
Temporal trends and Distribution of measles outbreaks in Uganda, 2020-2025
Authors: Sharon Namasambi*1, Richard Migisha1, Godfrey Biroma2, Deogratius Katongole2, Nasif Matovu1, Benon Kwesiga1, Yasin Nuwamanya2, Fred Nsubuga2 Institutional affiliation: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Uganda National Expanded Program on Immunization, Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256 772 511 067, Email: nabsharon@uniph.go.ug
Summary
Background: The World Health Organization (WHO) recommends ≥95% coverage with two doses of measles–rubella (MR) vaccine to interrupt transmission. However, by 2023, WHO/United Nations Children’s Fund (UNICEF) estimates of national immunization coverage (WUENIC) estimates showed Uganda among countries with MR2 coverage (≤50%) below this target, leaving many children susceptible to measles infection. We described temporal and spatial trends in measles outbreaks to identify persistent high-risk areas and programmatic gaps; to inform targeted outbreak control measures.
Methods: We conducted a descriptive analysis of national measles surveillance and immunization data from January 2020 to December 2025. Data sources included outbreak reports from the National Expanded Program on Immunization, and aggregate MR1/MR2 administrative coverage from District Health Information Software 2. Outbreaks were defined as ≥3 IgM-positive cases within 30 days.We summarised case counts using descriptive statistics, calculated annual percentage changes, and assessed temporal trends with Mann–Kendall tests.
Results: From 2020–2025, 3,192 measles cases were reported, 93% (2,970) of whom had received 1 MR dose, while none had received the full two-dose schedule. Cases increased from 48 (1.5%) in 2021 to 1,967 (61.6%) in 2025, though the trend was not statistically significant (τb=0.733, p=0.060). Overall, 115/146 (78.8%) districts reported ≥1 outbreak, peaking in 2025 (46 districts, 31.5%). MR1 coverage averaged at 92%, while MR2 improved to 64% by 2025 (τb=0.95, p=0.04).
Conclusion: Measles outbreaks persisted during the study period, driven by suboptimal vaccine coverage and resulting immunity gaps among vulnerable populations. Strengthening the second-year-of-life platform and integrating MR2 with co-administered vaccines are essential to close immunity gaps and prevent recurrent outbreaks.
Background
Measles is a highly contagious viral disease transmitted via respiratory droplets, characterized by fever, cough, coryza, conjunctivitis, and a maculopapular rash (1–3). Despite the availability of an effective vaccine for over five decades, measles remains a major global public health concern, particularly in settings with suboptimal immunization coverage (4–6). Achieving ≥95% coverage with two doses of measles–rubella vaccine (MR) is essential for herd immunity and interruption of transmission (7).
Between 2020 and 2025, measles control efforts were undermined by the COVID-19 pandemic, which disrupted routine immunization services worldwide. In 2020 alone, an estimated 22.7 million children missed routine vaccinations; a 19.5% increase from 2019 (8,9), creating what the World Health Organization described as a “perfect storm” for measles outbreaks (10).
Uganda reflects these global challenges. Coverage for first dose of measles-rubella vaccine (MR1) has remained below the 95% elimination threshold, averaging 90% through 2023–2024, while MR2, introduced in 2022, remains suboptimal at approximately 50% coverage by 2024(11). These gaps sustain a large pool of susceptible children, enabling recurrent outbreaks despite localised improvements in MR1 uptake. Additional drivers include cold chain limitations, inequitable access to services in hard-to-reach areas, and delays in outbreak detection (12–15). To inform targeted outbreak control interventions, we analysed temporal and spatial trends in measles outbreaks and assessed immunisation coverage to identify persistent high-risk areas and programmatic gaps.
Methods
We conducted a national descriptive analysis of measles surveillance and immunization data from January 2020 to December 2025 across all 146 districts in Uganda. Data were triangulated from three sources: (1) case-based records of laboratory-confirmed (IgM-positive) measles cases from the Uganda Virus Research Institute (UVRI); (2) Uganda National Expanded Programme on Immunization (UNEPI) surveillance reports to verify outbreak districts and supplement case data; and (3) aggregate MR1 and MR2 administrative coverage from DHIS2.
A measles outbreak was defined per Uganda’s National Technical Guidelines for Integrated Disease Surveillance and Response (3rd Edition) and WHO measles surveillance guidelines as ≥3 laboratory-confirmed (IgM-positive) measles cases within 30 days in the same district or sub-district (16,17).
