
District Leader Community Dialogue Meetings Improved Willingness to Receive COVID-19 Vaccines in Western Uganda, May 2021: A Pre-Post Study
Authors: Edirisa Juniour Nsubuga1, Arthur G. Fitzmaurice2, Allan Komakech1, Tom Dias Odoi3, Daniel Kadobera1,4, Lilian Bulage1,4, Benon Kwesiga1,4, Peter James Elyanu3, Alex Riolexus Ario1,4, Julie Harris2__ Institutional Affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda, 2United States Centers for Disease Control and Prevention, Kampala, Uganda, 3Baylor College of Medicine Children’s Foundation Uganda, Kampala, Uganda, 4Uganda National Institute of Public Health, Kampala, Uganda__ *Corresponding author: Email: nsubugaeddiej@musph.ac.ug, Tel: +256704131375
Summary
Background: Widespread COVID-19 vaccine uptake is necessary for epidemic control. A February 2021 study in Uganda suggested that public uptake would follow uptake among leaders. In May 2021, Baylor Uganda convened and led community dialogue meetings with district leaders from Western Uganda to promote vaccine uptake among leaders. We assessed the effect of the meetings on willingness towards COVID-19 vaccine uptake. Methods: All departmental district leaders, including health, education, security, engineering, and finance of the 17 districts in Western Uganda, were invited to the meetings, which lasted approximately four hours. Scripts were used, and the same topics were discussed in all meetings. Leaders completed self-administered questionnaires before and after the meetings. We used a five-point Likert scale to assess willingness to receive the vaccine. We analyzed the findings using Wilcoxon’s signed-rank test. Results: Among 268 attendees, 164 (61%) completed the pre- and post-meeting assessments; 48 (18%) had already been vaccinated, and 56 (21%) declined due to time constraints. Among the 164, the median scores for willingness to receive the vaccine changed from three (neutral) pre-meeting to five (strong willingness) post-meeting (p<0.0005). Conclusion: Dialogue meetings led to district leaders’ increased willingness to receive the COVID-19 vaccine. The information dissemination, interactive discussions, and the influence of trusted health experts may have led to the changes observed post-meeting. Broader use of such meetings with community leaders could reduce COVID-19 vaccine hesitancy and increase uptake.
Introduction
The Uganda Ministry of Health (MOH) began the deployment of vaccination against SARS-CoV-2 in March 2021. Vaccination was offered to prioritized subpopulations, which included health workers, teachers, adults with comorbidities, and the elderly (1). With the lack of a proven effective treatment against COVID-19 at the time, the vaccine was an essential additional measure to the existing standard operating procedures (e.g., use face masks, hand washing, and social distancing) to prevent COVID-19 spread (2-4). Widespread vaccine uptake is necessary for epidemic control (5). However, polls conducted worldwide showed that many people expressed hesitancy about receiving the COVID-19 vaccine (6). As a result, there was a need to identify behavior change methods that could effectively lead to increased COVID-19 vaccine uptake (2, 7). Community dialogue meetings are one method that can promote awareness and behavior change.
Uganda has faced a low level of uptake of new vaccines, such as the Human Papilloma Virus, which targeted girls aged 9–14 years in Uganda beginning in 2015 (8). Even after its use in the country for six years, its coverage was still low, partly due to negative media reporting (9) and the poor public attitude towards the vaccine, such as the perceived feeling that the vaccine had severe side effects (8). Even vaccines used in the country for a long time, such as the Diphtheria, Pertussis, and Tetanus-Hepatitis b-Hemophilus influenza type b (DPT-Hep-Hib) vaccines, still faced challenges with uptake due to misconceptions (9). Additionally, there was public distrust about the new vaccines due to a feeling that Africans were being used as “experimental specimens” (9).
As of May 1, 2021, the cumulative number of COVID-19 cases in Uganda stood at 41,975 cases, 13 months after Uganda reported its first case (10, 11). We suspected that due to the few cases at the time, many did not take COVID-19 seriously, which affected their perception and attitudes towards receiving the COVID-19 vaccines. These negative attitudes contributed to COVID-19 vaccine hesitancy at the time, with only 354,736 eligible people vaccinated as of May 1, 2021, nearly two months after COVID-19 vaccination was introduced in Uganda, despite the availability of free COVID-19 vaccines (12). A February 2021 study in Uganda suggested that public uptake of COVID-19 vaccines would follow the uptake of vaccines among leaders (13). In May 2021, community dialogue meetings were held with Baylor Uganda and district leaders from Western Uganda as a way of reducing COVID-19 vaccine hesitancy and promoting the uptake of COVID-19 vaccines among district leaders and their communities. However, it was not known whether these meetings would change participants’ attitudes about COVID-19 vaccination. Therefore, we assessed the effects of the meetings on district leaders’ COVID-19 risk perception, COVID-19 vaccine concerns, perceived vaccine benefits, perceived vaccine access, and willingness to receive the vaccine.
