
Readiness of Health Facilities to Manage COVID-19, Uganda, June 2021
Authors: Patience Mwine1*, Immaculate Atuhaire1, Sherry R. Ahirirwe1, Hilda T. Nansikombi1, Shaban Senyange1, Sarah Elayeete1, Veronicah Masanja1, Alice Asio1, Allan Komakech1, Rose Nampeera1, Edirisa J. Nsubuga1, Petranilla Nakamya1, Andrew Kwiringira1, Stella M. Migamba1, Benon Kwesiga1,2, Daniel Kadobera1,2, Lilian Bulage1,2, Paul E. Okello2, Sandra Nabatanzi3, Fred Monje1, Irene B. Kyamwine2, Alex R. Ario1,2, Julie R. Harris3___ Institutional Affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda, 2Uganda National Institute of Public Health, Kampala, Uganda, 3United States Centers for Disease Control and Prevention, Kampala, Uganda___ *Corresponding author: Email: pmwine@musph.ac.ug, Tel: +256702449738
Summary
Background: During 2020-2021, multiple waves of COVID-19 overwhelmed the capacity of health facilities globally, emphasizing the need to enhance facility readiness. In Uganda, regional referral hospitals (RRHs) managed severe COVID-19 patients, while lower-level health facilities screened, isolated, and managed mild cases. The first wave of COVID-19 in Uganda peaked in late 2020 and demonstrated challenges with facility readiness to manage large numbers of cases. The second wave began in May 2021. In June 2021, we assessed the readiness of health facilities in Uganda to manage the second wave of COVID-19. Methods: We assessed 88 health facilities. We purposively included all 17 referral health facilities in the country, all of which were managing COVID-19 patients, and 71 lower-level health facilities from all regions of Uganda. We used multistage sampling to randomly select the lower-level health facilities. In each of the facilities, we interviewed health facility heads about challenges faced during the first COVID-19 wave. We inspected COVID-19 treatment units (CTUs) at the referral hospitals and other facility service delivery points using the World Health Organization (WHO) observation checklist for capacity in infection prevention, medicines, personal protective equipment (PPE), and CTU surge capacity. We used the “ReadyScore” criteria to classify readiness levels as >80% (‘better prepared’), 40–80% (‘work to do’), and <40% (‘not ready’). We tailored facility readiness assessments to the specific health facility level being evaluated. Results: The overall median ±interquartile range; IQR) readiness score for all health facilities was 39% ± 12 (range, 8-83%). The median (IQR) readiness score in referral facilities was 63% ±17 (range, 46-83%), while in lower-level facilities it was 32% ± 24 (range: 8-78%). All 17 referral facilities assessed were managing COVID-19 patients at the time of our visit. Of these, two (12%) were ‘ready’ and 15 (88%) were in the “work to do” category. In relation to the number of COVID-19 patients admitted, 13 (82%) had an inadequate supply of essential medicines and 12 (71%) had insufficient oxygen; 11 (65%) needed but lacked space to expand CTUs to admit more COVID-19 patients in case of the surge. None of the 71 lower-level health facilities had COVID-19 patients isolated at the time of the visit. Sixteen (23%) of these facilities were in the “work to do” category and 55 (77%) were “not ready”. Seventy (99%) lacked medicines, 64 (90%) lacked PPE, and 53 (75%) lacked an emergency plan for COVID-19. Conclusion: Few health facilities were ready to manage the second wave of COVID-19 in Uganda during June 2021. The most significant gaps were in essential medicines, PPE, oxygen, and space for CTU expansion. Study results were used by the Ministry of Health to set up additional COVID-19 wards in hospitals and deliver medicines and PPE to all referral hospitals. Adequate readiness for future waves of COVID-19 requires additional support and action in Uganda.
Introduction
Ensuring the readiness of health facilities to respond to public health needs during emergencies is essential to effective epidemic management (1). Readiness is defined as a combination of the presence of appropriate infrastructure/amenities, basic supplies/equipment, standard precautions, laboratory tests, medicines and commodities, and trained health professionals (2). However, even countries with highly-resourced health care systems faced challenges with adequate readiness during the COVID-19 pandemic (3,4).
In February 2020, the World Health Organization (WHO) released a COVID-19 strategic response preparedness plan, meant to guide health facilities preparing for COVID-19 outbreaks (4). The key pillars of the plan included coordination, risk communication, infection prevention and control, logistics and medicines, ensuring continuity of other health services, and planning for surge capacity (1). In line with these pillars, Uganda’s Ministry of Health (MoH) equipped regional referral hospitals (RRHs) with trained health care workers and COVID-19 treatment units, and provided extra supplies of medicines and personal protective equipment at the beginning of the pandemic (5). Lower-level health facility health workers were trained to screen, identify, and manage mild cases and to refer severe COVID-19 cases to referral health facilities.
At the beginning of the pandemic, Uganda registered few COVID-19 cases, most among travelers and theirs contacts (6). However, community transmissions led to a rapid increase in cases starting in August 2020, which peaked around December 2020; 32,000 confirmed cases and 238 deaths were recorded in Uganda by the end of the first wave (7). During the peak of the first wave, health facilities faced major challenges in providing adequate care for COVID-19 patients, including having appropriate health facility infrastructure such as oxygen cylinders and patient beds, having sufficient trained health care workers, and having sufficient personal protective equipment (8). After a respite between waves of a few months, the second wave of COVID-19 began in May 2021 (7).