We summarized cases using descriptive statistics. Annual percentage changes (APCs) were estimated using log-linear regression, and temporal trends assessed using the Mann–Kendall test. Geographic patterns were mapped in QGIS 3.42.1. Coverage of first (MR1) and second dose (MR2) of measles rubella vaccine was compared across outbreak districts to identify high-risk areas.
Permission to analyse the data was obtained from the Uganda Ministry of Health (MoH). In addition, a non-research determination clearance was granted by the U.S. Centers for Disease Control and Prevention (CDC). The investigation was conducted in accordance with applicable U.S. federal regulations governing public health surveillance and data protection (see, for example, 45 C.F.R. part 46; 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.). Further authorization was obtained from the Uganda National Expanded Programme on Immunization (UNEPI) for access to vaccination and surveillance data. As this analysis involved routine program and surveillance data and posed no more than minimal risk to participants, written informed consent was not required. All data were anonymized before analysis, and strict measures were implemented to maintain privacy, confidentiality, and data security throughout the data abstraction and analysis process.
Results
National burden and temporal trends of measles cases, 2020–2025
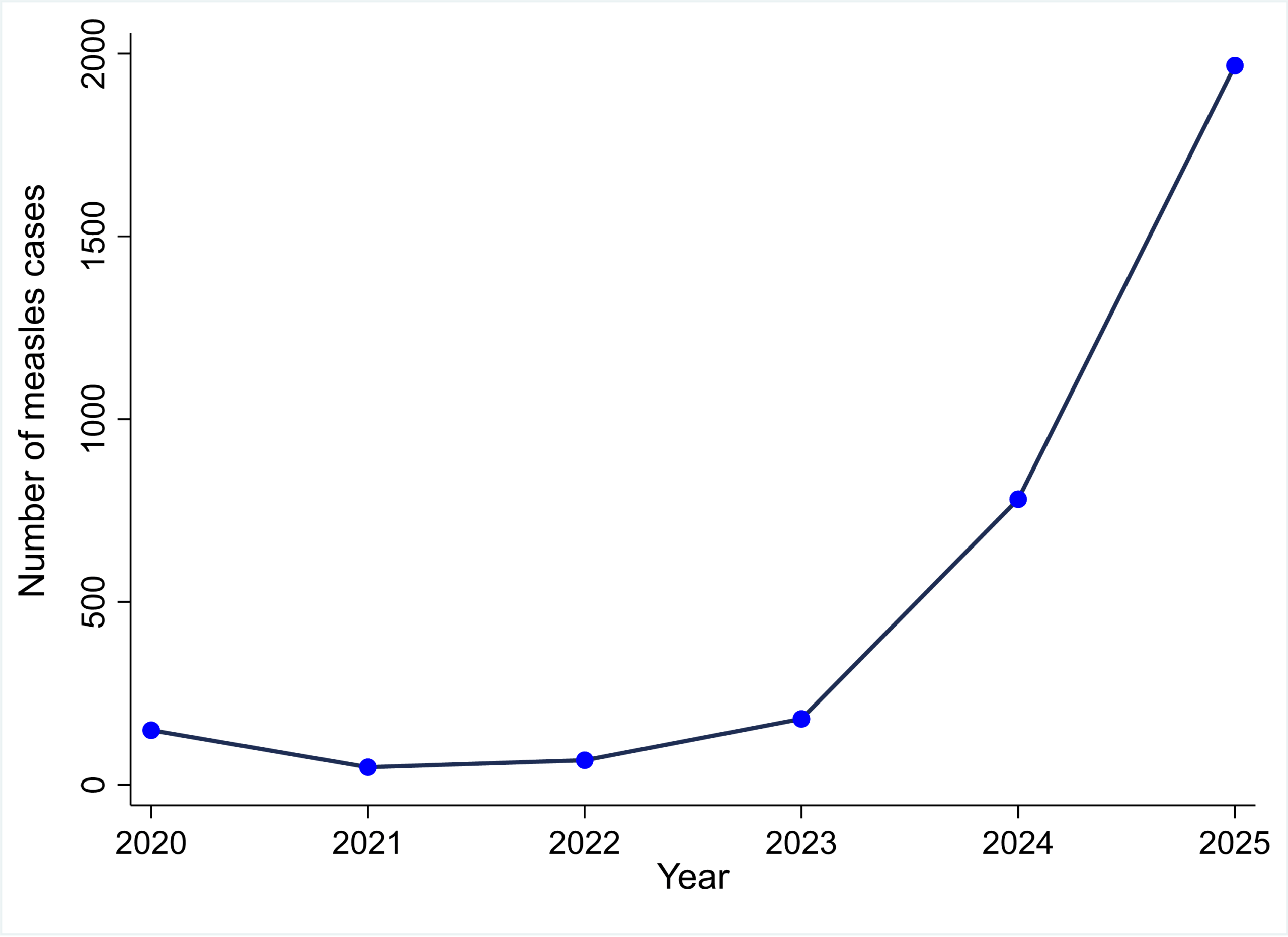
Between 2020 and 2025, Uganda reported 3,192 measles cases, of which 2,970 (93%) had received 1 MR dose, while none had received the full two-dose schedule Annual cases varied markedly, from 48 (1.5%) in 2021 to 1,967 (61.6%) in 2025. Although an overall upward trend was observed (τb=0.73, p=0.060), it was not statistically significant (Figure 1). Year-to-year changes were highly variable, with sharp increases in 2024 (APC=+334%) and 2025 (APC=+152%) following a decline in 2021 (APC=−68%) (Figure 1).
