
Comparison of Medically Certified and DHIS2-Reported Neonatal Sepsis Mortality in Uganda, 2020–2025.
Sharon Namasambi*1, Richard Migisha1, Irene Kyamwine1, Collins Ankunda2, Winfred Nakaweesi1, Pauline Achom1, Benon Kwesiga1, Fred Nsubuga3 Institutional affiliation:1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Department of Pharmacology, Makerere University, Kampala, Uganda, 3Uganda National Expanded Program on Immunisation, Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256 772 511 067, Email: nabsharon@uniph.go.ug
Summary
Background: In Uganda, neonatal deaths are routinely reported through District Health Information Software 2 (DHIS2); however, the extent of formal medical certification using International Classification of Diseases, 10th Revision (ICD-10) within the Medical Certification of Cause of Death–Civil Registration and Vital Statistics system (MCCOD-CRVS) platform remains poorly described. Assessing the concordance between MCCOD-certified deaths and DHIS2-reported data is essential to strengthen mortality surveillance, improve data quality, and inform targeted interventions to reduce preventable neonatal mortality. We compared NS-related deaths reported in DHIS2 with those medically certified in the MCCOD-CRVS system to quantify concordance between the two platforms and identify gaps to strengthen vital statistics systems.
Methods: We conducted a national-level descriptive analysis using DHIS2 data from 2020–2025. All facility-reported NS deaths during this period were identified and cross-referenced with Uganda’s MCCOD-CRVS system to determine the proportion that received formal ICD-10 medical certification. The proportion of medically certified deaths was calculated annually, and monotonic trends in annual proportions were assessed using the Mann-Kendall test.
Results: A total of 6,427 neonatal sepsis–related deaths were reported in DHIS2 from 2020–2025, of which 564 (8.8%) were medically certified in the MCCOD-CRVS system. Certification increased significantly over time from 0.1% in 2020 to 26.2% in 2025 (τb=0.87, p=0.02), while no significant trend was observed in total reported deaths (τb=0.20, p=0.71). Certified deaths were highly concentrated in regional and national referral hospitals (89.5%), with minimal contributions from lower-level facilities.
Conclusion: Substantial discordance persists between DHIS2-reported and MCCOD-CRVS–certified neonatal sepsis deaths in Uganda, with overall certification remaining low despite recent gains. The concentration of certification in higher-level facilities highlights gaps across the health system. Strengthening and decentralising medical certification, alongside improved integration of routine surveillance with CRVS systems, is essential to enhance mortality data quality and better inform efforts to reduce preventable neonatal deaths.
Background
Accurate and complete cause-of-death data are essential for tracking progress toward Sustainable Development Goal (SDG) 3.2, which aims to end preventable neonatal deaths by 2030. High-quality mortality data enable countries to monitor trends, prioritize interventions, and allocate resources effectively. However, in many low- and middle-income countries, including Uganda, weaknesses in civil registration and vital statistics (CRVS) systems and incomplete medical certification of deaths limit the availability of reliable cause-of-death information(1–3).These gaps undermine the ability to accurately quantify disease burden and evaluate the impact of newborn health interventions.
In Uganda, neonatal deaths are routinely reported through the District Health Information Software 2 (DHIS2), that captures aggregated facility-based data. While DHIS2 provides timely and broad coverage, cause-of-death attribution is often based on clinical judgment and may be affected by diagnostic uncertainty and inconsistent reporting (4).In contrast, the Medical Certification of Cause of Death–Civil Registration and Vital Statistics (MCCOD-CRVS) system applies standardized International Classification of Diseases, 10th Revision (ICD-10) coding and is considered the gold standard for assigning underlying causes of death (2,5). Despite this, MCCOD coverage in Uganda remains limited, and the extent of concordance between MCCOD-certified deaths and DHIS2-reported mortality has not been well determined. We compared NS-related deaths reported in DHIS2 with those medically certified in the MCCOD-CRVS system to quantify concordance between the two platforms and identify gaps to strengthen vital statistics systems.