The second wave of COVID-19 in Uganda was driven primarily by the SARS-CoV-2 Delta variant, which was at the same time causing massive outbreaks in many other countries, including neighboring Kenya (9). Despite efforts to improve health facility readiness after the first wave, including installation of ICU beds and ventilators at the Mulago National referral Hospital and some regional referral hospitals, it was not clear how ready health facilities were for the second wave (10). We assessed the health facility readiness to manage the second wave of COVID-19 in Uganda and identified areas for improvement to strengthen capacity for future waves of COVID-19 cases.
Methods
Study setting
As of November, 2018, Uganda had a total of 6,937 health facilities, including public, private not-for-profit and private facilities (11). Of these, 3,133 (45%) were public health facilities, which provide free health care to the general population with support from the government and partners. Public health facilities are classified (from most basic to most advanced) into Health Centers Level One (HCI) through Four (HCIV), general hospitals, regional referral hospitals (RRH), and national referral hospitals (NRH). At the start of the COVID-19 pandemic, the MoH established COVID-19 treatment units (CTUs) in all 17 RRH in Uganda. These CTUs were equipped with oxygen cylinders, beds, medicines for managing COVID-19 (such as azithromycin), and new and existing health care workers were trained to manage patients. In addition, personal protective equipment appropriate for COVID-19 was distributed to facilities. A single advanced-level CTU with advanced life support machines was set up at Mulago National Referral Hospital (MNRH) to provide care to the most critically ill COVID-19 patients.
Site selection and sample size consideration
Health facilities: We purposively selected all 17 referral health facilities including three national referral hospitals (NRH) and 14 regional referral hospitals (RRH). We selected 71 lower-level health facilities using multistage sampling. First, we randomly divided the country into seven subregions and selected two districts from each: one with and the other without a referral health facility. From each district, we listed all the heath facilities and randomly selected one general hospital (GH), one health centre IV (HC IV), two health centre III (HC III), and two health centre II (HC II).
Health care workers: We interviewed the head of each health facility or CTU visited about COVID-19 response challenges in their health facilities.
Study variables and data collection
We interviewed heads of health facilities using a structured questionnaire. We obtained information on their experiences with the first and the start of the second waves of COVID-19 as well as the challenges they faced with case management. We inspected the CTUs and other service delivery points in the health facility using a readiness assessment tool developed by Centers for Disease Control and Prevention (CDC) for Non-US health care settings revised to suite Uganda’s situation (12).
We assessed facility-level response coordination by checking for documentation of health facility meeting minutes on COVID-19 response, availability of an emergency response plan, communication systems in place necessary for coordination and reporting of COVID-19 cases to the MoH.
We checked for availability of appropriate Personal Protective Equipment (PPE), medicines for management of COVID-19 and compared the counts to the average monthly consumption of individual health facilities. In addition to these we observed for oxygen equipment (cylinders, masks) and space for CTU expansion in case of a surge of COVID-19 patients for the referral health facilities. We checked for documentation on training and mentorship of health facility staff on COVID-19 and standard operating procedures for infection prevention. We also observed service delivery points, checked for infection prevention measures and the presence and functioning of triaging systems. Both the questionnaire and the checklist were in an electronic form prepared using Kobo Toolbox (13).
Data analysis
We imported clean data into EpiInfo version 7 for analysis. We determined a facility’s level of readiness using Resolve to Save Lives’ “ReadyScore” criteria (14). These criteria were developed to determine if health facilities in the country had the capacity to prevent, stop or control any epidemic. The individual facility percentage scores were categorized as not ready (<40%), work to do (40-80%), and ready (>80%) based on the “Ready Score” criteria. The classification of readiness of the health facilities was specific to the level of the health facility. We considered 59 questions for the lower level health facilities related to coordination, communication, reporting, supplies, training, triage, and evaluation of COVID-19 suspects. In addition to these questions, for referral health facilities, we assessed provision of care, monitoring of health care workers and inpatients, and preparation for a surge of COVID-19 cases to make a total of 71 questions. We coded “Yes” responses “one” and “No” as “zero”. We computed the percentage score for each health facility. We used QGIS software to map the geographical distribution of the health facilities visited.
Ethical considerations
This was a public health emergency and the Ministry of Health (MoH) gave the directive to evaluate for readiness of health facilities to manage the second wave of COVID-19 in the country. However, we also sought permission from the district health officials and heads of the health facilities.
We obtained verbal consent from respondents before interviews and inspections of various health facility service delivery points. During data collection, respondents were assigned unique identifiers instead of names to protect their confidentiality. Also, a non-research determination form was submitted to US CDC for clearance before the commencement of the assessment as a requirement.
The Office of the Associate Director for Science, U.S. Centers for Disease Control and Prevention, determined that this activity was in response to a public health emergency with the primary intent of public health practice (epidemic disease control activity). It was determined therefore to not be human subjects research.
