
Trends and Distribution of Malaria Deaths Among the General Population, Uganda, 2015-2019
Authors: Peter Omms Oumo*1, Patricia Thiwe1, Dan iel Kadobera1, and Alex Riolexus Ario2; Institutional affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda, 2Uganda Nation- al Institute of Public Health, Kampala, Uganda; *Corresponding author: poumo@musph.ac.ug, Tel:+256-782533926
Summary
In Uganda, malaria is endemic in approximately 95% of the country, affecting over 90% of the population with up to 20% of all hospital deaths. We conducted a descriptive cross-sectional analysis of surveillance data (2015-2019) for confirmed malaria deaths from health facilities into the DHIS2 to understand the magnitude of malaria deaths and hence inform targeted interventions in Uganda.
Between 2015 and 2019, a total of 23,022 malaria deaths were reported, leading to an overall incidence of 62 deaths/100,000. Incidence of malaria deaths significantly increased from 15/100,000 in 2015 to 17/100,000 in 2016. The incidence then declined from 17/100,000 in 2016 to 13/100,000 in 2017 and to 7/100,000 in 2018. Malaria deaths generally significantly declined over the 5 years. The overall incidence among those aged >5 years was 43.2/100,000 and for those 5+years was 5.8/100,000, while incidence among both sexes was equal at 13/100,000. Malaria deaths were highest in May (2,121) through June (2,212) and then July (2,161) and November (2,016) of each year.
Malaria deaths were highest in May through June and then July and November of each year with children under five years being the most affected. The National Malaria Control Division (NMCD) should sustain the programs it is implementing such as the national net distribution campaigns, Integrated Vector Management (IVM), Indoor Residual Spraying, chemoprevention, provision of ACTs and RDTs for VHTs, passive and active malaria surveillance through improved weekly reporting and sustained field supervision. More efforts should be focused on the children under five years and months of May, June, July, and November when most deaths occur.
Background
Malaria is a leading cause of morbidity and mortality in many developing countries, where young children and pregnant women are the groups most affected[1]. In 2019, there were an estimated 229 million cases of malaria worldwide[2]. The estimated number of malaria deaths stood at 409,000 with children aged under five years being the most affected group; accounting for 67% (274,000) of all malaria deaths worldwide. The Global Technical Strategy for Malaria 2016–2030 (GTS) calls for reducing malaria cases and deaths by at least 75% by 2025 and at least 90% by 2030. Without a major turnaround, these targets are unlikely to be met – a challenge further compounded by insufficient levels of funding for malaria control [3].
With a prevalence of 19% in Uganda, malaria has remained endemic in approximately 95% of the country, affecting over 90% of the population [4]. It is the leading cause of morbidity and accounts for 30-50% of out- patient visits at health facilities, 15-20% of all hospital admissions, and up to 20% of all hospital deaths. More than one-quarter of inpatient deaths among children under five years of age are due to malaria [1].
The National Malaria Control Division Uganda has put in place several interventions to fight malaria and reduce malaria deaths. Some of the interventions put in place include: Long Lasting Insecticide Nets (LLINs) distribution through mass campaigns and 10% in ante- natal care facilities, Rapid diagnostic testing kits distribution, distribution of Artemisinin-based Combination Therapy (ACT), Integrated Community Case Management (iCCM), Indoor Residual Spraying (IRS), protecting women using IPTp with the antimalarial drugs Sulfa- doxine-Pyrimethamine (SP)[2]. Despite the highlighted interventions, Uganda has continued to register malaria deaths.
We analyzed surveillance data on malaria deaths in Uganda from 2015-2019, in order to guide the allocation of the limited available resources and inform the design of interventions to reduce malaria deaths.
Methods Study setting
This analysis covered all the 136 districts of Uganda which were reporting through the District Health Information System2 (DHIS2) at the time. Uganda is sub divided into 15 sub geographical regions of which three namely west Nile region, Busoga, and Teso regions are marked as high malaria death burden areas.
Study design and data source
We conducted a descriptive cross-sectional analysis of surveillance data for confirmed malaria deaths from health facilities into the District Health Information Soft- ware2 (DHIS2). DHIS2 is an open-access system for aggregating and collection and validation of case-based routine data with associated data elements of key epidemiological and data quality indicators. According to the malaria surveillance system, a malaria death is defined as death occurring from malaria and confirmed by malaria Rapid Diagnostic Test (mRDT) or microscopy in a re- porting health facility. Malaria death data is reported in such a way that when the malaria patients from the community seek health care from the Village Health Team (VHT) or health facility, the date of visit, their demographics, clinical presentation, diagnosis and treatment given is captured through the HMIS forms which is entered into the electronic system on a weekly basis.