Methods
We conducted a descriptive trend analysis of routinely collected facility-based surveillance data to compare neonatal sepsis (NS) deaths reported in Uganda’s District Health Information Software 2 (DHIS2) with medically certified NS deaths captured in the Medical Certification of Cause of Death–Civil Registration and Vital Statistics (MCCOD-CRVS) system from 2020 to 2025. The analysis included all public and private health facilities reporting to DHIS2 at Health Centre III level and above across Uganda’s districts. The study population comprised all facility-based neonatal deaths (0–28 days) attributed to sepsis in DHIS2 and those medically certified with ICD-10 code KA60 (neonatal sepsis) in the MCCOD-CRVS system over the same period.
Data were extracted from monthly inpatient reports (HMIS Form 108-ND01b) submitted to DHIS2 and from MCCOD-CRVS records. We summarized the annual and overall number of NS deaths reported in each system for 2020–2025. The proportion of DHIS2-reported deaths that were medically certified in MCCOD-CRVS was calculated for each year; and was compared across health facility levels.
Temporal trends in certification were assessed using the Mann–Kendall trend test to evaluate changes in the proportion of DHIS2-reported deaths captured in MCCOD-CRVS over time. Permission to access HMIS data was obtained from the Ministry of Health Resource Centre. The activity was classified by the U.S. Centers for Disease Control and Prevention (CDC), Center for Global Health, as non-research, as it was conducted to support public health practice and data use for decision-making.