This work was funded by the Cooperative Agreement-Provision of Comprehensive HIV/AIDS services and Developing National Capacity to manage HIV/AIDS Programs in the Republic of Uganda under the President’s Emergency Plan for AIDS Relief (Cooperative Agreement number)
Results
Characteristics of assessed health facilities
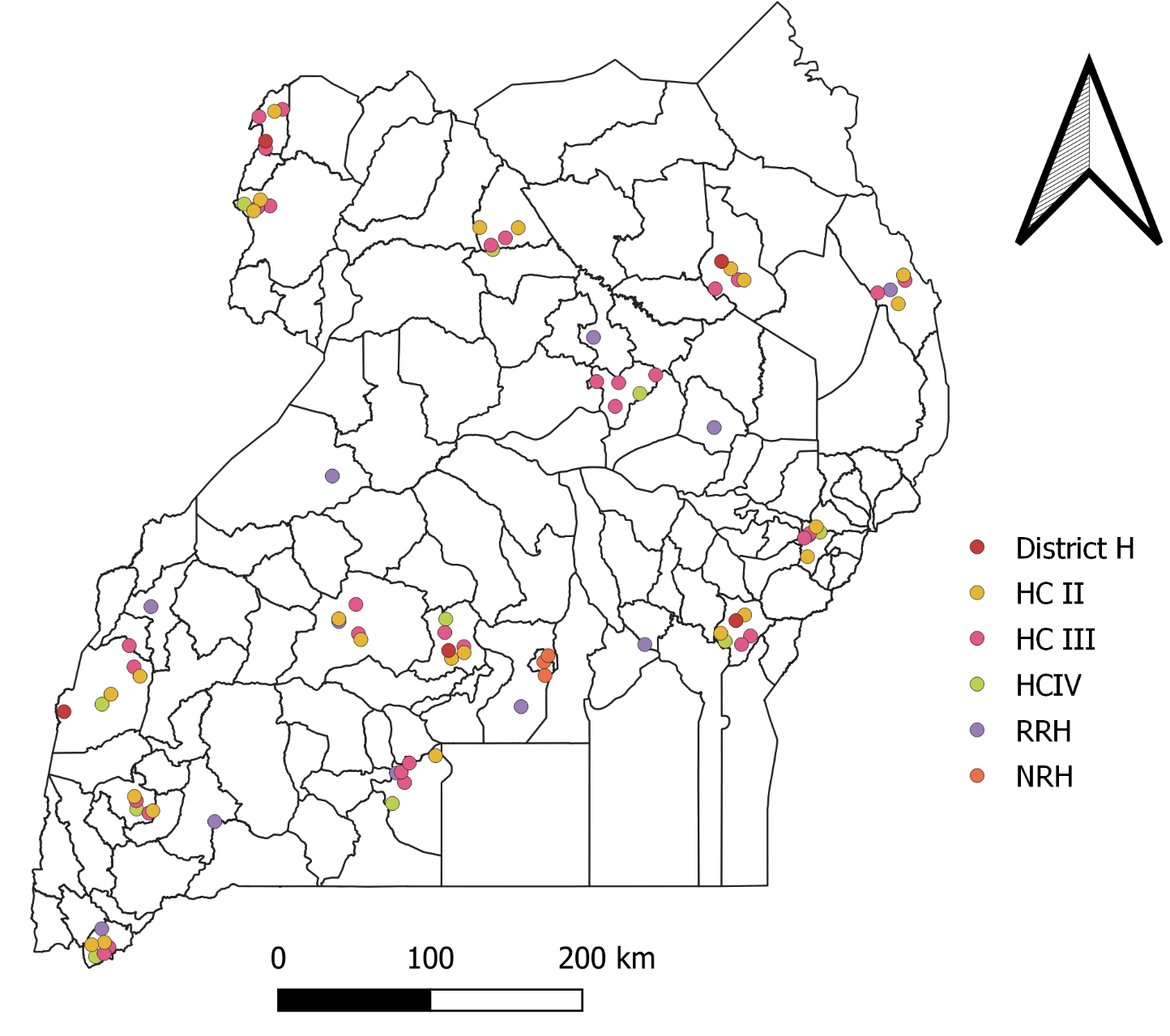
The 88 health facilities assessed were widely distributed across the country (Figure 1). At the time of the assessment, all 17 referral health facilities were managing COVID-19 patients and no lower-level health facilities had COVID-19 patients isolated.
Health facility readiness scores
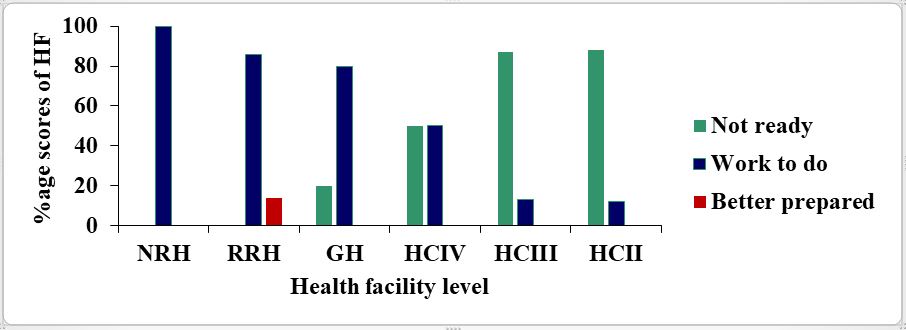
The overall median ±interquartile range; IQR) readiness score for all health facilities was 39% ± 12 (range, 8-83%). The median (IQR) readiness score in referral facilities was 63% ±17 (range, 46-83%), while in lower-level facilities it was 32% ± 24 (range: 8-78%). Of the 17 referral facilities, only two (12%), both regional referral hospitals, were “better prepared”, while 15 (88%) were in the “work to do” category. Fifty-five (77%) lower-level health facilities were in the “not ready” category (Table 1).