VHTs submit their quarterly data to respective health facilities, which then submit their reports to the health sub district on a quarterly basis which further submit their data to the district health office where it is then submitted to the DHIS2.
Data abstraction, study variables, and analysis
We downloaded monthly malaria deaths reported in the inpatient departments by each district from DHIS2 on 14th January 2020. The data captures the malaria death’s demographics (age and sex), and health facility where they died, district, and region.
We abstracted data into Excel and analyzed using Excel and EPI info version 7.2. We computed incidence of malaria deaths per 100,000 population overall during 2015-2019 by sex, age (under 5 years and 5 years and above), district, and region. We computed incidences using population figures projected from 2014 census figures as denominators. The projected population for each year were: 35,502,100 in 2015, 36,652,700 in 2016, 37,838,900 in 2017, 9,059,000 in 2018 and 40,308,000 in 2019 with a growth rate of 3.3% (UBOS, 2015, 2018).
We also plotted the malaria deaths by month to establish seasonality in the reported number of deaths and by year to identify the variations in different years. We drew line graphs to identify trends of malaria deaths and tested the significance of the trends using logistic regression. We also used choropleth maps to show distribution of malaria deaths by place in the 135 districts in Uganda.
Ethical considerations
We utilized routinely collected malaria surveillance data from DHIS2. Ministry of Health gave us the permission to utilize the data. Data utilized did not have personal identifiers.
Results
Description of confirmed malaria deaths, Uganda, 2015-2019
Between 2015 and 2019, a total of 23,022 deaths were reported. Children < 5 years contributed the highest count of malaria deaths 14,314 (62%) com- pared to persons aged ≥5 years. Overall, males and females contributed equally to the total count of malaria deaths reported within the study period (50%).
Incidence of malaria deaths, Uganda, 2015-2019
The overall incidence of deaths in the 5 years was 62 deaths/100,000 population. The lowest incidence in deaths was recorded in 2018 (7/100,000) and the highest in 2016 (17/100,000) (Table 1).
Table 1: Incidence of malaria deaths, Uganda, 2015- 2019
| Years | Deaths | Population | Incidence/100,000 |
| 2015 | 5,153 | 35,502,100 | 15 |
| 2016 | 5,991 | 36,652,700 | 17 |
| 2017 | 4,722 | 37,838,900 | 13 |
| 2018 | 2,611 | 39,059,000 | 7 |
| 2019 | 4,545 | 40,308,000 | 12 |
| Total | 23,022 | 62 |
Trend of the overall incidence of malaria deaths, Uganda, 2015-2019
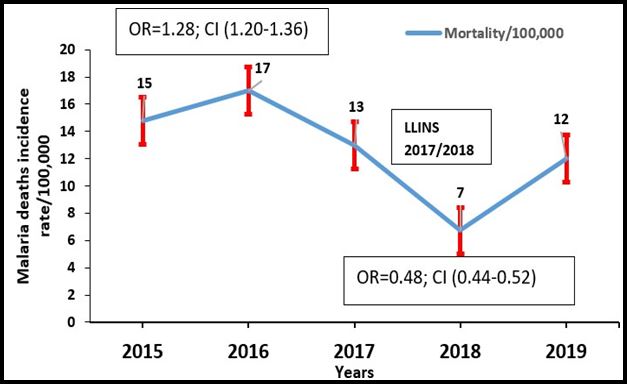
Incidence of malaria deaths significantly increased from 15/100,000 in 2015 to 17/100,000 in 2016. The incidence then declined from 17/100,000 in 2016 to 13/100,000 in 2017 and to 7/100,000 in 2018 (Figure 1).
Significance of trends of malaria deaths, Uganda, 2015-2019
Considering 2015 as the reference year. There was an observed significant increase of incidence of malaria deaths in 2016 by 28%; (OR=1.28; 95% CI=1.20-1.36) (Table 2). There was a reduction in malaria-related deaths by 16% (OR=0.84; 95% CI=0.78-0.90) in 2017, 52% reduction (OR=0.48; 95% CI=0.44-0.52) in 2018. There was a further significant reduction of malaria deaths by 16% in 2019 with (OR=0.84; 95% CI=0.79-0.90) (Table 2).
