
Cholera outbreak following cross-border introduction and consumption of untreated River Nile water, Moyo District, Uganda, June–July 2025
Authors: Martha Dorcas Nalweyiso1*, Justine Wobusobozi1, Aminah Namwabira1, Patricia Eyu1, Richard Migisha1, Benon Kwesiga1, Bonny Kintu2, Godfrey Bwire2 Institutional affiliations:1Uganda National Institute of Public Health, Kampala, Uganda 2Department of Integrated Epidemiology, Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256785832362, Email: nmartha@uniph.go.ug
Summary
Background: Cholera is endemic in Uganda, with periodic outbreaks occurring naturally. On June 12, 2025, Uganda’s Ministry of Health was notified of a cholera outbreak in Dufile Sub-county, Moyo District. We investigated to determine the source and magnitude of the outbreak and recommend evidence-based control measures.
Methods: We defined a suspected case as onset of watery diarrhoea in a resident of Moyo District aged ≥2 years with Vibrio cholerae O1 or O139 detected by a rapid diagnostic test (RDT) from June 5–July 8, 2025. A confirmed case was a suspected case with Vibrio cholerae O1 or O139 isolated by stool culture. Cases were identified by active case search and records review at health facilities. We conducted descriptive epidemiology and environmental assessments. We then calculated attack rates (ARs) by sex and subcounty.
Results: We identified 17 confirmed cases with no deaths. Nine cases (53%) were female, with a median age of 27 years (range:5–57). Attack rates (AR) were similar among females (1.4/10,000) and males (1.3/10,000). Dufile Sub-county accounted for 12(71%) cases and had the highest AR (10.4/10,000). The index case had travelled to Nimule, South Sudan, for trade during an ongoing outbreak. He reported drinking untreated River Nile water at the Fula section of the river in South Sudan on June 5, 2025, and developed symptoms the next day. He was transported from South Sudan to Dufile HC IV, which likely facilitated the introduction of cholera in the community. Most (14,82%) of the case-patients also reported consuming untreated water from the Fula section of the River Nile, a common water collection point.
Conclusion: The outbreak was linked to cross-border transmission, which introduced cholera into Moyo District via the index case. Ongoing community transmission was driven by consumption of untreated River Nile water and limited access to safe water sources. We recommend strengthening cross-border surveillance through enhanced screening at points of entry and improving access to safe water.
Background
Cholera is characterised by profuse watery diarrhoea and is caused by the bacterium Vibrio cholerae (1). It is transmitted through the consumption of food and water contaminated with faeces (1). It has a short incubation period of hours to 5 days, with most persons being asymptomatic, capable of transmitting infection to communities with inadequate safe water, sanitation and hygiene (2, 3). Clusters of cholera cases are common due to either contamination of the communal water source or contamination of the environment by a case (4).
Most of the global burden of cholera is seen in developing countries and areas with poor sanitation. Globally, it is estimated that 1.3 to 4 million cases and 22,000 to 143,000 deaths occur annually (5). In response, the Global Task Force on cholera set targets to reduce cholera deaths by 90% and eliminate transmission in at least 20 countries by 2030 (6). Key prevention strategies include oral vaccination in hotspots, improving water quality, sanitation and hygiene (7).
Uganda is among the cholera-endemic countries targeted for elimination by the Global Task Force for cholera (6). Uganda experiences an estimated annual incidence of 23 cases per 100,000 population, equivalent to 11,000 reported cases. Notably, 81% of these cases occur in a relatively small number of districts, accounting for only 24% of the country’s population (8). High-risk districts include those hosting fishing communities, slum dwellers, refugee settlements and those at the border (9).
Moyo is a cholera-prone district since it has never received the Oral Cholera Vaccine (OCV). The district is located in Northern Uganda along the border with South Sudan. Being a border District, Moyo has a porous border, which facilitates the transboundary movement of people, contributing to the spread of infections (9). Moyo District last experienced a cholera outbreak in August 2014 in Metu and Dufile sub-counties, and recorded four (4) deaths (10).
On June 12, 2025, the Ministry of Health was notified of a confirmed cholera case in Moyo District. We investigated to determine the source and magnitude of the outbreak to recommend evidence-based control interventions.
