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda, 3Department of Environmental Health, Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256785832362, Email: nmartha@uniph.go.ug
Summary
Background: Snakebites remain a neglected public health challenge in Uganda, with an annual incidence of 101/1,000,000 population. Snakebites have been prioritised in Uganda’s Neglected Tropical Diseases Master Plan, 2023-2027, which aligns with WHO’s target to reduce snakebite mortality and disability by 50% by 2030. We described trends and distribution of snakebite cases in Uganda, 2020–2024, to inform control efforts.
Methods: We analysed snakebite cases reported through the District Health Information Software (DHIS2) from January 2020 to December 2024 across 146 districts. We calculated annual incidence rates per 1,000,000 population stratified by age, sex, year, and district, using Uganda Bureau of Statistics (UBOS) population projections. Temporal trends were assessed using the Mann–Kendall test. Spatial distribution of snakebites was assessed using QGIS. We correlated annual district-level rainfall data from the Uganda National Meteorological Authority with snakebite incidence using the Spearman correlation coefficient.
Results: From 2020-2024, 50,011 snakebite cases were reported, yielding a mean incidence of 250/1,000,000 population. Adults aged ≥20 years had the highest incidence (320/1,000,000). Females had a slightly higher incidence (250/1,000,000) than males (240/1,000,000). A significant temporal trend in snakebite incidence was observed among females (p=0.02). Incidence declined between 2020 and 2022, with no significant overall upward trend (p=0.22).
West Nile and Acholi regions consistently reported snakebite incidence risks exceeding 1,000/1,000,000 with Moyo District among the highest annually. Rainfall showed a weak negative correlation with snakebite incidence, significant only in 2022 (ρ=−0.22, p=0.01).
Conclusion: Snakebites mostly affected adults and females, with West Nile and Acholi regions reporting the highest incidences. No significant temporal trend was observed over five years. We recommend enhancing community awareness in high-burden regions and supporting locally produced antivenom tailored to Uganda’s snake species.
Background
Snakebites are recognised by the World Health Organisation (WHO) as a top-priority neglected tropical disease (NTD) with a particularly high burden in rural, low-and middle-income (LMICs) countries, and represent a major global public health challenge (1, 2). Sub-Saharan Africa is especially affected, and annual estimates indicate 421,000 to 500,000 snakebites occur, resulting in up to 32,000 deaths, leaving survivors with permanent disabilities and socio-economic consequences (3, 4).
In Uganda, Snakebite Envenoming (SBE) is a significant public health threat, especially within the agricultural sector, where nearly 70% of the population is employed. Farming activities frequently expose individuals to snake habitats, increasing the risk of snakebites (5, 6). The estimated national incidence is at 10.1 cases per million people annually, with higher rates reported in certain districts such as Gulu and Nakapiripirit (7). Uganda’s biodiversity includes more than 200 snake species whose bites can cause illness, disability, and death in humans (8, 9).
Despite the high burden of snakebites, Uganda’s healthcare response is limited. Critical shortages of antivenom mean that only 4% of health facilities have the treatment (7, 10). This challenge is exacerbated by knowledge gaps among healthcare practitioners (HCPs), resulting in delayed or suboptimal care (11, 12). Consequently, snakebite victims seek help from traditional healers first, influenced by accessibility, affordability, and cultural beliefs (13-16). Ethnobotanical studies in Uganda have identified over 77 plant species used as folk remedies for snakebites, alongside harmful practices, such as applying tourniquets, black stones, or coins to bite wounds (14, 17).
In response, the Ugandan Ministry of Health has added SBE to the national list of neglected tropical diseases and drafted a strategic plan for prevention and management (18). However, implementation is challenged by a lack of detailed, up-to-date information on the epidemiology and spatial distribution of cases, as well as the interplay between community behaviours and the formal health system. Environmental factors, especially rainfall and temperature, influence snakebite incidence, but these relationships vary by region and are not fully understood in Uganda (19, 20).
In Uganda, snakebite cases are routinely reported monthly by health workers through the District Health Information Software version 2 (DHIS2); however, gaps remain in understanding the true magnitude and spatial distribution of cases. We analysed DHIS2 data to examine trends and the distribution of snakebites in Uganda, 2020-2024.