Methods
Study setting
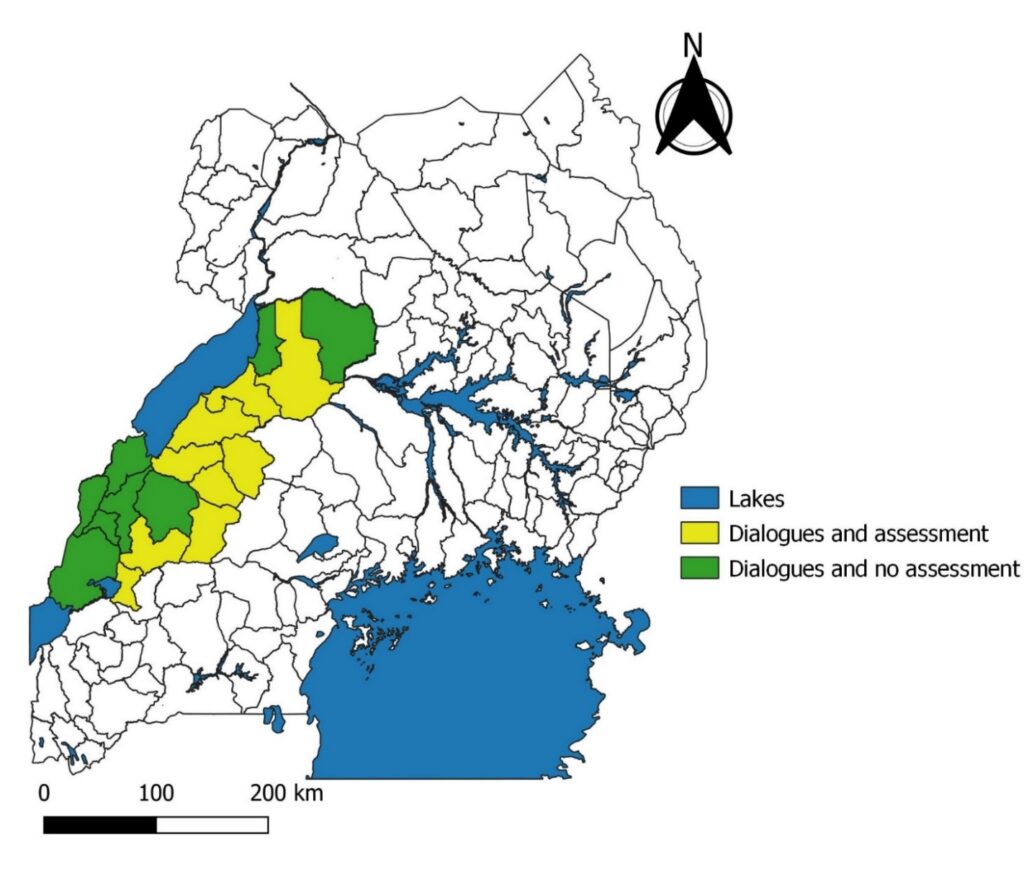
We conducted the evaluation in 17 districts of Western Uganda (Figure 1). Of the 41,975 COVID-19 cases reported nationally by May 1, 2021, 2,305 (6%) were reported in 17 districts—1,430 (3%) from the Tooro Region (Bundibugyo, Bunyangabu, Kabarole, Kamwenge, Kasese, Kitagwenda, Kyegegwa, Kyenjojo, and Ntoroko districts) and 875 (2%) from the Bunyoro Region (Buliisa, Hoima, Kagadi, Kakumiro, Kibale, Kikube, Kiryandongo, and Masindi districts) (11). Despite the availability of free COVID-19 vaccines at the time, the 17 districts had low vaccine uptake, with only 20,358 (25%) vaccinated out of a total of 81,430 eligible people who were supposed to have been vaccinated by May 1, 2021 (12).