Results
Trends in DHIS2 reported and MCCOD-certified deaths, 2020–2025
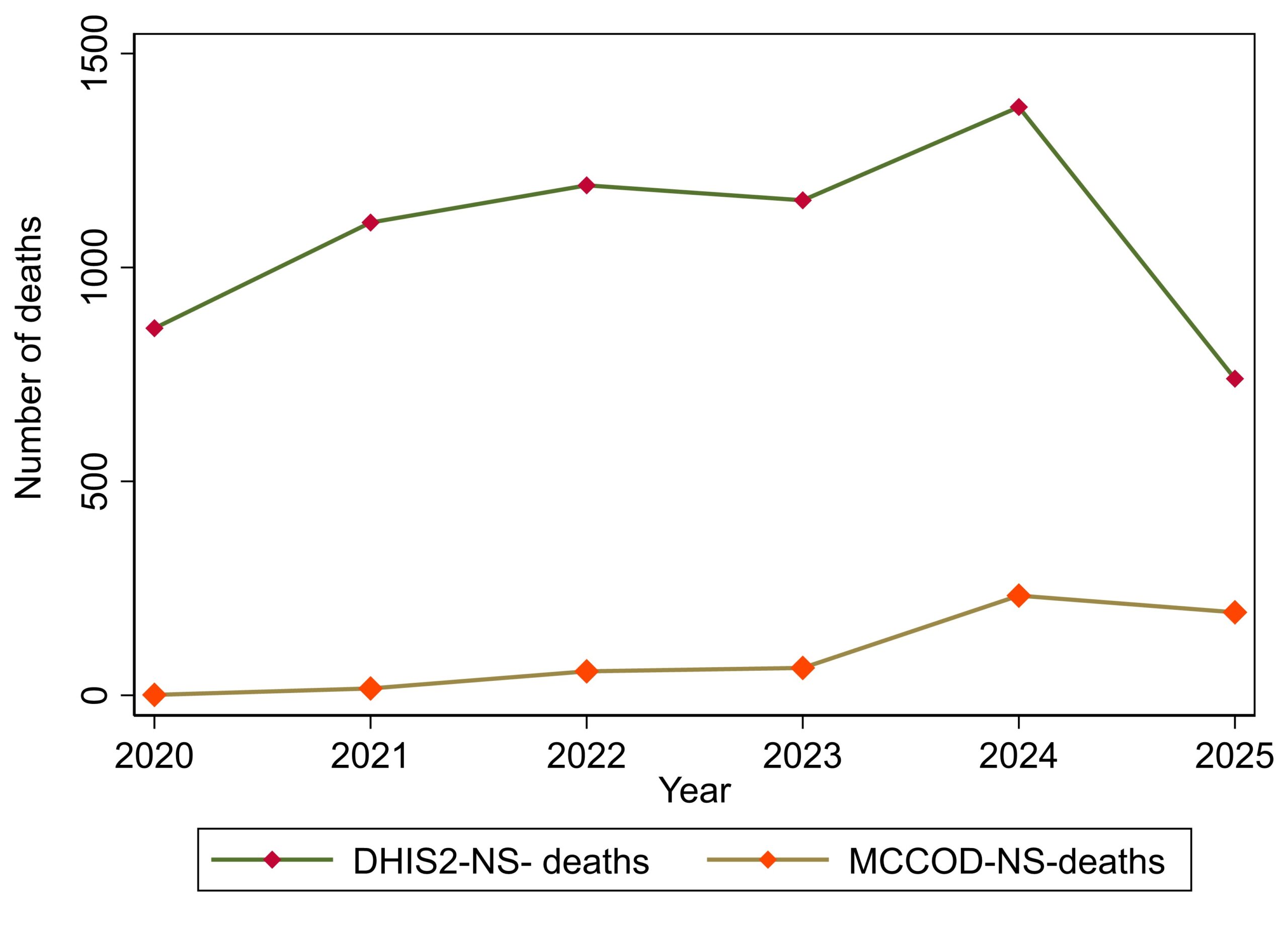
A total of 6,427 neonatal sepsis (NS)-related deaths were reported in DHIS2 between 2020 and 2025, of which 564 (8.8%) were medically certified using the Medical Certificate of Cause of Death (MCCOD).
Cause of death certification increased significantly over time, from 0.1% (1/858) in 2020 to 26.2% (194/740) in 2025; (τb=0.87, p=0.02), demonstrating a strong upward trend in certification. In contrast, there was no significant monotonic trend in total DHIS2-reported deaths over time (τb=0.20, p=0.71) (Figure 1).
Distribution of certified Neonatal sepsis deaths across health facility levels in Uganda, 2020-2025
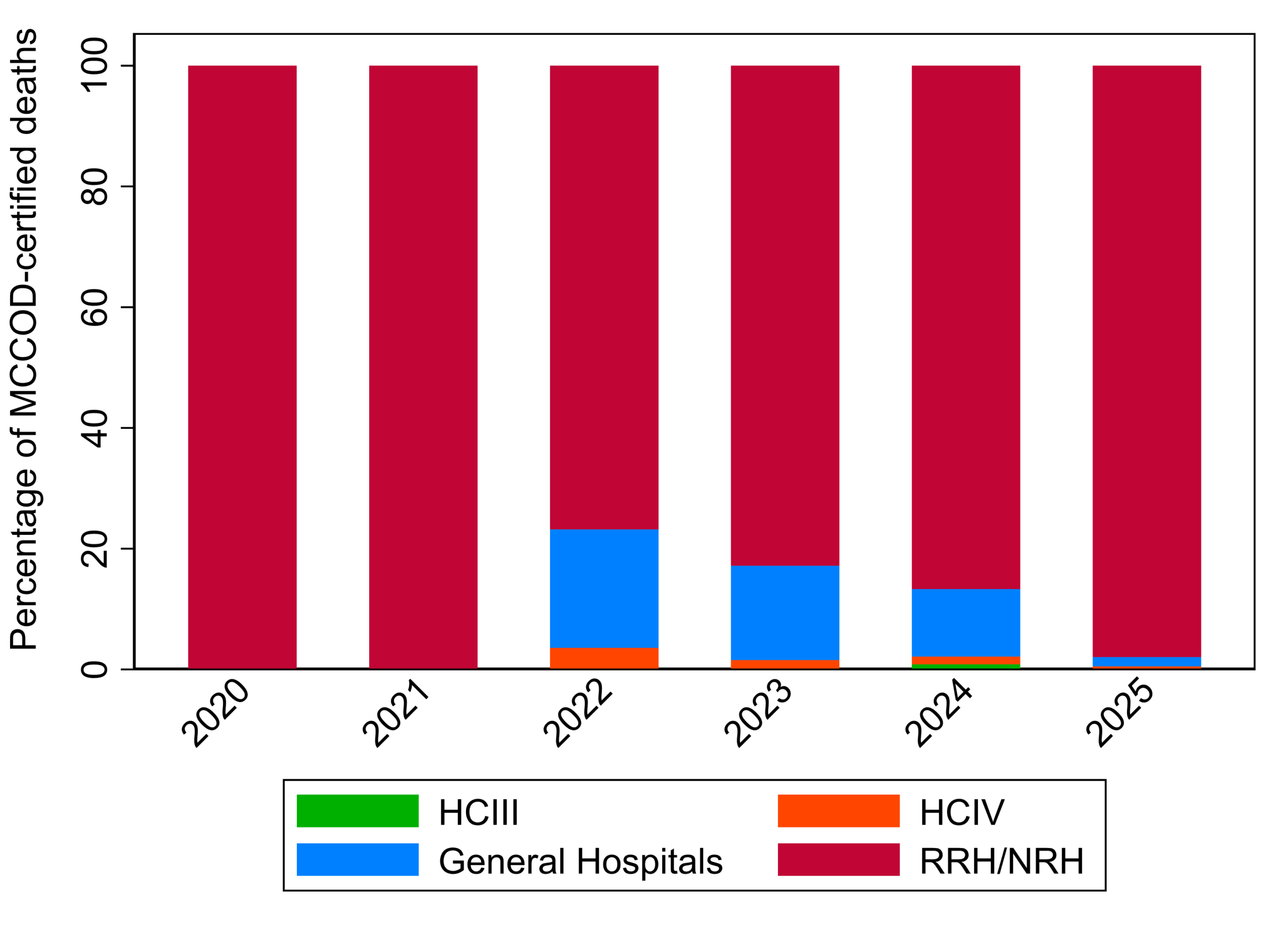
Medical certification of neonatal sepsis (NS) deaths was highly concentrated at higher-level health facilities. Of the 564 certified deaths, 89.5% (505) occurred in regional and national referral hospitals (RRH/NRH), followed by general hospitals (8.9%), Health Centre IVs (1.2%), and Health Centre IIIs (0.4%). Across the study period, RRH/NRH facilities consistently accounted for the majority of certifications each year, contributing over 80% annually, while certification at lower-level facilities remained minimal throughout the period (Figure 2).
Discussion