Methods
The outbreak occurred in Moyo District, West Nile Region, Northern Uganda. The district is bordered by South Sudan to the North with frequent cholera outbreaks. The district has 10 sub-counties, with a total population of 120,900. The district is bordered by mountains and forests that form a natural boundary with South Sudan.
We defined a suspected case as onset of watery diarrhoea in a resident of Moyo District (aged >2 years) from June 5–July 8, 2025. A confirmed case was a suspected case with Vibrio cholerae O1 or O139 confirmed by stool culture. Cases were identified through a review of medical records and active case search at health facilities.
We conducted a descriptive analysis of the cases identified from June 5–July 8, 2025, by age, sex, clinical presentation, place of residence, and possible exposures. We calculated frequencies, percentages, and attack rates by place (subcounty) and sex using the 2024 population estimates for Moyo District and the Uganda Bureau of Statistics (UBOS). An epidemic curve was used to describe the distribution of cases by the date of symptom (diarrheal) onset.
We used a case investigation form to collect information on potential exposures from randomly selected case patients. Exposures included sources of household water, contact with an individual with profuse watery diarrhoea, and travel from an area with known cholera occurrence.
Based on the hypothesis-generating interviews, consumption of untreated water and travel from South Sudan with known cholera occurrence were suspected to be the possible source of infection in this outbreak. Using a standardised environmental assessment checklist, we planned to inspect key water-collection points along the River Nile identified by case-patients. However, this was unsuccessful because the border area was inaccessible. The terrain leading to the identified sites was impassable, limiting our ability to reach and assess the suspected water-collection points along the river.
This investigation was in response to a cholera outbreak under the directive of the Ugandan Ministry of Health. The Office of the Associate Director for Science at the Center for Disease Control and Prevention (CDC), Uganda, determined that this research did not involve human subjects and that its primary intent was public health practice or disease control. Verbal informed consent was obtained from participants or, if the interviewee was a minor, from the guardian before the start of each interview.