Study design
We conducted a pre-post evaluation study, through which we assessed district leaders’ willingness to receive the COVID-19 vaccine before and after the community dialogue meetings conducted by Baylor Uganda in May 2021. Scripts were used to lead the dialogues, and the same topics were discussed at all meetings.
Community dialogue description
Community dialogue is a forum that brings together people from different sections of society and creates an opportunity for exchanging ideas, information, and perspectives, clarifying viewpoints, and developing solutions to issues of interest to society (14-16). District leaders were invited because it was demonstrated in several studies that they can play vital roles in supporting or opposing health service utilization through the mobilization of community members (17-19). Dialogue participants included political, technical, cultural, and religious leaders.
The political leaders consisted of the District Local Council V (LC V) chairpersons, secretaries for health, councilors, and Resident District Commissioners (RDCs). Technical district leaders included Chief Administrative Officers (CAOs) and district heads of departments such as health, education, planning, production, works, administration, human resources, and finance. District religious leaders from all prevalent faiths in Uganda—including but not limited to Catholics, Anglicans, and Muslims—and cultural leaders were also invited.
One community dialogue meeting was held in each of the 17 districts, and 14–21 district leaders from each district participated in the meetings. The number of district leaders who participated in the dialogue meetings depended on their availability at the time of the meetings. A total of 268 district leaders from nine districts participated in the meetings and were invited to participate in the evaluation assessment (Figure 1). On average, each meeting lasted approximately four hours.
After arrival and registration, participants completed the pre-meeting assessment questionnaire, followed by opening prayers, self-introductions, brief remarks by Baylor Uganda staff, and opening remarks by District Health Officers (DHOs). Meetings were chaired by District Health Educators (DHEs) who made brief presentations on frequently asked questions about COVID-19 vaccines. Among the issues that the DHEs talked about were general COVID-19 information (what it is, signs and symptoms, who is at risk, how one can be protected from contracting it), the types and availability of different COVID-19 vaccines in circulation, how the vaccines work, how they were developed, and why they were developed in a short time.
The DHEs also talked about COVID-19 vaccines in Uganda—which type are given to Ugandans, why, who is eligible to receive those vaccines, and why they are eligible. Other topics included vaccine availability, administration, safety, effectiveness, common side effects, risks of serious reactions, and how to deal with them.
After their presentations, DHEs allowed participants to ask questions, raise points of concern, and answer each other from their different views of understanding. This was under the guidance of DHEs and other technical professionals, such as DHOs and Assistant DHOs, who were present in the meetings. After issues and concerns about the vaccines were discussed to every participant’s satisfaction, DHEs summarized key messages and closed the meetings.
Closing activities included the development of an action plan on how each participant would disseminate the information they received from the meeting to the community to promote vaccine uptake. Each leader was invited to complete the same evaluation questionnaire that was administered at the beginning of the meeting.
Questionnaire
The self-administered questionnaire consisted of information on sociodemographic factors and willingness to receive a COVID-19 vaccine. For the five-point Likert scale questions, participants indicated 1 strongly disagree, 2 disagree, 3 neither disagree nor agree, 4 agree, or 5 strongly agree.
The assessment was performed based on three of the most prominent health behavior theory constructs—the health belief model (20), the theory of planned behavior (21), and the extended parallel process model (22). We used these theories to assess COVID-19 risk perception, vaccine concerns, perceived vaccine benefits, perceived vaccine access, and willingness to receive a COVID-19 vaccine.
Study variables
In the questionnaire, we asked about sociodemographic factors, including highest education level attained, presence of children younger than five years old at home, presence of elderly 60 years or older at home, and district of work. We asked four questions on willingness to receive a COVID-19 vaccine. We constructed a composite score by summing scores from the four questions.
Data analysis
We analyzed the data using STATA version 14.0. We described sociodemographic factors using frequencies and percentages. Likert scale data were ordinal and not normally distributed when tested for normality using the Shapiro–Wilk tests, so we used the non-parametric Wilcoxon signed-rank test to assess differences between pre- and post-dialogue scores for each question (23, 24). We used Wilcoxon’s signed-rank test instead of the sign test because it has more statistical power (25). Wilcoxon’s signed-rank test ranks the degree of change between the paired scores in addition to considering the degree of change measured by the sign test, providing more information for analysis (25).