Our analysis reveals a substantial gap between DHIS2-reported neonatal sepsis (NS) deaths and medically certified deaths in Uganda’s MCCOD-CRVS system. Over the six-year period, only 8.8% of NS-related deaths reported in DHIS2 were formally certified using ICD-10 processes; medical certification increased from 0.1% in 2020 to 26.2% in 2025; and nearly 80% of certified deaths occurred in referral hospitals.
The persistent under certification observed in our study aligns with broader evidence from sub-Saharan Africa, where discrepancies between routine health information systems and civil registration data are well documented (6,7). Although medical certification improved markedly over the study period, the overall low concordance limits the ability to validate DHIS2-reported deaths and accurately assess the true population-level burden of neonatal sepsis.
The discordance between DHIS2 and MCCOD-CRVS may reflect inherent differences in how deaths are captured and classified in these two systems. Routine health management information systems (HMIS) like DHIS2 often rely on syndromic or clinical diagnoses recorded by frontline health workers without formal medical certification or standardized ICD-10 coding (4,8). In contrast, CRVS systems require structured cause-of-death certification following WHO guidelines, which includes completing medical certificates of cause of death and applying ICD coding by trained personnel (9).
Studies from Kenya, Tanzania, and Ethiopia have similarly documented substantial discrepancies between HMIS mortality data and medically certified deaths.