Methods
This study employed a descriptive design, utilising DHIS2 and rainfall data from the Uganda National Meteorological Authority (UNMA), covering the period from January 2020 to December 2024. Snakebite cases were defined as injuries resulting from snake bites, with or without clinical signs of envenomation, as reported by health facilities. Study variables included year of reporting, district, number of snakebite cases, age group, sex, and population estimates. Rainfall data consisted of annual totals aggregated at the district level to align with snakebite surveillance data.
Descriptive analyses were conducted by person (age group, sex), place (district), and time (year). Snakebite incidence rates were calculated using reported cases as the numerator and district-level population projections from the Uganda Bureau of Statistics (UBOS) as the denominator, stratified by age group and sex.
Temporal trends were analysed using annual variations in case counts and incidence rates, visualised with line graphs, and assessed using the Mann–Kendall trend. Spatial analysis was performed in Quantum GIS to generate district-level choropleth maps of incidence. The relationship between annual rainfall and snakebite incidence was examined using Spearman’s rank correlation, with statistical significance set at p<0.05. All statistical analyses were conducted using Stata version 17.
The study used routine surveillance data from health facilities in DHIS2, which were aggregated without individual patient identifiers. However, we obtained administrative clearance to use the data from the Uganda Ministry of Health. The US Centers for Disease Control and Prevention (CDC) also determined that this activity was not human subject research and that its primary intent was public health practice or disease control. This activity was reviewed by CDC and conducted in accordance with applicable federal law and CDC policy. §§See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.
Results
Person characteristics of snakebite cases, Uganda, 2020-2024
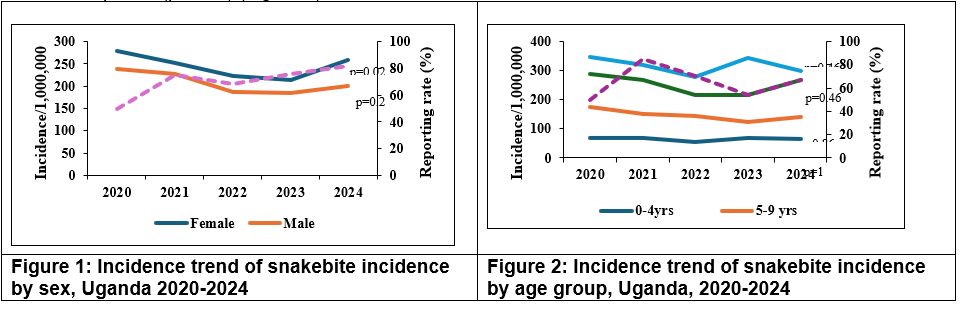
A total of 50,011 snakebite cases were reported between 2020-2024. Of these, 2,385(4.8%) were children <5 years, 4,750(9.5%) aged 5-9 years, 13,680(27.4%) aged 10-19 years, and 29,196(58.4%) aged ≥20 years. Females accounted for 27,474(54.9%) of all cases. The highest proportion of cases was reported in 2024 (10,802,21.6%), followed by 2020 (10,737,21.5%), while the lowest number was registered in 2022 (9,088,18.2%). The mean incidence among females was 245/1,000,000 compared to 208/1,000,000 among males. A statistically significant temporal trend was observed among females (p=0.02) (Figure 1).
Incidence varied across age groups, with adults aged ≥20 years recording the highest incidence throughout the study period. There were no statistically significant temporal trends observed across any age category. Incidence declined from 259/1,000,000 in 2020 to 200/1,000,000 in 2023, then increased to 230/1,000,000 in 2024. Despite these fluctuations, no statistically significant temporal trend was observed over the study period (p = 0.2) (Figure 2).
Spatial distribution of snakebite incidence in Uganda 2020-2024
The national incidence was 250/1,000,000 population, with the proportion of affected districts reporting fluctuating between 14% and 21% over the study period (2020-2024). Mean annual district-level incidence ranged from 20 to 30/1,000,000 population and statistical testing showed no significant trend across years. The burden was consistently concentrated in Northen Uganda with Lamwo, Obongi, Moyo, Kitgum, and Pakwach districts recording risk exceeding 1,000/1,000,000 population, while Luwero District in Central Uganda emerged as a notable new hotspot in 2024 [Figure 3].