To calculate the magnitude of the effect of the community dialogue meetings on willingness to receive the COVID-19 vaccines, we used Cliff’s delta measure (Cliff’s dominance measure), which is the accepted measure of effect size for the Wilcoxon signed-rank test (26, 27), to calculate the effect sizes (r) of the changes (28). It is obtained by subtracting the ratio of the negative rank-sum to the total rank-sum from that of the positive rank-sum to the total rank-sum (29, 30). The effect size ranges from 0 to 1, with 0 indicating that the groups are statistically equal and 1 implying that one group significantly dominates (29, 30). We graded the effect size as small effect (r=0.1-0.3), medium effect (r=0.4-0.5), and large effect (r=0.6-1.0) for both positive and negative changes (28).
As part of the analysis, we reported median frequencies, percentages, and first and third quartiles, which we used to calculate interquartile ranges (IQRs) for both pre- and post-meeting assessments. We defined significance as p≤0.05. We also performed logistic regression to assess whether COVID-19 vaccine willingness was associated with the presence of children younger than five years old or elderly persons 60 years or older at home.
Ethical considerations
This assessment was in response to a public health emergency. The Ministry of Health gave the directive and approval to evaluate the effect of the dialogue meetings on the leader’s willingness and intention to receive COVID-19 vaccines. The Office of the Associate Director for Science, CDC/Uganda, also determined that this activity was not human subject research. Its primary intent was public health practice and epidemic disease control. Written informed consent was sought from the respondents. All respondents were informed that their participation was voluntary and that their refusal would not result in any negative consequences. To protect the confidentiality of the respondents, each was assigned a unique identifier.
Results
Final evaluation sample size
Among the 268 community dialogue meeting attendees, 164 (61%) filled out both pre- and post-meeting assessments. Forty-eight (18%) who had already been vaccinated and 56 (21%) who completed only the pre-meeting assessment due to time constraints were excluded from the analysis.
Sociodemographic characteristics of community dialogue participants
In total, 150 (92%) of the 164 district leaders who participated in the study had attained either a tertiary or university education; the rest had attained secondary or primary education. Most (118, 72%) were men. The districts with the highest numbers of participants were Kikube (21, 13%), Kibale (20, 12%), and Hoima (20, 12%); Kyegegwa had the fewest participants (14, 8.0%) (Table 1).
Table 1: Sociodemographic characteristics of community dialogue participants, Western Uganda, May 2021 (N=164)
| Variable | Frequency (n) | Percent (%) | |
| Education | |||
| Primary | 2 | 1 | |
| Secondary | 12 | 7 | |
| Tertiary/University | 150 | 92 | |
| Having children <5 years old in the household | |||
| No | 56 | 34 | |
| Yes | 108 | 66 | |
| Having elderly ≥60 years old in the household | |||
| No | 114 | 70 | |
| Yes | 50 | 30 | |
| Sex | |||
| Female | 46 | 28 | |
| Male | 118 | 72 | |
| A frontline worker during COVID-19 response* | |||
| No | 48 | 29 | |
| Yes | 116 | 71 | |
| Districts | |||
| Hoima | 20 | 12 | |
| Kagadi | 18 | 11 | |
| Kakumiro | 16 | 10 | |
| Kamwenge | 16 | 10 | |
| Kibaale | 20 | 12 | |
| Kikuube | 21 | 13 | |
| Kitagwenda | 18 | 11 | |
| Kyegegwa | 14 | 8 | |
| Masindi | 21 | 13 | |
* A frontline worker who worked during the COVID-19 response, e.g., a health worker and a COVID-19 district task force member
Willingness to receive the COVID-19 vaccine
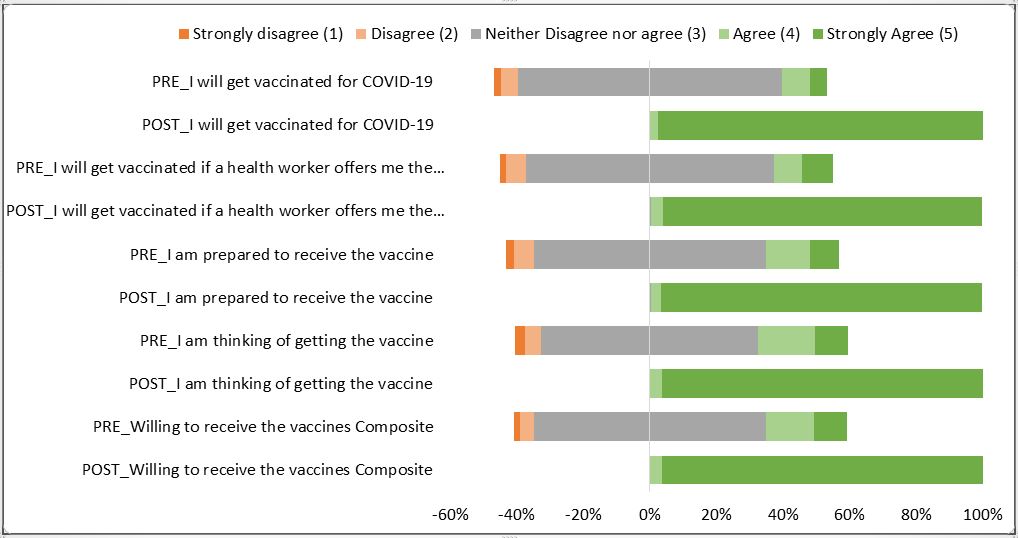
Before the meetings, 114 (70%) district leaders neither agreed nor disagreed (median: 3, IQR: 3,3) that they were willing to receive the COVID-19 vaccines. After the meetings, 158 (96%) leaders strongly agreed (median: 5; IQR: 5,5) that they were willing to receive the vaccine. This change was statistically significant (p<0.0005, r=0.995) (Table 2, Figure 2).