For instance, a Kenyan study found that only 15% of neonatal deaths reported in HMIS were medically certified, comparable to our 8.8% finding(10,11).
The concentration of certified deaths in higher-level facilities is consistent with international literature showing that referral and tertiary hospitals are more likely to have staff trained in MCCOD and better adherence to ICD coding practices(12,13)
In our study, nearly 80% of certified deaths occurred in referral hospitals, reflecting both greater case severity at these levels and enhanced capacity for formal death certification. This hierarchical pattern has been observed across multiple sub-Saharan African countries, where certification rates rise with facility level but remain inadequate overall, undermining national mortality surveillance(14)
The marked improvement in medical certification from 0.1% in 2020 to 26.2% in 2025 suggests that Uganda’s investments in strengthening CRVS systems, including training health workers on MCCOD, expanding access to certification tools, and integrating MCCOD modules into DHIS2, are yielding measurable results(15).
Similar improvements have been documented in countries that prioritized CRVS strengthening as part of national health information system reforms, such as Rwanda and South Africa(16,17). However, the persistence of a large certification gap indicates that substantial barriers remain, including limited human resources, competing clinical priorities, and insufficient supervision and quality assurance mechanisms at facility level
In summary, our findings emphasise the critical need to bridge the gap between routine surveillance and formal certification systems. Without reliable, standardised cause-of-death data, policy-making and resource allocation for newborn health remain inadequately informed, potentially undermining interventions aimed at reducing preventable neonatal mortality. Enhancing concordance between DHIS2 and MCCOD-CRVS data will improve the accuracy of neonatal mortality estimates, inform targeted interventions, and ultimately support Uganda’s efforts to meet SDG 3.2.
Study limitations
The study relied on aggregated routine surveillance data, limiting the ability to assess individual-level agreement between DHIS2 and MCCOD-CRVS records. However, this was mitigated by using national-level data over a six-year period and applying trend analysis to provide robust insights into patterns of concordance between the two systems.
Conclusion
Substantial discordance exists between DHIS2-reported and MCCOD-CRVS certified neonatal sepsis deaths in Uganda, with persistently low certification despite recent improvements. The marked concentration of certification in higher-level facilities highlights critical gaps at lower-level facilities, highlighting the need to decentralise and strengthen medical certification practices. Enhancing integration between routine surveillance and CRVS systems, alongside targeted capacity building at facility level, is essential to improve mortality data quality and guide interventions to reduce preventable neonatal deaths.
Conflict of Interests: The authors declare no conflict of interests.
Author Contributions: SN conceptualized, led data collection, analysis and report writing. WN and PA supported data collection and review of draft report. RM, CA and IK supported technical review of data analysis, and report writing. SN, CA, and RM contributed to writing and reviewing the bulletin article to ensure scientific rigor and intellectual content. All authors reviewed and approved the final bulletin for submission.
Acknowledgements: We acknowledge the Ministry of Health Division of Health Information for granting access to the data used in this study. We also thank the Ministry of Health Reproductive Health Department and the Uganda Public Health Fellowship Program for their valuable technical support.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission. However, citation as to source is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- World Health Organisation. Covering every birth and death: improving civil registration and vital statistics (CRVS) [Internet]. 2014 [cited 2026 Mar 27]. Available from: https://iris.who.int/items/501ecdd3-4c30-4b37-a8ee-af5df864d475
- World Health Organisation. Civil registration and vital statistics [Internet]. 2025 [cited 2026 Mar 27]. Available from: https://www.who.int/news-room/fact-sheets/detail/civil-registration-and-vital-statistics
- AbouZahr C, de Savigny D, Mikkelsen L, Setel PW, Lozano R, Nichols E, et al. Civil registration and vital statistics: progress in the data revolution for counting and accountability. Lancet Lond Engl. 2015 Oct 3;386(10001):1373–85. doi:10.1016/S0140-6736(15)60173-8 PubMed PMID: 25971224; PubMed Central PMCID: PMC7753937.