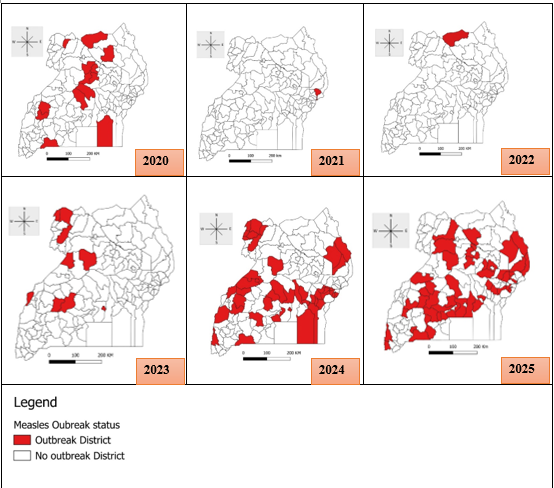
Spatial distribution and trends confirmed measles outbreaks across districts, Uganda, 2020–2025
Overall, 115/146 (78.8%) districts reported ≥1 confirmed outbreak. The number of affected districts fluctuated widely, from 13 (8.9%) in 2020 to a low of 1 (0.7%) in 2021–2022, before rising sharply to 45 (30.8%) in 2024 and 46 (31.5%) in 2025 (τb=0.55, p=0.181). Twenty-two districts experienced recurrent outbreaks, including Buvuma, Isingiro, Jinja, Kamwenge, Kiryandongo, Mbale, Manafwa, Kikuube, Butaleja, Kakumiro, Mpigi, Moroto, Napak, Nakaseke, Kanungu, Namutumba, Lamwo, Kampala, Koboko, Madi-Okollo, Yumbe, and Sembabule during the study period (Figure 2).
Spatial overlay of Measles-Rubella vaccination coverage by outbreak districts, Uganda, 2020–2025
Over the six-year period, MR1 coverage averaged at 92%, while MR2 coverage, introduced in 2022, statistically increased from low baseline (22%) to 64% by 2025 (τb=0.95, p=0.04). Spatial overlay analysis showed that outbreaks occurred across all coverage categories, including districts with MR1 coverage ≥95% (Figure 3).
Discussion
Our analysis demonstrates persistent measles transmission in Uganda from 2020 to 2025, marked by a 40-fold increase in cases, spread to 78.8% of districts, and ongoing immunity gaps driven by suboptimal vaccination coverage. The rise from a single outbreak-affected district in 2021 to 46 districts in 2025 suggests sustained local transmission rather than isolated importations. This pattern aligns with global post-COVID-19 trends, where disruptions in routine immunization created susceptible cohorts, resulting in explosive outbreaks upon measles reintroduction (8,9,18).