Table 2: Effect of community dialogue meetings on district leaders’ willingness to receive the COVID-19 vaccine, Western Uganda, May 2021 (N=164)
| Variable | Pre-dialogue assessment | Post-dialogue assessment | p-value | Effect Size (r) | |||||
| Median | Median | ||||||||
| n | % | IQR | n | % | (IQR) | ||||
| Willingness to receive COVID-19 vaccines | 114 | 70 | 3 (3,3) | 158 | 96 | 5 (5,5) | <0.0005* | 0.995 | |
| I am thinking of getting the vaccine | 107 | 65 | 3 (3,4) | 158 | 96 | 5 (5,5) | <0.0005* | 1.000 | |
| I am prepared to receive the vaccine | 114 | 70 | 3 (3,3) | 158 | 96 | 5 (5,5) | <0.001* | 1.000 | |
| I will get vaccinated if a health worker offers me the vaccine | 122 | 74 | 3 (3,3) | 157 | 96 | 5 (5,5) | <0.0005* | 0.993 | |
| I will get vaccinated for COVID-19 | 122 | 74 | 3 (3,3) | 160 | 98 | 5 (5,5) | <0.0005* | 0.996 | |
Median IQR of 1=strongly disagree, 2=disagree, 3=neither disagree nor agree, 4=agree, or 5=strongly agree. * Significant association at p-value < 0.05
Discussion
Based on 164 district leaders completing pre- and post-meeting questionnaires, community dialogue meetings led to increased willingness and intention to receive COVID-19 vaccines. District leaders’ willingness to receive the COVID-19 vaccines increased after the meetings as they were provided with information on the safety and side effects of the vaccines. Information dissemination, interactive discussion (individual questions and concerns being answered or addressed to the satisfaction of the participants), and the personal influence of trust in experts instead of mere risk communication materials led to the changes we observed in post-meeting assessments.
The discursive nature of the meetings among the leaders themselves and between the leaders and facilitators might have led to an improvement in their willingness to receive the COVID-19 vaccines. It was shown that learning environments that provide learners with more understanding, richer and more realistic contexts, and dialogic dimensions can be persuasive and lead to eventual behavior change (31). As leaders learned more information, they asked more questions, which, when answered, might have led to improvement in their willingness to receive the vaccine.
Our findings are in line with Bandura’s argument that the type of learning environment and teaching method can improve the self-efficacy of individuals (32). Similar findings were also reported by Fenci and Scheel, who found that a question-and-answer format of learning can create a positive climate that engages participants, thereby leading to improved self-efficacy towards adopting a given behavior (33).
During these meetings, district medical experts supported the uptake of the vaccines and explained and answered the questions raised by the meeting participants to their satisfaction. Since these medical experts are trusted and have at times been involved in the treatment of the district leaders, this might have influenced the changes in willingness to receive the vaccine observed after the meetings. Findings from this study are consistent with findings from other studies that showed that trust in experts improved acceptance of vaccines and reduced anti-vaccination sentiments and that effective policymaking depended on trust in the experts (34, 35).