Results
We identified 17 confirmed cholera cases of Vibrio cholerae, serotype 01 and 0139 ogawa with no deaths. The median age was 27 years (range: 5–57), and females accounted for 9 (53%) of cases. All cases presented with acute watery diarrhoea; other symptoms included abdominal pain (14,83%), vomiting (13,76%), and nausea (11,64%). Both males and females were similarly affected (attack rate: 1.4/10,000 vs.1.3/10,000). Most case-patients had primary education (12,71%), followed by ordinary level (3,18%), and no formal education (2, 12%). The main occupations were farming (5,29%), fishing (5,29%), students (4,24%), casual labourers (2,12%), and fishmongers (1,6%).
Three (3) out of 10 sub-counties were affected. Dufile Sub-county had the highest attack rate of 10.4/10,000 population, followed by Otce Town Council (1.2/10,000) and Metu Sub-county (0.5/10,000) (Figure 1). These three (3) sub-counties border South Sudan, and most cases had visited the Fula fishing site in Nimule, South Sudan, to participate in fishing activities.
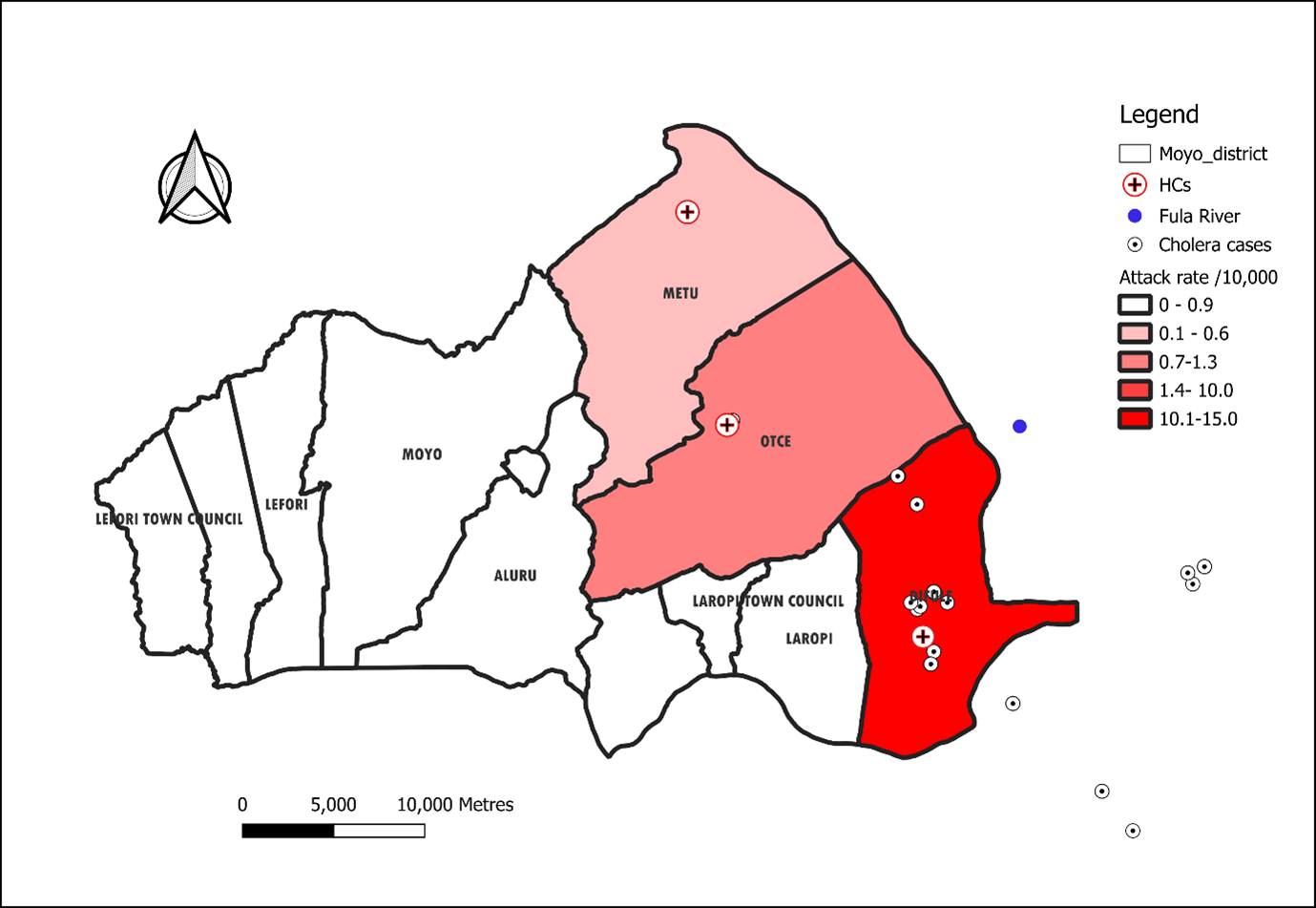
Distribution of cases
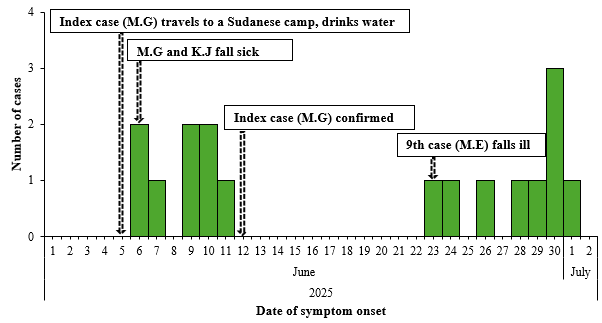
The index case, M.G. (27-year-old fisherman), visited the South Sudanese part of the camp and drank untreated water from the Fula section of River Nile on June 5, 2025, and developed symptoms (abdominal pain, loose stools, vomiting) on June 6, tested RDT-positive and stool culture-confirmed for cholera by June 12. On the same day (June 5, 2025), a fishmonger (K.J.) also travelled to the same camp to sell fish and drank contaminated water from the River Nile. Several people carried K.J from South Sudan, who was in a wet state, of whom five shared bread and drinking water, fell sick and were admitted at Dufile HC IV. The second cluster of cases was reported eighteen (18) days later, where M.E washed a mango in the Fula River and ate it. The other cases visited relatives in Sudan, leading to another cluster of the outbreak. Overall, the Moyo District experienced a point-source outbreak with clusters propagated by two cases (Figure 2).
Environmental assessment findings
Based on the inaccessibility of the Fula section of the River Nile, water samples were not collected. However, South Sudan already had an ongoing outbreak. It was noted that residents of Dufile, Otce, and Metu Sub-counties which border South Sudan use River water for bathing and washing clothes. Water for domestic use is also drawn from the same water source.