That 93% of cases had received at least one MR dose may seem paradoxical but reflects the limitations of a single-dose schedule. With 5–10% primary vaccine failure and ~5% secondary failure due to waning immunity (19–22) , 10–15% of children remain susceptible even in a population with 92% MR1 coverage. This highlights the critical role of routine MR2 in addressing primary vaccine failures and boosting immunity, a strategy proven effective in global measles elimination efforts (23).
Outbreaks in districts reporting ≥95% MR1 coverage can be explained by two factors: (1) administrative coverage often overestimates true immunity due to inaccurate denominators, inflating coverage by 10–20% (24); and (2) 5–10% of vaccinated children fail to develop protective immunity (19,20). Although MR2 coverage improved to 64% by 2025, systemic challenges remain.
Study limitations: Administrative coverage data from DHIS2 may not reflect true immunity due to inaccurate denominators, unregistered children, or incomplete reporting. We focused on temporal trends and relative changes rather than absolute coverage, reducing sensitivity to systematic errors.
Conclusion
Measles persisted in Uganda from 2020 to 2025 due to suboptimal vaccine coverage, leaving many children vulnerable. Strengthening the second-year-of-life platform by integrating MR2 with routine child health services, along with targeted follow-up, could close immunity gaps, achieve ≥95% MR coverage, and advance measles elimination efforts in Uganda.
Conflicts of interest: The authors declared no conflicts of interest.
Acknowledgements: We acknowledge the Uganda National Expanded Programme on Immunization, Uganda Virus Research Institute, and Ministry of Health Division of Health Information for data access and technical support. We thank district health teams for their commitment to measles surveillance and outbreak response.
Author contributions: SN conceptualized the study and led data collection, analysis, and writing. RM, and BK, provided technical supervision and Bulletin review. GB, DK, NM, MDN, YN, and FN supported data analysis, and report writing. All authors approved the final version.
Copyright: Materials in the Uganda Public Health Bulletin are public domain and may be reproduced with appropriate citation.
References
- Jalal MA, Halboot KM, Lami SA, Gumar EA, al-Delphi MHK, Lami F, et al. Epidemiological trends and clinical characteristics of measles in Iraq (2023–2024): a retrospective cross-sectional study. BMC Infect Dis. 2025 Apr 9;25(1):487. doi:10.1186/s12879-025-10904-8
- Kulsoom S, Soomro S, Junejo S, Anjum M, Waseem H, Akram M. Clinical Presentation, Complications and Outcome of Measles in Pediatric Population at Tertiary Care Hospital: Measles in Pediatric Population. Pak J Health Sci. 2023 Mar 31;50–3. doi:10.54393/pjhs.v4i03.624
- CDC. Measles (Rubeola) [Internet]. 2025 [cited 2025 Nov 8]. Measles (Rubeola). Available from: https://www.cdc.gov/measles/index.html
- Measles [Internet]. [cited 2025 Nov 8]. Available from: https://www.who.int/news-room/fact-sheets/detail/measles
- Minta AA, Ferrari M, Antoni S, Lambert B, Sayi TS, Hsu CH, et al. Progress Toward Measles Elimination — Worldwide, 2000–2023. Vol. 73. 2024;73(45).
- Minta AA, Ferrari M, Antoni S, Portnoy A, Sbarra A, Lambert B, et al. Progress Toward Measles Elimination — Worldwide, 2000–2022. Morb Mortal Wkly Rep. 2023 Nov 17;72(46):1262–8. doi:10.15585/mmwr.mm7246a3 PubMed PMID: 37971951; PubMed Central PMCID: PMC10684353.