The improvements in district leaders’ willingness and intention to receive the COVID-19 vaccines may have been due to peer influence. If leaders influence each other, this implies that leaders will also be more likely than risk communication materials alone to influence other community members. Targeted community health education with the opportunity for discussion can be a vital tool to improve attitudes towards the COVID-19 vaccine. This is consistent with several studies that found community health education to be one of the most effective methods of increasing community willingness to receive vaccines (36-38).
Study limitations
Although we report changes in participants’ willingness to receive the COVID-19 vaccines, we do not know if the theoretical changes eventually led to vaccine uptake. District leaders may have overreported their willingness to receive the COVID-19 vaccine after the meeting due to social desirability. Participants could provide proof of vaccination, but that is beyond the scope of the dialogues.
Conclusion
The 17 community leader dialogue meetings reported here led to district leaders’ increased willingness to receive the COVID-19 vaccine. These improvements might influence public uptake of the COVID-19 vaccines if leaders get vaccinated and publicly share their vaccination status and what they learned during dialogue meetings. The information dissemination, interactive discussions, and the influence of trusted health experts may have led to the changes observed after the meetings. Broader use of such meetings with community leaders could reduce COVID-19 vaccine hesitancy and increase uptake. We recommend the broader use of such meetings to bring together health authorities and other community leaders as a way of reducing COVID-19 vaccine hesitancy and increasing uptake. Scaling up community dialogue meetings in the form of public town hall meetings to involve community members might also have the same effect.
Acknowledgements
The authors would like to thank the district leaders who spared time to participate in the pre-post meeting assessments out of their very busy schedules. Last but not least, our deepest gratitude goes to the administration of Baylor Uganda for allowing us to carry out this study even when it was inconvenient for their meeting participants.
References
- MOH. UGANDA LAUNCHES THE COVID-19 VACCINATION CAMPAIGN. Ministry of Health, Uganda; 2021.
- Chu H, Liu S. Integrating health behavior theories to predict Americans’ intention to receive a COVID-19 vaccine. Patient education and counseling. 2021.
- CDC. Ten great public health achievements–the United States, 2001-2010. MMWR Morbidity and mortality weekly report. 2011;60(19):619-23.
- Schoch-Spana M, Brunson EK, Long R, Ruth A, Ravi SJ, Trotochaud M, et al. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine. 2020.
- Betsch C, Böhm R, Korn L, Holtmann C. On the benefits of explaining herd immunity in vaccine advocacy. Nature human behavior. 2017;1(3):1-6.
- Tyson A, Johnson C, Divided CFUPN. over Whether to Get COVID-19 Vaccine Concerns about the safety and effectiveness of the possible vaccine, the pace of approval process. 2020.
- Zhang KC, Fang Y, Cao H, Chen H, Hu T, Chen Y, et al. Behavioral Intention to Receive a COVID-19 Vaccination Among Chinese Factory Workers: Cross-sectional Online Survey. Journal of medical Internet research. 2021;23(3):e24673.
- Isabirye A, Mbonye M, Asiimwe JB, Kwagala B. Factors associated with HPV vaccination uptake in Uganda: a multi-level analysis. BMC Women’s Health. 2020;20(1):1-11.
- IDRC. EVALUATION OF THE DRIVERS OF URBAN IMMUNISATION IN UGANDA: A CASE STUDY OF KAMPALA CITY. 2020. Kampala: IDRC and Makerere University; 2020.
- COVID-19 DAILY SITUATION REPORT [Internet]. Ministry of Health Uganda. 2021 [cited 11 May 2021]. Available from: https://veoci.com/veoci/p/w/f/4kt8iduidn4unwe4/Ug_COVID-19_SitRep%23410.pdf
- COVID-19 RESPONSE INFO HUB [Internet]. Ministry of Health Uganda. 2020 [cited 11 May 2021]. Available from: https://covid19.gou.go.ug/timeline.html.
- MINISTRY OF HEALTH – UGANDA NATIONAL EXPANDED PROGRAM ON IMMUNISATION UPDATES ON COVID-19 VACCINATION CAMPAIGN: COVID Vaccination Situation Update – Issue 25, as of 1st May 2021 [Internet]. Ministry of Health Uganda. 2021 [cited 12 May 2021]. Available from: https://veoci.com/veoci/p/w/f/lwe3ryeyfvvheppy/Ug_COVID-19_Vaccination_Update%2325.pdf
- IANPHI. How African National Public Health Institutes Can Address COVID-19 Vaccine Misinformation: The International Association of National Public Health Institutes; 2021 [Available from: https://ianphi.org/news/2021/webinar-covid-19-africa.html.