- Iburg KM, Mikkelsen L, Adair T, Lopez AD. Are cause of death data fit for purpose? evidence from 20 countries at different levels of socio-economic development. PLOS ONE. 2020 Aug 24;15(8):e0237539. doi:10.1371/journal.pone.0237539
- World Health Organisation. International Classification of Diseases (ICD) [Internet]. 2024 [cited 2026 Mar 27]. Available from: https://www.who.int/standards/classifications/classification-of-diseases
- Mikkelsen L, Phillips DE, AbouZahr C, Setel PW, Savigny D de, Lozano R, et al. A global assessment of civil registration and vital statistics systems: monitoring data quality and progress. The Lancet. 2015 Oct 3;386(10001):1395–406. doi:10.1016/S0140-6736(15)60171-4 PubMed PMID: 25971218.
- Setel PW, Macfarlane SB, Szreter S, Mikkelsen L, Jha P, Stout S, et al. A scandal of invisibility: making everyone count by counting everyone. The Lancet. 2007 Nov 3;370(9598):1569–77. doi:10.1016/S0140-6736(07)61307-5 PubMed PMID: 17992727.
- Countdown to 2030: tracking progress towards universal coverage for reproductive, maternal, newborn, and child health – The Lancet [Internet]. [cited 2026 Mar 27]. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)30104-1/abstract
- World Health Organisation. Medical certification of cause of death : instructions for physicians on use of international form of medical certificate of cause of death [Internet]. 2016 [cited 2026 Mar 27]. Available from: https://iris.who.int/items/59fc64df-14ed-44f2-a115-a1137c3a998f
- Shabani J, Salim N, Bohne C, Day LT, Kumalija C, Makuwani AM, et al. Neonatal indicator data in Tanzania District Health Information System: evaluation of availability and quality of selected newborn indicators, 2015-2022. BMC Pediatr. 2025 Jan 23;23(Suppl 2):658. doi:10.1186/s12887-025-05417-x PubMed PMID: 39849367; PubMed Central PMCID: PMC11755859.
- Irimu G, Aluvaala J, Malla L, Omoke S, Ogero M, Mbevi G, et al. Neonatal mortality in Kenyan hospitals: a multisite, retrospective, cohort study. BMJ Glob Health. 2021 May 31;6:e004475. doi:10.1136/bmjgh-2020-004475
- Mahapatra P, Shibuya K, Lopez AD, Coullare F, Notzon FC, Rao C, et al. Civil registration systems and vital statistics: successes and missed opportunities. The Lancet. 2007 Nov 10;370(9599):1653–63. doi:10.1016/S0140-6736(07)61308-7 PubMed PMID: 18029006.
- Kazonga E, Mwinga DKK. Strengthening of Civil Registration and Vital Statistics System for Enhanced Public Health Information in Zambia.
- Ye Y, Wamukoya M, Ezeh A, Emina JBO, Sankoh O. Health and demographic surveillance systems: a step towards full civil registration and vital statistics system in sub-Sahara Africa? BMC Public Health. 2012 Sep 5;12(1):741. doi:10.1186/1471-2458-12-741
- Ministry of Health. National Mortality Surveillance Roadmap 2024_25 – 2027_28 edited [Internet]. 2024. Available from: https://library.health.go.ug/sites/default/files/resources/National%20Mortality%20Surveillance%20Roadmap%202024-2028.pdf
- Yokobori Y, Matsuura J, Obara H, Sugiura Y, Kitamura T, Moyo C, et al. Rapid assessment of the civil registration and vital statistics performance of health facilities in the five districts of Zambia: A cross-sectional study. Heliyon. 2021 Nov 11;7(11): e08367. doi: 10.1016/j. heliyon.2021.e08367 PubMed PMID: 34825083; PubMed Central PMCID: PMC8605283.
- Dorrington R, Bradshaw D, Laubscher R, Nannan N. RAPID MORTALITY SURVEILLANCE REPORT 2019 & 2020.
Comments are closed.