Table 1: Health facility readiness to manage the second wave of COVID-19 based on Resolve to Save Lives “ReadyScore” criteria, Uganda, June 2021
| Level of Health facility (n) | “Not ready”
(n, %) |
“Work to do”
(n, %) |
“Better prepared”
(n, %) |
| National Referral Hospitals (n=3) | 0 | 3 (100) | 0 |
| Regional Referral Hospital (n=14) | 0 | 12 (86) | 2 (14) |
| General Hospital (n=5) | 1 (20) | 4 (80) | 0 |
| Health Center IV (n=10) | 5 (50) | 5 (50) | 0 |
| Health Centre III (n=32) | 28 (87) | 4 (13) | 0 |
| Health Center II (n=24) | 21 (88) | 3 (12) | 0 |
The health facility readiness decreased with decreasing level of the facility (Figure 2).
Coordination, reporting, and preparation for the surge
Referral health facilities scored well in the coordination component of the assessment, with 100% having an IPC focal person and 82% having an emergency response plan describing the arrangement, responsibilities, and activities to enable the hospital to function adequately in the COVID-19 response. Most of referral health facility heads/CTU heads (14; 82%) knew their maximum capacity in the event of a surge of COVID-19 cases. However, 11 (65%) reported that they needed but lacked additional space to accommodate the expanding numbers of COVID-19 patients, and 12 (71%) did not include in their plans the option to stop non-essential services in case of overwhelming surge of COVID-19 cases (Table 2).
Comparatively, lower-level health facilities were poorly prepared. Fifty-three (75%) lower-level health facilities lacked emergency plans for COVID-19. Communication and reporting were poor in lower-level health facilities; 29 (41%) lacked personnel designated to report suspected or confirmed cases of COVID-19 (Table 2).
Table 2: Comparison of coordination, communication, and reporting systems among health facilities admitting and those not admitting COVID-19 cases during the second wave of COVID-19, Uganda, June 2021
| Referral HF (n=17) | Lower level HF (n=71) | |||
| Response pillar | Yes (%) | No (%) | Yes (%) | No (%) |
| Coordination | ||||
| Facility has an IPC focal person in place | 17 (100) | 0 (0) | 63 (89) | 8 (11) |
| The facility has an emergency response plan for COVID-19 | 14 (82) | 3 (18) | 18 (25) | 53 (75) |
| The facility has an emergency committee that meets weekly | 13 (76) | 4 (24) | 12 (15) | 59 (83) |
| IPC team participates in emergency committee meetings | 17 (100) | 0 (0) | 17(24) | 54 (76) |
| Communication and reporting | ||||
| Focal person(s) to receive reports of suspected or confirmed COVID-19 cases | 17 (100) | 0 (0) | 42 (59) | 29 (41) |
| A phone number to report suspected or confirmed COVID-19 cases | 16 (93) | 1 (6) | 55 (77) | 16 (23) |
| Health facility understands reporting levels of suspected or confirmed COVID-19 cases | 16 (93) | 1 (6) | 57 (80) | 14 (20) |
| A Referral system for suspected or confirmed COVID-19 for treatment is known. | 17 (100) | 0 (0) | 56 (79) | 15 (21) |
| Preparation for the Surge in CTU | ||||
| The facility knows its maximum capacity | 14 (82) | 3 (18) | NA | NA |
| The facility has developed a plan to stop non-essential services | 5 (29) | 12 (71) | NA | NA |
| The facility has identified additional space to expand the number of COVID-19 patients. | 11 (65) | 6 (35) | NA | NA |
| The facility has developed a plan to move non-critical patients. | 12 (71) | 5 (29) | NA | NA |
| The facility has estimated consumption rates for critical supplies. | 11 (65) | 6 (35) | NA | NA |
*CTU -COVID-19 Treatment Unit ** IPC-Infection Prevention Control
Training and triage
All 17 referral health facilities, health workers had received training to recognize COVID-19 symptoms. However, at 26 (37%) lower-level health facilities, reported the health workers did not receive COVID-19 training. Triage for respiratory patients was lacking in most lower level health facilities and some referral health facilities; 57 (80%) of the lower-level health facilities and 8 (47%) of the referral facilities lacked a physical barrier to separate health workers and patients during patient review. More so, respiratory (coughing) areas to isolate patients with acute respiratory symptoms were missing in 54 (76%) of lower-level health facilities and 2 (29%) of referral hospitals (Table 3).