- McGee-Cooper A, Trammell D. Servant Leadership Learning Communities®. Servant Leadership: Springer; 2010. p. 130-44.
- Umbreit M, Armour MP. Restorative justice dialogue: An essential guide for research and practice: Springer publishing company; 2010.
- Isaacs WN. Taking flight: Dialogue, collective thinking, and organizational learning. Organizational dynamics. 1993;22(2):24-39.
- Walsh A, Matthews A, Manda-Taylor L, Brugha R, Mwale D, Phiri T, et al. The role of the traditional leader in implementing maternal, newborn, and child health policy in Malawi. Health policy and planning. 2018;33(8):879-87.
- Rosen B, Goodson P. A Recommendation to Use the Diffusion of Innovations Theory to Understand School Nurses’ Role in HPV Vaccine Uptake. International Quarterly of Community Health Education. 2014;34(1):37-49.
- Karan A, Hartford E, Coates TJ. The potential for political leadership in HIV/AIDS communication campaigns in Sub-Saharan Africa. Global Health Action. 2017;10(1):1270525.
- Becker MH. The health belief model and sick role behavior. Health education monographs. 1974;2(4):409-19.
- Azjen I. Understanding attitudes and predicting social behavior. Englewood Cliffs. 1980.
- Witte K. Fear control and danger control: A test of the extended parallel process model (EPPM). Communications Monographs. 1994;61(2):113-34.
- Jamieson S. Likert scales: How to (ab) use them? Medical education. 2004;38(12):1217-8.
- Sullivan GM, Artino Jr AR. Analyzing and interpreting data from Likert-type scales. Journal of graduate medical education. 2013;5(4):541.
- Nahm FS. Nonparametric statistical tests for the continuous data: the basic concept and the practical use. Korean Journal of anesthesiology. 2016;69(1):8.
- Grissom RJ, Kim JJ. Effect sizes for research: Univariate and multivariate applications: Routledge; 2012.
- Samples TI. Nonparametric Effect Size Estimators.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale. Erlbaum. Conner, BE (1988). The Box in the Barn. Columbus: Highlights for …; 1988.
- Glass GV. Note on rank biserial correlation. Educational and Psychological Measurement. 1966;26(3):623-31.
- Kerby DS. The simple difference formula: An approach to teaching nonparametric correlation. Comprehensive Psychology. 2014;3:11. IT. 3.1.
- Petraglia J. The importance of being authentic: Persuasion, narration, and dialogue in health communication and education. Health communication. 2009;24(2):176-85.
- Bandura A. Self-Efficacy: The Exercise of Control. The British Journal of Clinical Psychology. 1997;37(4):470.
- Fencl H, Scheel K. Engaging students. Journal of College Science Teaching. 2005;35(1):20.
- Cairney P, Wellstead A. COVID-19: effective policymaking depends on trust in experts, politicians, and the public. Policy Design and Practice. 2021;4(1):1-14.
- Stecula DA, Kuru O, Jamieson KH. How trust in experts and media use affect acceptance of common anti-vaccination claims. Harvard Kennedy School Misinformation Review. 2020;1(1).
- AD W. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic” – A Systematic Review. Risk Manag Healthc Policy. 2021;14:2609-2623:2609-23.
- Al-Mohaithef M, Padhi BK. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. Journal of multidisciplinary healthcare. 2020;13:1657.
- Marcec R, Majta M, Likic R. Will vaccination refusal prolong the war on SARS-CoV-2? Postgraduate medical journal. 2021;97(1145):143-9.
Reference this page as below
Edirisa Juniour Nsubuga1, Arthur G. Fitzmaurice2, Allan Komakech1, Tom Dias Odoi3, Daniel Kadobera1,4, Lilian Bulage1,4, Benon Kwesiga1,4, Peter James Elyanu3, Alex Riolexus Ario1,4, Julie Harris2. District Leader Community Dialogue Meetings Improved Willingness to Receive COVID-19 Vaccines in Western Uganda, May 2021: A Pre-Post Study. Kampala, Uganda National Institute of Public Health. 2022 March 30th Available from:https://uniph.go.ug/district-leader-community-dialogue-meetings-improved-willingness-to-receive-covid-19-vaccines-in-western-uganda-may-2021-a-pre-post-study.
Comments are closed.