Hypothesis generation findings
Of the 17 case patients, 11 (65%) used river water for domestic purposes (bathing, cooking), 12 (71%) had contact with someone with profuse watery diarrhoea, 14 (82%) travelled from an area with known cholera occurrence, and 14 (82%) drank untreated water (Table 1). Based on the descriptive epidemiology and findings from hypothesis-generating interviews, we hypothesised that recent travel from a cholera-affected area, drinking untreated river water, using river water for domestic use and contact with a person with cholera (or profuse watery diarrhoea) were likely risk factors for this outbreak.
Table 1: Exposures among cholera case-patients, Moyo District, Uganda, June–July 2025
| Exposure (N=17) | n | (%) |
| River water* is the main source of water for domestic use | 11 | 65 |
| Contact with an individual with profuse watery diarrhoea | 12 | 71 |
| Travel from an area with known cholera occurrence. | 14 | 82 |
| Drink untreated water | 14 | 82 |
| Wash hands with soap after visiting the toilet | 14 | 82 |
*Water was fetched from a section of the River Nile locally referred to as ‘Fula’ due to the rapids.
Discussion
Our investigation confirmed a cholera outbreak in Dufile Sub-county, Moyo District, likely due to the importation of Vibrio cholerae from a cholera-affected fishing camp in South Sudan. The location of Moyo District at the Uganda-South Sudan border, combined with frequent cross-border fishing activities at the Fula section, heightened cholera vulnerability, particularly given South Sudan’s ongoing epidemic lasting two years (11). Although Moyo District had not experienced an outbreak in over 10 years despite persistent cross-border movements, the active South Sudan epidemic facilitated disease importation, with the index case acquiring cholera through consumption of contaminated water. Fishing interactions between Ugandans and South Sudanese at the Fula section amplified transmission risks, consistent with previous findings that cross-border population movements are a key driver of cholera in border districts (12, 13).
Females were more affected, with a slightly higher attack rate than males, likely reflecting their roles in water collection, food preparation, and laundry which increase exposure to contaminated water sources. Similar gender disparities have been observed in cholera-endemic settings, where women’s domestic responsibilities heighten risk (14, 15). Despite late detection, no deaths were reported, likely due to the prompt response of Cholera Treatment Units (CTU) staff, early administration of oral rehydration solution (ORS) and intravenous (IV) fluids and the index case seeking care quickly, enabling timely sample collection, diagnosis and effective treatment.
Most cases were linked to the consumption of untreated river water despite the availability of boreholes and piped treated water, suggesting persistent behavioural or access barriers, a challenge commonly observed in cholera outbreaks, consumption of contaminated water has been found to be a risk factor for outbreaks (8, 15-18).This outbreak underscores the need for enhanced cross-border surveillance, stronger community awareness of the risks posed by untreated river water and consistent access to safe water sources to prevent future outbreaks.
Study limitations
We were unable to access the Fula section of the River Nile due to inaccessibility and since all cases were linked and had similar exposures, a case-control study to assess risk factors could not be conducted.
Conclusion
Our investigation suggests that the outbreak was likely initiated through the importation of cholera following travel to a cholera-affected area in South Sudan, supported by the high proportion of case-patients reporting recent travel. Subsequent transmission likely occurred locally through consumption of untreated river water and close contact with infected individuals. The clustering of cases among fishermen, fishmongers, and their contacts indicates occupational and social exposures that facilitated both environmental and person-to-person transmission.
Public health actions
To stop the propagation of the outbreak, we conducted health education on cholera prevention and the use of safe water use. We educated residents and encouraged them to use chlorine-releasing tablets provided to make the water safe for consumption. Health care workers were trained in Infection Prevention and Control (IPC) practices and case management, and in the local preparation of Oral Rehydration Salts (ORS).
Recommendations
We recommend intensifying door-to-door safe water messaging in Dufile Sub-county and riverine parishes, emphasising water boiling and installing warning signage at water access points near Fula. In addition, cross-border surveillance could be intensified to enhance early detection of cases, facilitate timely information sharing, and strengthen coordinated response efforts between neighbouring districts.
Conflict of interest
The authors declare that they have no conflict of interest.