Table 3: Comparison of training and triage systems among health facilities admitting and not admitting COVID-19 cases during the second wave of COVID-19, Uganda, June 2021
|
|
Referral HF (n=17) | Lower Level HF (n=71) | ||
| Variable | Yes (%) | No (%) | Yes (%) | No (%) |
| Training | ||||
| All HCWs were trained to recognize COVID-19 symptoms. | 17(100) | 0 (0) | 45 (63) | 26 (37) |
| HCWs managing COVID-19 trained in transmission-based precautions | 16 (94) | 1 (6) | NA | NA |
| Cleaners trained in cleaning CTU/Isolation units | 14 (82) | 3 (18) | NA | NA |
| Triage and evaluation of suspected COVID-19 cases | ||||
| Available alternative ways to seek care for patients with respiratory symptoms. | 10 (59) | 7 (41) | 14 (20) | 57 (80) |
| Directions (signs) patients with respiratory symptoms | 8 (47) | 9 (53) | 9 (13) | 62 (87) |
| A physical barrier is in place between staff and patients | 9 (53) | 8 (47) | 14 (20) | 57 (80) |
| A separate “respiratory waiting area”) | 12 (71) | 5 (29) | 17 (24) | 54 (76) |
| Benches, chairs, or other seating in the respiratory waiting area are separate by at least 1 meter | 12 (71) | 5 (29) | 15 (21) | 56 (79) |
| Functional hand hygiene available near the registration desk and respiratory waiting area | 17 (100) | 0 (0) | 50 (70) | 21 (30) |
| Dedicated toilets are available for patients in the respiratory waiting area | 4 (24) | 13 (76) | 6 (8) | 65 (92) |
| A separate room for conducting physical evaluations of other patients | 11 (65) | 6 (35) | 10 (14) | 61 (86) |
| COVID-19 triage forms and flow charts available | 9 (53) | 8 (47) | 12 (17) | 59 (83) |
| Access to PPE by HCW during patient examination | 13(76) | 4(24) | 24 (34) | 47 (66) |
| Plans for the safe transfer of patients with suspected or confirmed COVID-19 identified | 13 (76) | 4 (24) | 36 (50) | 35 (49) |
| The facility has increased staff dedicated to triage for COVID-19 | 7 (41) | 10 (59) | 6 (8) | 65 (92) |
| A separate temporary structure to for patients with fever and respiratory symptoms | 11 (64) | 6 (35) | 4 (6) | 67 (94) |
*HCW-Health Care Workers *** Personal Protective Equipment
Medicines and personal protective equipment supply
More referral health facility heads/CTU heads (16; 94%) knew how to estimate the critical PPE supply consumption rate than heads at lower-level health facilities (46; 65%).In relation to the number of COVID-19 patients admitted at the time of assessment, most referral health facilities (13; 82%) lacked essential medicines, (9;53%) lacked adequate PPE appropriate for COVID-19, and (12;71%) did not have oxygen supply and cylinders. Among lower-level facilities, all but one (70; 99%), lacked medicines and most (64; 90%) had inadequate PPE supplies (Table 4).
Table 4: Comparison of availability of essential medicines and personal protective equipment among health facilities managing COVID-19 patients and those not managing COVID-19 during the second wave of COVID-19, Uganda, June 2021
| Referral HF (n=17) | Lower Level HF (n=71) | |||||
| Variable | Yes (%) | No (%) | Yes(%) | No (%) | ||
| Essential medicines | ||||||
| Adequate medicines for the management of COVID-19 | 3 (18) | 13 (82) | 1 (1) | 70 (99) | ||
| Vitamin C | 6 (35) | 11 (65) | 6 (8) | 65 (92) | ||
| Zinc | 4 (23) | 13 (76) | 8 (11) | 63 (89) | ||
| Azithromycin | 2 (12) | 15 (88) | 0 (0) | 71 (100) | ||
| Dexamethasone | 3 (18) | 14 (82) | 6 (8) | 65 (92) | ||
| Clexane | 2 (12) | 15 (88) | NA | |||
| Ramdesivir | 0 (00) | 17 (100) | NA | |||
| Isolation spaces/ Isolation Units | 16 (94) | 1 (6) | 9 (13) | 62 (87) | ||
| HDU/ICU | 13 (76) | 4 (24) | NA | |||
| Adequate Oxygen Supply | 5 (29) | 12 (71) | NA | |||
| PPE supplies | ||||||
| Consumption rate (per week) for critical supplies estimated | 16 (94) | 1 (6) | 46 (65) | 25 (35) | ||
| Monthly inventory of PPE supply at least once a month | 16 (94) | 1 (6) | 45 (63) | 26 (37) | ||
| Available focal person to manage critical IPC supplies | 17 (17) | 0 (0) | 59 (83) | 12 (17) | ||
| Facility leadership knows how to request additional supplies | 17(100) | 0 (0) | 56 (79) | 15 (21) | ||
| Inventory of PPE supplies in the past seven days | 9 (53) | 8 (47) | 14 (20) | 57 (80) | ||
| Adequate medicines for the management of COVID-19 | 8 (47) | 9 (53) | 6 (8) | 65 (90) | ||
| The facility has the following PPE supplies in stock | ||||||
| Gowns | 12 (71) | 5 (29) | 4 (6) | 67 (94) | ||
| Aprons | 13 (76) | 4 (24) | 4 (6) | 67 (94) | ||
| Eye protection (face shields or goggles) | 13 (76) | 4 (23) | 5 (7) | 66 (93) | ||
| Surgical Face masks | 5 (29) | 12(71) | 12 (17) | 59 (83) | ||
| N 95, or equivalent respirators | 10 (59) | 7 (41) | 11 (15) | 60 (84) | ||
| Alcohol-based hand rub | 12 (71) | 5 (29) | 10 (14) | 61 (86) | ||
| Soap | 9 (53) | 8 (47) | 35 (49) | 36 (51) | ||
| Buckets | 8 (47) | 9 (53) | 5 (7) | 66 (93) | ||
| Hospital-grade disinfectants (Sodium hypochlorite) | 10 (59) | 7 (41) | 7 (10) | 64 (90) | ||
*PPE-Personal Protective Equipment ** ICU-Intensive Care Unit *** HDU-High Dependence Unit
Discussion
Early in the second wave of COVID-19 in Uganda, the readiness of most health facilities to manage cases was poor. Triage systems and supplies of medicines, personal protective equipment, and oxygen appropriate for management of COVID-19 were all lacking. Few referral facilities were able to expand their capacity for more COVID-19 patients in the event of a surge.