- Do LAH, Mulholland K. Measles 2025. N Engl J Med. 0(0). doi:10.1056/NEJMra2504516
- Packham A, Taylor AE, Karangwa MP, Sherry E, Muvunyi C, Green CA. Measles Vaccine Coverage and Disease Outbreaks: A Systematic Review of the Early Impact of COVID-19 in Low and Lower-Middle Income Countries. Int J Public Health. 2024 Apr 25;69:1606997. doi:10.3389/ijph.2024.1606997
- World Health Organisation. Progresses and Challenges with Sustaining and Advancing Immunization Coverage During the COVID-19 Pandemic [Internet]. 2023 [cited 2025 Nov 8]. Available from: https://www.who.int/publications/i/item/progresses-and-challenges-with-sustaining-and-advancing-immunization-coverage-during-the-covid-19-pandemic
- UNICEF and WHO warn of perfect storm of conditions for measles outbreaks, affecting children [Internet]. [cited 2025 Nov 8]. Available from: https://www.who.int/news/item/27-04-2022-unicef-and-who-warn-of–perfect-storm–of-conditions-for-measles-outbreaks–affecting-children
- WHO/UNICEF estimates of national immunization coverage [Internet]. [cited 2026 Feb 13]. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage
- Nsubuga EJ, Morukileng J, Namayanja J, Kadobera D, Nsubuga F, Kyamwine IB, et al. Measles outbreak in Semuto Subcounty, Nakaseke District, Uganda, June–August 2021. IJID Reg. 2022 Dec;5:44–50. doi:10.1016/j.ijregi.2022.08.017
- Okiror EO, Ampaire I, Nsubuga F, Kwizera P, Okello PE, Migisha R, et al. Measles outbreak with children below the recommended age for first dose of measles vaccine most affected in Kakumiro District, February–May 2024. Vol. 9. 2024;9(3).
- Mfitundinda E, Migisha R, Namusisi AM, Wenani D, Kwesiga B, Ayeerwot R, et al. Investigation of a cross-border measles outbreak in Moroto District, northeastern Uganda, March–September, 2024. Discov Public Health. 2025 May 16;22(1):267. doi:10.1186/s12982-025-00581-y
- Namusisi AM, Nuwamanya Y, Migisha R, Atugonza R, Immaculate A, Nsubuga F, et al. Measles outbreak Investigation in Terego District, Uganda, May- June, 2024. Vol. 9. 2024;9(3).
- World Health Organization WH. Measles outbreak guide. World Health Organization; 2022. 96 p.
- Ministry of Health. Uganda 3rd IDSR Tech Guideline_PrintVersion_10Sep2021.pd [Document] [Internet]. Ministry of Health; 2021. Available from: https://www.afro.who.int/sites/default/files/2021-09/2_Uganda%203rd%20IDSR%20Tech%20Guideline_PrintVersion_10Sep2021.pdf
- Cardoso Pinto AM, Ranasinghe L, Dodd PJ, Budhathoki SS, Seddon JA, Whittaker E. Disruptions to routine childhood vaccinations in low-and middle-income countries during the COVID-19 pandemic: A systematic review. Front Pediatr. 2022;10:979769.
- Hickman CJ, Hyde TB, Sowers SB, Mercader S, McGrew M, Williams NJ, et al. Laboratory Characterization of Measles Virus Infection in Previously Vaccinated and Unvaccinated Individuals. J Infect Dis. 2011 Jul 1;204(suppl_1):S549–58. doi:10.1093/infdis/jir106
- Kontio M, Jokinen S, Paunio M, Peltola H, Davidkin I. Waning Antibody Levels and Avidity: Implications for MMR Vaccine-Induced Protection. J Infect Dis. 2012 Nov 15;206(10):1542–8. doi:10.1093/infdis/jis568
- Patel MK, Dumolard L, Nedelec Y, Sodha SV, Steulet C, Gacic-Dobo M, et al. Progress Toward Regional Measles Elimination — Worldwide, 2000–2018. Morb Mortal Wkly Rep. 2019 Dec 6;68(48):1105–11. doi:10.15585/mmwr.mm6848a1 PubMed PMID: 31805033; PubMed Central PMCID: PMC6897527.
- Weldegebriel GG, Gasasira A, Harvey P, Masresha B, Goodson JL, Pate MA, et al. Measles Resurgence Following a Nationwide Measles Vaccination Campaign in Nigeria, 2005–2008. J Infect Dis. 2011 Jul 1;204(suppl_1):S226–31. doi:10.1093/infdis/jir136
- World Health Organization. Measles vaccines: WHO position paper, April 2017 – Recommendations. Vaccine. 2019 Jan 7;37(2):219–22. doi:10.1016/j.vaccine.2017.07.066
- Wariri O, Edem B, Nkereuwem E, Nkereuwem OO, Umeh G, Clark E, et al. Tracking coverage, dropout and multidimensional equity gaps in immunisation systems in West Africa, 2000–2017. BMJ Glob Health. 2019 Sep 6;4(5). doi:10.1136/bmjgh-2019-001713 PubMed PMID: 10.1136/bmjgh-2019-001713.
Comments are closed.