Table 2: Significance of trends of malaria deaths, Uganda, 2015-2019
| Year | OR | 95% CI | p-value |
| 2015 | 1 | ||
| 2016 | 1.28 | 1.20-1.36 | 0.000 |
| 2017 | 0.84 | 0.78-0.90 | 0.000 |
| 2018 | 0.48 | 0.44-0.52 | 0.000 |
| 2019 | 0.84 | 0.79-0.90 | 0.000 |
Incidence of malaria deaths, by age, Uganda, 2015-2019
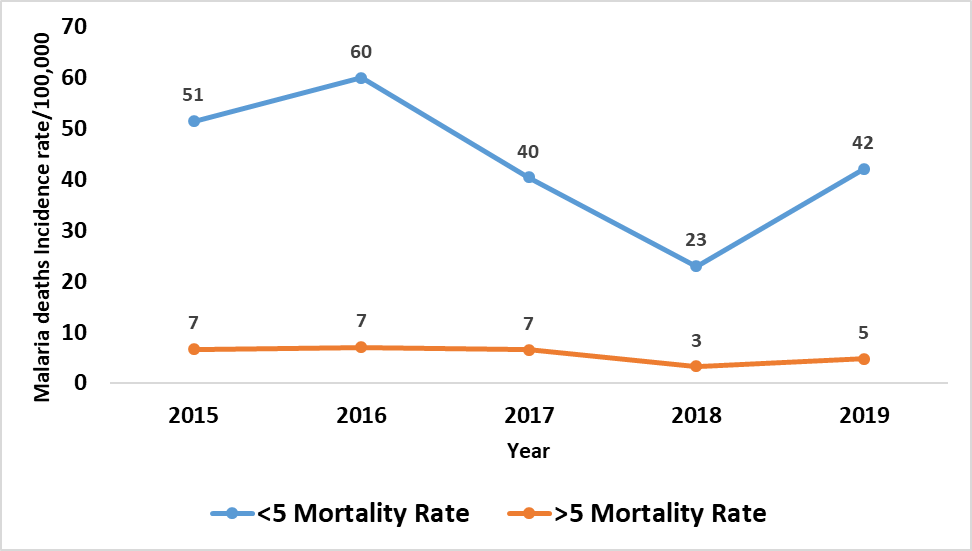
Consistent with the national trend, we observed that the total deaths of both the <5 and 5+ years aged persons significantly recorded (Table 2) their highest incidence of malaria deaths in 2016 with children < 5 years having an incidence of 60/100,000 and ≥ 5 years having 7/100,000. The deaths then reduced by half in both age groups falling to 23/100,000 for children < 5 years in 2018 (Figure 2).
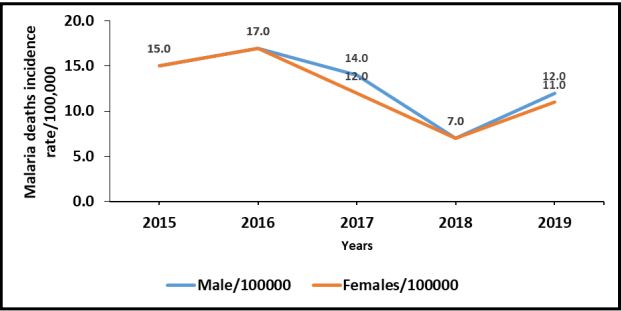
Consistent with the national trend of the total deaths (Table 2), we observed a similar statistically significant increase in incidence rates of malaria mortality of 13 deaths/100,000 population in females vs. 13 deaths/100,000 population in males. In 2016, the incidence of deaths in both sexes significantly increased to (IR=17/100,000) population OR=1.28; 95% CI (1.20-1.36) (Figure 3).
Both sexes reported a decline in malaria related death incidence in 2018 with the overall average incidence of 7/100,000; OR=0.48; 95% CI (0.44-.52). In 2019, the incidence in both sexes shot up registering (IR=12/100,000) in males and (IR=11/100,000) in females OR=0.84; 95% CI (0.79- 0.90) (Figure 3).
Seasonal variation of total malaria deaths, Uganda, 2015-2019
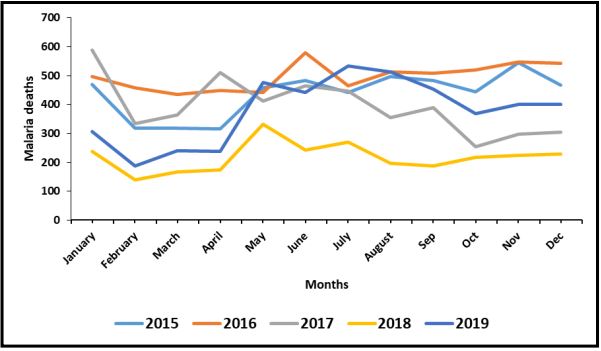
Consistent with the national trend of malaria deaths, the lowest deaths in malaria was reported in 2018 with the month of February (1438) having the lowest deaths. The highest deaths were reported in 2016. The months that experienced the highest deaths were: May (2,121), June (2,212), July (2,161) and November (2,016) There were notable spikes in the months of November 2015 and June 2016 (Figure 4).