In addition, the overall median readiness scores for health facilities was 39%; this was below the recommended target of 80% for a health facility’s readiness score. This could have been due to low perception of the new wave of COVID-19 by most health facilities and relaxing of infection prevention measures after the first wave.
The readiness median scores were much lower (32%) in the lower-level health facilities than referral health facilities (63%). In addition, readiness declined with decreasing health facility level among lower-level health facilities. Also, despite the preparation in referral hospitals, at the beginning of the pandemic to manage COVID-19, only two regional referral health facilities were found to be ready to manage COVID-19 (9,10,11). The assessment was conducted at a time when the second wave had picked momentum, and these results show that referral health facilities were not ready for the second wave. Therefore, health facilities needed more support from Uganda’s Government and relevant bodies to improve their readiness to handle surges of COVID-19 cases, especially during acute phases of the pandemic.
This could have been due to low perceived risk of COVID-19 among the lower level health facilities, since they are located in rural areas compared to referral health facilities which are majorly located in urban area. Readiness of lower level health facilities is critical in controlling COVID-19 outbreaks especially community spread by supporting screening and management of mild cases. This would help in decongesting the referral health facilities hence the need for more support to lower level health facilities in Uganda.
We established poor triaging systems in all health facilities. Efficient triage of patients with COVID-19 at all levels of health facilities helps in planning, allocation of resources, case management as well as prevention of COVID-19 infections among health care workers and other patients (15). WHO recommends all health facilities to have triaging stations irrespective of the level of health facility(16).
A good triage system involves: screening of all patient for COVID-19 symptoms, isolation of patients with symptoms, ensuring infection prevention measures like strict wearing of mask, maintaining one-meter distance among others, to limit transmission of COVID-19 (15). A triage system is fairly inexpensive and reliable to screen and separate patients and is effective at preventing spread of COVID-19 with in the health facilities (17). Inadequate triage of patients increases the risk of exposure to COVID-19 among health care workers and the patients and can quickly become the source of infections to communities due to free interactions (18). Therefore, there is need to improve triage systems in all levels of health to prevent spread of COVID-19 with in the health facilities.
A considerable proportion of health facilities admitting COVID-19 patients lacked extra space for admitting more COVID-19 patients in case of a surge. A surge of COVID-19 cases could quickly overwhelm a health facility resulting in a lack of space in the planned hospitals initially. A similar incident occurred towards the end of the first wave; various hospitals lacked space to isolate and manage COVID-19 cases in the designated health facilities resulting into the MoH adopting the home-based care strategy to manage non-severe COVID-19 (8). However, this had consequences since most Ugandan families lack adequate space or rooms to serve the purpose, increasing the risk of infections among family members. According to WHO, 80% of COVID-19 cases are mild and can be manage as out patients’ cases (15). However, some of these may progress and develop severe symptoms which may necessitate hospitalization. Due to lack of monitoring and inadequate patient knowledge on when to report to the hospital, community deaths are likely to occur (19). From the results of all-cause mortality rapid surveillance, 51% of the reported community deaths had tested positive for COVID-19 between January to August 2021(20).
Inadequate supply of drugs and personal protective equipment to manage the number of existing patients was also a significant challenge. Drug shortage became a major challenge globally during the COVID-19 pandemic including high income countries (21). Countries attribute this inadequacy in essential supplies to the rapid increase in demand for personal protective equipment and drugs, resulting in early stock outs (22). Before the COVID-19 pandemic, the Uganda health care system was already weak due to an insufficient supply chain system and a constrained budget (23). Referral health facilities in Uganda rely on a Push inventory control system to receive supplies and drugs from the national medical stores (NMS). The disadvantage with this system is inaccuracies in the forecast; consumption can be unpredictable and vary depending on the season.