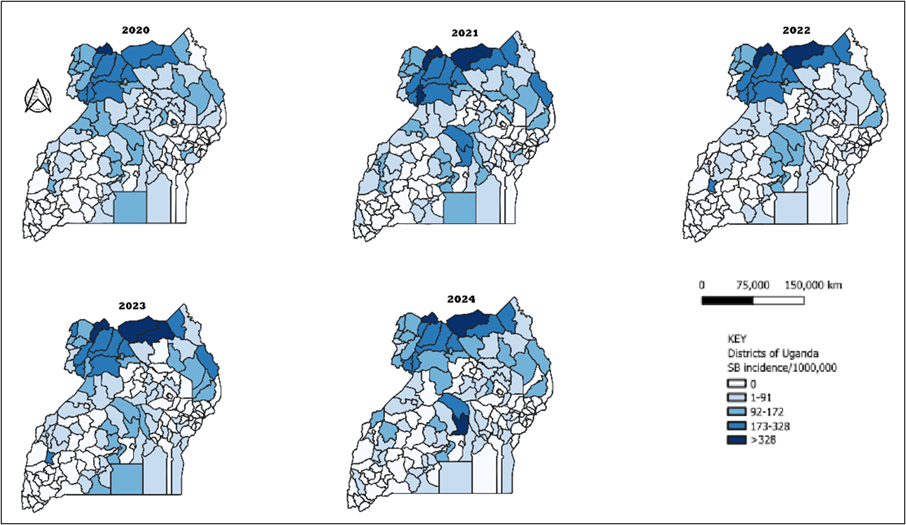
Table 1: Correlation between rainfall (mm) and annual snakebite incidence, Uganda, 2020-2024
| Year | Outcome | Number of districts (n) | Spearman’s ρ | p-value |
| 2020 |
snakebite incidence |
146 |
−0.03 | 0.72 |
| 2021 | −0.11 | 0.17 | ||
| 2022 | −0.22 | 0.01 | ||
| 2023 | −0.10 | 0.21 | ||
| 2024 | −0.06 | 0.49 |
Spearman’s rank correlation analysis examining the association between annual rainfall and snakebite incidence across districts showed evidence of a statistically significant correlation only in 2022. In that year, a weak negative correlation was observed (ρ=−0.22, p=0.01). In contrast, no evidence of a statistically significant correlation between annual rainfall and snakebite incidence was observed in 2020 (ρ=−0.03, p = 0.72), 2021 (ρ=−0.11, p=0.17), 2023 (ρ=−0.10, p=0.21), or 2024 (ρ=−0.06, p=0.49).
Discussion
Our study showed a higher incidence of snakebites among adult females and in Northern region, largely reflecting occupational exposure in agricultural activities (11, 21). While adults bear the greatest burden, cases among children and adolescents indicate additional risks during play and farm tasks, underscoring the need for community-wide education. and availability of pediatric antivenom in essential drug supplies (22). The higher incidence among females differs from patterns reported in many other regions, where males are more affected (6). In Uganda, this may be explained by women’s prominent involvement in agriculture and possible differences in health-seeking behaviours (23).
Snakebite incidence declined after 2020 but increased between 2023-2024, indicating temporal variation. The incidence in 2020 may be linked to heightened surveillance and behavioral changes during the COVID-19 pandemic (24). The subsequent decline in 2022–2023 may reflect shifts in reporting, health system performance, or exposure patterns. The rise of cases in 2024 suggests a combination of surveillance practices, environmental factors, and population exposure (25). Similar rainfall-associated increases in snakebite incidences have been documented in Africa and Asia (25, 26).
Snakebite incidence remains concentrated in Northern Uganda particularly in West Nile and Acholi with parts of the central region in Luwero District. The high burden is likely driven by the presence venomous species combined with intense agricultural activity that increases human exposure (27). The emergence of Luwero District suggests shifting risk patterns, possibly due to land-use changes, population expansion, and improved reporting.
Annual rainfall showed no consistent association with snakebite incidence across the study period. Only in 2022 was a weak negative correlation observed; in other years, no significant relationship was found. This suggests that rainfall alone does not explain differences in snakebite burden, which are likely shaped by additional factors such as agricultural practices, land use, and human exposure patterns (25, 28). Aggregated annual data may also obscure important seasonal effects relevant to snakebite risk (25, 29, 30).