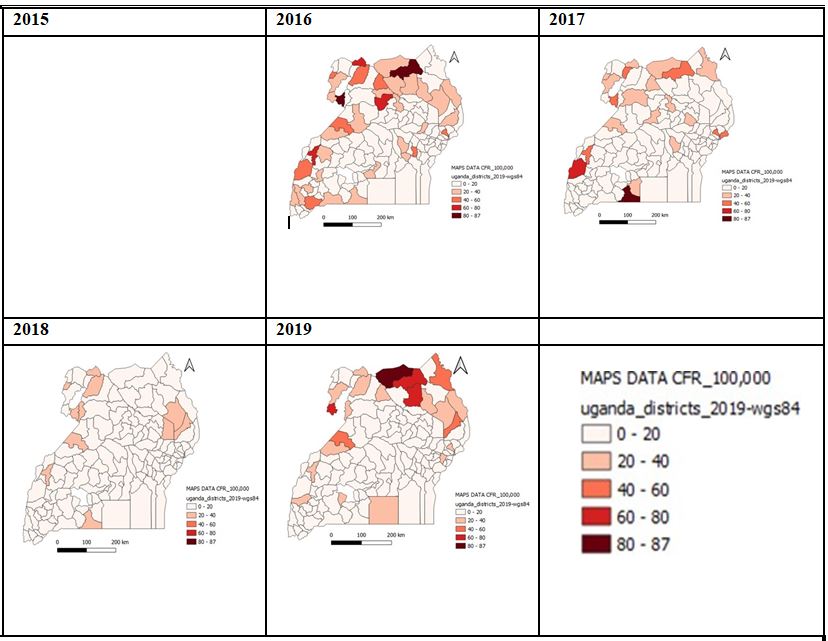
Distribution of malaria deaths by district, Uganda, 2015-2019
The geographic distribution of malaria mortality/100,000 in Uganda indicates a general decline in malaria deaths over the 5 years. The years with the highest incidence in deaths are 2016 and 2019. While those with the lowest incidence in deaths were 2017 and 2018. The northern part of the country especially West Nile, Karamoja, and Acholi regions had higher incidences of malaria deaths in 2015-2019. In 2015, 24 districts recorded IR above 20 deaths/100,000 population. The deaths went up by 11 districts with a total of 31 districts reporting above 20 deaths/100,000 population. In 2018 the incidence of death declined with districts that had 20/100,000 deaths reducing to only 7 (Figure 5).
Discussion
There was a general reduction in malaria deaths incidence with the only significant increase being in 2016. The incidence of malaria deaths was higher among children < 5 years. Similar results from in a study in Zambia found that children aged < 5 years usually had a 4-fold risk of contracting and dying from malaria compared to their older counterparts above 5 years old [5]. This is also similar to studies done in Zimbabwe and Ethiopia where children were among the most affected people with many deaths occurring amongst them[6] [2] [7].
The northern part of the country especially West Nile, Karamoja, and Acholi areas had higher incidences of malaria deaths, 2015-2019. The transmission of malaria is dependent on the presence of the vector mosquitoes whose breeding habits depend on rainfall patterns and ambient temperatures[7]. The semi-arid climate with warm temperatures, humid conditions, coupled with rainfall favors mosquito breeding in these areas hence more cases of severe malaria which result into deaths. Poor health seeking behaviour including delay in seeking treatment and the long distances to heath facilities have also led to the delay of managing severe malaria hence resulting into deaths[8]. Similar to the districts identified to have the highest incidence in this study, the annual report of 2017 and a study on the 2016 malaria upsurge identified districts in the north including Yumbe, Moyo, Adjumani, Lamwo, and Namayingo from the East to have the highest incidence of deaths [9][10].
The rise in deaths in April and June is due to the rainy season which leads to increased breeding sites for mosquitoes increasing vector density and in turn exposure to mosquito bites[11].
In 2018, the rise in total malaria deaths in the months of April to June was not as high as the previous years.