Health facilities do not request their projected supplies hence a possible reason for early stock outs, which burden them (24). If personal protective equipment is inadequate during the COVID-19 outbreak, health workers are likely to get exposed to COVID-19 infections, which puts them at risk of severe disease and death (25). Several countries registered a high number of COVID-19 infections among health care workers due to shortages in personal protective equipment (26). Furthermore, when health workers get COVID 19, they are likely to be the source of infections to the patients, families, and communities where they live (27).
In addition, inadequate oxygen supply to manage COVID-19 patients, especially in the COVID-19 treatment units, could result in early disease progression and massive deaths like in one of the national referral hospitals in Uganda (25). The shortage of oxygen supply became a big challenge in several countries, including India, which experienced the worst second wave of COVID 19 (28). These shortages have been due to increased demand and high consumption of oxygen by the COVID-19 patients. Oxygen therapy is crucial for COVID-19 patient survival (28, 29) and according to WHO, they require three times more oxygen than other patients.
Study limitations
were some limitations in the assessment. We could have interfaced some bias due to participant social desirability to perform better for some responses. In addition, the date of assessment of hospital readiness was not uniform among the surveyed health facilities making it impossible to assess the true variability of readiness among hospitals.
Conclusion
Ensuring the readiness of health facilities is vital in controlling the COVID-19 pandemic. Most health facilities managing COVID-19 patients were in the “work to do”, and those not admitting COVID-19 were in the “not ready” categories. Furthermore, health facilities were under-equipped with essential drugs, PPEs, and oxygen and could not expand to accommodate more COVID-19 patients. We presented our findings to the MoH, and the incident management team utilized them to support the health facilities in the response. The National Medical Stores made an emergency supply of medicines and personal protective equipment to the under-equipped referral hospitals. Also, an isolation ward was created at Kiruddu National Referral Hospital to separate COVID-19 patients from those with other medical conditions. Infection prevention and control were strengthened and respiratory areas were created in health facilities across the country.
Acknowledgments
We thank the health facility and COVID-19 treatment unit heads who participated in this evaluation. We are also grateful for the support from the medcal teams who were managing COVID-19 patients as well as well as the district health teams in Uganda.
References
- World Health Organization. Hospital preparedness for epidemics [Internet]. World Health Organization; 2014 [cited 2022 Mar 9]. 71 p. Available from: https://apps.who.int/iris/handle/10665/151281
- Ssempiira J, Kasirye I, Kissa J, Nambuusi B, Mukooyo E, Opigo J, et al. Measuring health facility readiness and its effects on severe malaria outcomes in Uganda. Sci Rep. 2018 Dec 18;8(1):17928.
- Covid-19 pandemic, declared by the World Health Organizsation (WHO). [Internet]. [cited 2021 May 5]. Available from: https://www.pharmaceutical-technology.com/news/who-declares-covid-19-pandemic/
- WHO. COVID-19 Strategic Preparedness and Response Plan (SPRP 2021) [Internet]. 2021 [cited 2022 Mar 9]. Available from: https://www.who.int/publications-detail-redirect/WHO-WHE-2021.02
- Seed, Global heath SG health. Frontline Dispatch: Regional COVID-19 Training in Uganda [Internet]. Seed Global Health. 2020 [cited 2022 Mar 14]. Available from: https://seedglobalhealth.org/2020/05/20/frontline-dispatch-regional-covid-19-training-in-uganda/
- Olum R, Bongomin F. Uganda’s first 100 COVID-19 cases: Trends and lessons. Int J Infect Dis. 2020 Jul;96:517–8.
- Uganda: WHO Coronavirus Disease (COVID-19) Dashboard With Vaccination Data [Internet]. [cited 2021 May 5]. Available from: https://covid19.who.int
- Voice of America. Uganda’s Health Care System Struggling Against Second COVID Wave [Internet]. 2020 [cited 2021 Jul 8]. Available from: https://www.voanews.com/covid-19-pandemic/ugandas-health-care-system-struggling-against-second-covid-wave
- Ajari EE, Ojilong D. Assessment of the preparedness of the Ugandan health care system to tackle more COVID-19 cases. Journal of Global Health [Internet]. 2020 Jul 30 [cited 2021 Jul 8];10(2). Available from: http://www.jogh.org/documents/issue202002/jogh-10-020305.htm
- Musasizi A, Jjingo MF. Uganda: Masaka Hospital to Get 10 Ventilators for COVID-19 Patients. The Monitor [Internet]. 2020 May 6 [cited 2022 Mar 14]; Available from: https://allafrica.com/
- MOH U. National Health Facility Master List [Internet]. Ministry of Health | Government of Uganda. 2018 [cited 2022 Mar 9]. Available from: https://www.health.go.ug/
- CDC. Facility readiness assessment for coronavirus disease 2019 (COVID-19) : infection prevention and control considerations in non-US healthcare settings [Internet]. 2019 [cited 2022 Mar 26]. Available from: https://stacks.cdc.gov/view/cdc/90293
- KoBoToolbox | Data Collection Tools for Challenging Environments [Internet]. [cited 2022 Mar 9]. Available from: https://www.kobotoolbox.org/
- Lives R to S. Resolve to Save Lives: ReadyScore [Internet]. [cited 2021 Jun 30]. Available from: https://resolvetosavelives.org/prevent-epidemics/readyscore
- WHO. Algorithm for COVID-19 triage and referral : patient triage and referral for resource-limited settings during community transmission [Internet]. WHO Regional Office for the Western Pacific; 2020 [cited 2022 Mar 26]. Report No.: WPR/DSE/2020/009. Available from: https://apps.who.int/iris/handle/10665/331915
- WHO. Establishing COVID-19 triage stations at healthcare facilities [Internet]. ReliefWeb. 2020 [cited 2022 Mar 26]. Available from: https://reliefweb.int/report/world/establishing-covid-19-triage-stations-healthcare-facilities-key-instructions-and-tips
- Gilbert A, Ghuysen A. Triage in the time of COVID-19. The Lancet Digital Health. 2022 Apr 1;4(4):e210–1.