Study limitations
We relied on DHIS2 routine surveillance data, which may underestimate the burden of snakebites due to underreporting and inconsistent reporting across districts and over time. The data also lacked detailed clinical information (snake species, envenomation severity, outcomes, time to treatment), limiting in-depth analysis.
Conclusion
Snakebites remain a major public-health concern in Uganda, with incidence rates exceeding 100/1,000,000 between 2020-2024, disproportionately affecting adults, females and children. The Northern region bears the highest burden with emerging hotspots Luwero District. We recommend enhancing community awareness in high-burden regions and supporting locally produced antivenom tailored to Uganda’s snake species.
Conflict of interest: The authors declare that they have no conflict of interest.
Authors’ contributions
MDN participated in the conception, design, analysis, and interpretation of the study and wrote the draft bulletin. JW, AN, PE, RM, BK, RM, DK, EO, FI, DWO, and CKK reviewed the report and the drafts of the bulletin for intellectual content and made multiple edits to the draft bulletin; BK, RM, and ARA reviewed the final bulletin to ensure intellectual content and scientific integrity. All authors read and approved the final bulletin.
Acknowledgement
We thank the staff of the Uganda Public Health Fellowship Program and Uganda Public Health Emergency Operation Centre for the technical support and guidance offered during this work. We also thank the US-CDC for supporting the activities of the Uganda Public Health Fellowship Program under which this work was done.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or republished. If cited as a reprint, it should be referenced in the original form.
References
- Williams DJ, Faiz MA, Abela-Ridder B, Ainsworth S, Bulfone TC, Nickerson AD, et al. Strategy for a globally coordinated response to a priority neglected tropical disease: Snakebite envenoming. PLoS neglected tropical diseases. 2019;13(2):e0007059.
- World Health Organisation. Snakebite envenoming 2023 [Available from: https://www.who.int/news-room/fact-sheets/detail/snakebite-envenoming.
- Chippaux JP. Snake-bites: appraisal of the global situation. Bulletin of the World Health organization. 1998;76(5):515.
- Kasturiratne A, Wickremasinghe AR, De Silva N, Gunawardena NK, Pathmeswaran A, Premaratna R, et al. The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS medicine. 2008;5(11):e218.
- Uganda K. Uganda Bureau of Statistics. Kampala, Uganda and Calverton. 2016.
- Ooms GI, van Oirschot J, Waldmann B, von Bernus S, van Den Ham HA, Mantel-Teeuwisse AK, et al. The current state of snakebite care in Kenya, Uganda, and Zambia: healthcare workers’ perspectives and knowledge, and health facilities’ treatment capacity. The American Journal of Tropical Medicine and Hygiene. 2020;104(2):774.
- Ddamulira J, Kasasa S, Kizito S. The Burden of Snakebite and Snakebite Envenoming in Uganda: A Community Survey and Facility Audit. Kampala, Uganda: Makerere University. 2021.
- The Surgery. Poisonous snakes in Uganda 2025 [Available from: https://thesurgeryuganda.org/poisonous-snakes-in-uganda/.
- Rentokil U. Types of snakes in Uganda 2025 [Available from: https://www.rentokil.co.ug/snakes/species/.
- Health Action International. Snakebite project in Uganda, Fact Sheet 2019 [Available from: https://nru.uncst.go.ug/server/api/core/bitstreams/7fa55c67-adfa-4e1f-9650-a5dacf1acf15/content.
- Wafula ST, Mugume IB, Namakula LN, Nalugya A, Naggayi V, Walekhwa AW, et al. Healthcare practitioners’ knowledge of snakebite management and associated factors in high-burden, low-resource settings in Uganda. Transactions of The Royal Society of Tropical Medicine and Hygiene. 2023;117(8):569-79.
- Tusabe J, Muhoozi M, Kajungu D, Mukose A, Kasasa S, Sebina Kibira SP. Knowledge, perceptions and healthcare practices of communities for management of snakebites in Kamuli District, Eastern Uganda. Transactions of The Royal Society of Tropical Medicine and Hygiene. 2025;119(4):418-31.
- Steinhorst J, Aglanu LM, Ravensbergen SJ, Dari CD, Abass KM, Mireku SO, et al. ‘The medicine is not for sale’: practices of traditional healers in snakebite envenoming in Ghana. PLOS Neglected Tropical Diseases. 2021;15(4):e0009298.