Such flattening of the incidence curves is indicative of interrupted transmission possibly due to the effect of interventions such as: Long Lasting Insecticide Nets which are rendered effective for 3 years while Indoor Residual Spraying effectively reduces mosquito density in the households for 6 months after the last spray[11] [9]. Furthermore, at the start of 2017 to early 2018, LLINs were distributed through a universal campaign achieving an operational coverage of over 95% from 51% in 2016 [10].
Incidence of malaria deaths increased exponentially in 2015, 2016, and 2017 in November and May respectively [3]. In 2019, malaria deaths were on the rise com- pared to 2018 and the transmission peak was untypically long with causes pointing to increased rains and aging of mosquito nets. This emphasizes the need to increase efforts towards maintaining gains obtained so far[11][12].
Limitations
We utilized surveillance data characterized by missing values hence a possible under or over estimation of the magnitude of the incidence of malaria deaths in the country.
Conclusion and recommendation
Whereas there was an increase in Incidence of malaria death in 2016, there was a general decline in malaria deaths incidence between 2017 and 2019. Malaria deaths were highest in May through June and then July and November of each year with children < 5 years be ing the most affected. The National Malaria Control Division (NMCD) should sustain the programs it is im plementing such as the national net distribution campaigns, Integrated Vector Management (IVM), Indoor Residual Spraying, chemoprevention, provision of ACTs and RDTs for VHTs, passive and active malaria surveillance through improved weekly reporting and sustained field supervision. More efforts should be focused on the children < 5 years and months of May, June, July, and November when most deaths occur.
Acknowledgements
We would like to thank, the Ministry of Health for giving us the opportunity to access DHIS2 data. We appreciate the of staff of NMCD for their technical guidance during the writing of this project. We thank the US-CDC for funding the Uganda Public Health Fellowship Program activities.
References
- Y. The United Nations Children’s Fund (UNICEF), “Malaria a Major Cause of Child Death and Poverty in Africa Controlling the Malaria Burden in Africa –,” pp. 1–17, 2004.
- World malaria report, World malaria report 2019. 2019.
- WHO, “High burden to high impact A targeted malaria response “ A MASSIVE,” 1–8, 2018.
- NMCP, “Uganda National Malaria Control Policy,” June, 2010.
- Nawa, P. Hangoma, A. P. Morse, and C. Michelo, “Investigating the upsurge of malaria prevalence in Zambia between 2010 and 2015: A decomposition of determinants,” Malar. J., vol. 18, no. 1, pp. 1–10, 2019, doi: 10.1186/s12936- 019-2698-x.
- Tesfahunegn, G. Berhe, and E. Ge- bregziabher, “Risk factors associated with malaria outbreak in Laelay Adyabo district northern Ethiopia, 2017: Case-control study design,” BMC Public Health, vol. 19, no. 1, pp. 1–7, 2019, doi: 10.1186/s12889-019-6798-x.
- Roberts and G. Matthews, “Risk factors of malaria in children under the age of five years old in Uganda,” Malar. J., vol. 15, no. 1, pp. 1– 11, 2016, doi: 10.1186/s12936-016-1290-x.
- M. Mutombo et al., “Severe malaria and death risk factors among children under 5 years at Jason Sendwe hospital in democratic republic of Congo,” Pan Afr. Med. J., vol. 29, pp. 1–8, 2018, doi: 10.11604/pamj.2018.29.184.15235.
- M. & E. U. Uganda Ministry of Health, National Malaria Control Division, “Annual Re- port,” no. National Malaria Annual Report 2017- 2018, 2019, [Online]. Available: file:///Users/ walusimbidennis/Downloads/Malaria Annual Report July 2017 web (2) (3).pdf.
- Health and R. B. Malaria, “Severe malaria.,” Trop. Med. Int. Health, vol. 19 Suppl1, pp. 7– 131, 2014, doi: 10.1111/tmi.12313_2.
- USAID and CDC, “U . S . President ’ s Malaria Initiative Cambodia: Malaria Operational Plan FY 2020,” pp. 1–136, 2020.
- Nile, N. Districts, A. Districts, K. Districts, and A. Districts, “MALARIA SITUATION REPORT AS AT 24th SEPTEMBER 2019,” no. September, 2019.
Reference this page as below
Peter Omms Oumo*1, Patricia Thiwe1, Daniel Kadobera1, and Alex Riolexus Ario2. Trends and Distribution of Malaria Deaths Among the General Population, Uganda, 2015-2019, Kampala, Uganda National Institute of Public Health, 2021 September 30th. Available from:https://uniph.go.ug/trends-and-distribution-of-malaria-deaths-among-the-general-population-uganda-2015-2019.
Comments are closed.