- Heneghan et al. The Ongoing Problem of UK Hospital Acquired Infections [Internet]. The Centre for Evidence-Based Medicine. [cited 2022 Mar 26]. Available from: https://www.cebm.net/covid-19/the-ongoing-problem-of-hospital-acquired-infections-across-the-uk/
- Wasswa H. Covid-19: Uganda’s low inpatient numbers mask high community infection as desperate patients turn to herbs. BMJ. 2021 Aug 9;374:n1909.
- Byaruhanga et al. Counting deaths in Uganda: history, challenges, and what is currently being done amidst COVID-19 Pandemic [Internet]. UNIPH. 2021 [cited 2022 Mar 26]. Available from: https://uniph.go.ug/amp/counting-deaths-in-uganda-history-challenges-and-what-is-currently-being-done-amidst-covid-19-pandemic/
- Shukar S, Zahoor F, Hayat K, Saeed A, Gillani AH, Omer S, et al. Drug Shortage: Causes, Impact, and Mitigation Strategies. Front Pharmacol [Internet]. 2021 [cited 2021 Aug 16];0. Available from: https://www.frontiersin.org/articles/10.3389/fphar.2021.693426/full
- Cohen J, Rodgers Y van der M. Contributing factors to personal protective equipment shortages during the COVID-19 pandemic. Prev Med. 2020 Dec;141:106263.
- Understanding the Systems that Influence Distribution Channels for Drugs in Uganda – PEAH – Policies for Equitable Access to Health [Internet]. [cited 2021 Aug 16]. Available from: http://www.peah.it/2018/01/understanding-the-systems-that-influence-distribution-channels-for-drugs-in-uganda/
- Bukenya et al. Understanding the Systems that Influence Distribution Channels for Drugs in Uganda – PEAH – Policies for Equitable Access to Health [Internet]. 2018 [cited 2022 Mar 26]. Available from: http://www.peah.it/2018/01/understanding-the-systems-that-influence-distribution-channels-for-drugs-in-uganda/
- Athumani H. Uganda Loses 37 Health Workers to COVID-19 [Internet]. VOA. [cited 2022 Mar 26]. Available from: https://www.voanews.com/a/africa_uganda-loses-37-health-workers-covid-19/6207955.html
- Oksanen L-MAH, Sanmark E, Oksanen SA, Anttila V-J, Paterno JJ, Lappalainen M, et al. Sources of healthcare workers’ COVID‑19 infections and related safety guidelines. Int J Occup Med Environ Health. 2021 May 27;34(2):239–49.
- Sabetian G, Moghadami M, Hashemizadeh Fard Haghighi L, Shahriarirad R, Fallahi MJ, Asmarian N, et al. COVID-19 infection among healthcare workers: a cross-sectional study in southwest Iran. Virology Journal. 2021 Mar 17;18(1):58.
- Beaubien J. Africa Is Running Out Of Oxygen. NPR [Internet]. 2021 Jun 24 [cited 2022 Mar 26]; Available from: https://www.npr.africa-is-running-out-of-oxygen
- Ukor NA, Adebisi YA, Uwizeyimana T, Ahmadi A, Ekwebelem OC, Fadele P, et al. Community distribution of oxygen: a unique COVID-19 intervention. Tropical Medicine and Health. 2021 May 14;49(1):39.
Reference this page as below
Patience Mwine1*, Immaculate Atuhaire1, Sherry R. Ahirirwe1, Hilda T. Nansikombi1, Shaban Senyange1, Sarah Elayeete1, Veronicah Masanja1, Alice Asio1, Allan Komakech1, Rose Nampeera1, Edirisa J. Nsubuga1, Petranilla Nakamya1, Andrew Kwiringira1, Stella M. Migamba1, Benon Kwesiga1,2, Daniel Kadobera1,2, Lilian Bulage1,2, Paul E. Okello2, Sandra Nabatanzi3, Fred Monje1, Irene B. Kyamwine2, Alex R. Ario1,2, Julie R. Harris3. Readiness of Health Facilities to Manage COVID-19, Uganda, June 2021. Kampala, Uganda National Institute of Public Health. 2022 March 30th. Available from:https://uniph.go.ug/readiness-of-health-facilities-to-manage-covid-19-uganda-june-2021
Comments are closed.