- Schioldann E, Mahmood MA, Kyaw MM, Halliday D, Thwin KT, Chit NN, et al. Why snakebite patients in Myanmar seek traditional healers despite availability of biomedical care at hospitals? Community perspectives on reasons. PLoS neglected tropical diseases. 2018;12(2):e0006299.
- Omara T, Kagoya S, Openy A, Omute T, Ssebulime S, Kiplagat KM, et al. Antivenin plants used for treatment of snakebites in Uganda: ethnobotanical reports and pharmacological evidences. Tropical Medicine and Health. 2020;48(1):6.
- The Daily Monitor. How to get rid of snakebites 2015 [Available from: https://www.monitor.co.ug/uganda/magazines/healthy-living/using-nature-to-get-rid-of-snakes-and-their-venom-1622448.
- Adu-Gyamfi S. Spiritual and indigenous healing practices among the Asante people of Ghana: A testimonial from twenty-first century practitioners and recipients in Kumase. Journal of Basic and Applied Research International. 2016;12(1):39-50.
- HEPS Uganda. Uganda Reviews Snakebite Prevention and Management Strategy 2023 [Available from: https://www.heps.or.ug/uganda-reviews-snakebite-prevention-and-management-strategy/.
- Bravo-Vega C, Santos-Vega M, Cordovez JM. Disentangling snakebite dynamics in Colombia: How does rainfall and temperature drive snakebite temporal patterns? PLoS Negl Trop Dis. 2022;16(3):e0010270.
- Gutiérrez JD, Bravo-Vega C, Cordovez JM. Causal inference unveils how forest coverage mitigates excess snakebite cases during rainfall seasons in Colombia. Sci Rep. 2025;15(1):32401.
- Nanyonga SM, Matafwali SK, Kibira D, Kitutu FE. Treatment and treatment outcomes of snakebite envenoming in Uganda: a retrospective analysis. Transactions of The Royal Society of Tropical Medicine and Hygiene. 2025;119(7):796-803.
- Moos B, Williams D, Bolon I, Mupfasoni D, Abela-Ridder B, de Castaneda RR. A scoping review of current practices on community engagement in rural East Africa: Recommendations for snakebite envenoming. Toxicon: X. 2021;11:100073.
- Aglanu LM, Amuasi JH, Prokesh E, Beyuo A, Dari CD, Ravensbergen SJ, et al. Community members and healthcare workers’ priorities for the control and prevention of snakebite envenoming in Ghana. PLOS Neglected Tropical Diseases. 2023;17(7):e0011504.
- Musoke D, Nalinya S, Lubega GB, Deane K, Ekirapa-Kiracho E, McCoy D. The impact of the COVID-19 lockdown on social and economic welfare in Uganda. Archives of Public Health. 2024;82(1):117.
- Bravo-Vega C, Santos-Vega M, Cordovez JM. Disentangling snakebite dynamics in Colombia: how does rainfall and temperature drive snakebite temporal patterns? PLOS Neglected Tropical Diseases. 2022;16(3):e0010270.
- Bhaumik S, Beri D, Jagnoor J. The impact of climate change on the burden of snakebite: evidence synthesis and implications for primary healthcare. Journal of Family Medicine and Primary Care. 2022;11(10):6147-58.
- Warrell DA, Williams DJ. Clinical aspects of snakebite envenoming and its treatment in low-resource settings. The Lancet. 2023;401(10385):1382-98.
- Mugasha R, Kwiringira A, Ntono V, Nakiire L, Ayebazibwe I, Kyozira C, et al. Enhancing functionality and scaling up of the electronic Integrated Diseases Surveillance and Response system in Uganda, 2020-2023: Description of the journey, challenges, and lessons learned.
- Landry M, D’Souza R, Moss S, Chang HH, Ebelt S, Wilson L, et al. The association between ambient temperature and snakebite in Georgia, USA: a case‐crossover study. GeoHealth. 2023;7(7):e2022GH000781.
- Ediriweera DS, Kasthuriratne A, Pathmeswaran A, Gunawardene NK, Jayamanne SF, Murray K, et al. Evaluating spatiotemporal dynamics of snakebite in Sri Lanka: Monthly incidence mapping from a national representative survey sample. PLoS neglected tropical diseases. 2021;15(6):e0009447.
Comments are closed.