Authors’ contributions
MDN, JW and AN designed the study and contributed to data collection and analysis. PE, BK and GB also contributed to the study design and data collection. MDN led the writing of the bulletin. RM, and BK participated in writing the bulletin and in its review to ensure scientific integrity. All authors contributed to the final draft of the bulletin.
Acknowledgments
The authors would like to thank the Moyo District Health Team and the health workers at Dufile HC IV, Metu HC III, and Otce HC III for their support with medical record review and active case search. We also acknowledge the Health Assistants and Village Health Teams (VHTs) for their invaluable assistance with active case-finding and line listing of cases during this investigation.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- WHO. Cholera Fact Sheet. 2024.
- Azman AS, Rudolph KE, Cummings DA, Lessler J. The incubation period of cholera: a systematic review. Journal of Infection. 2013;66(5):432-8.
- Bwire G, Orach CG, Aceng FL, Arianitwe SE, Matseketse D, Tumusherure E, et al. Refugee settlements and cholera risks in Uganda, 2016–2019. The American Journal of Tropical Medicine and Hygiene. 2021;104(4):1225.
- Almagro-Moreno S, Taylor RK. Cholera: environmental reservoirs and impact on disease transmission. Microbiology spectrum. 2013;1(2):10.1128/microbiolspec. oh-0003-2012.
- Control GTFoC. Ending cholera: a global roadmap to 2030. World Health Organization Geneva, Switzerland; 2017.
- Force GT. <ending-cholera-a-global-roadmap-to-2030 (1).pdf>. 2017.
- Buliva E, Elnossery S, Okwarah P, Tayyab M, Brennan R, Abubakar A. Cholera prevention, control strategies, challenges and World Health Organization initiatives in the Eastern Mediterranean Region: A narrative review. Heliyon. 2023;9(5).
- Monje F, Ario AR, Musewa A, Bainomugisha K, Mirembe BB, Aliddeki DM, et al. A prolonged cholera outbreak caused by drinking contaminated stream water, Kyangwali refugee settlement, Hoima District, Western Uganda: 2018. Infectious Diseases of Poverty. 2020;9(1):154.
- Health Mo. Final Cholera Guidelines. May, 2025.
- Abubakar A, Bwire G, Azman AS, Bouhenia M, Deng LL, Wamala JF, et al. Cholera epidemic in South Sudan and Uganda and need for international collaboration in cholera control. Emerging infectious diseases. 2018;24(5):883.
- World Health Organisation. South Sudan declares cholera outbreak in Renk, Upper Nile State 2024 [Available from: https://www.afro.who.int/countries/south-sudan/news/south-sudan-declares-cholera-outbreak-renk-upper-nile-state.
- Bompangue D, Giraudoux P, Piarroux M, Mutombo G, Shamavu R, Sudre B, et al. Cholera epidemics, war and disasters around Goma and Lake Kivu: an eight-year survey. PLoS neglected tropical diseases. 2009;3(5):e436.
- Piarroux R, Barrais R, Faucher B, Haus R, Piarroux M, Gaudart J, et al. Understanding the cholera epidemic, Haiti. Emerging infectious diseases. 2011;17(7):1161.
- Ali M, Nelson AR, Lopez AL, Sack DA. Updated global burden of cholera in endemic countries. PLoS neglected tropical diseases. 2015;9(6):e0003832.
- Okello PE, Bulage L, Riolexus AA, Kadobera D, Kwesiga B, Kajumbula H, et al. A cholera outbreak caused by drinking contaminated river water, Bulambuli District, Eastern Uganda, March 2016. BMC infectious diseases. 2019;19(1):516.
- Kamukama A, Nuwamanya Y, Namulondo E, Baliruno LN, Kyamwine IB, Nansikombi HT, et al. Cholera outbreak associated with drinking contaminated river water in Kayunga District, Uganda, June-August 2023. BMC Infectious Diseases. 2025;25(1):848.
- Rek J, Orit D, Waako S, Kwesiga B, Migisha R, Bulage L, et al. Cholera outbreak associated with drinking contaminated lake shore water, Namayingo District, Uganda, July–August 2023.
- Swerdlow DL, Greene K, Tauxe R, Wells J, Bean N, Ries A, et al. Waterborne transmission of epidemic cholera in Trujillo, Peru: lessons for a continent at risk. The Lancet. 1992;340(8810):28-32.
Comments are closed.