
Timeliness and completeness of monthly disease surveillance data reporting in Uganda, 2020─2021
Authors: Robert Zavuga*1, Richard Migisha1, Doreen Gonahasa1, Daniel Kadobera1, Benon Kwesiga1, Peter Edward Okello1, Lilian Bulage1, Freda Loy Aceng2, Joshua Kayiwa3, Issa Makumbi3, Alex Riolexus Ario1; Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda, National Institute of Public Health, Kampala, Uganda, 2Department of Integrated Epidemiology, Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda, 3Public Health Emergency Operations Center, Ministry of Health, Kampala, Uganda; *Correspondence: Email: rzavuga@musph.ac.ug, Tel: +256772655723
Summary
Background: In Uganda, electronic District Health Information System (DHIS2) surveillance data are entered by health facilities on a weekly or monthly basis. The monthly outpatient department (OPD) reports are submitted in 3 different categories namely; nationals, refugees, and foreigners. For the purpose of this study, OPD reports from only Ugandan nationals were considered. We assessed completeness and timeliness of monthly OPD data from Ugandan nationals from January 2020 to December 2021.
Methods: We used DHIS2 data from all 15 regions and 146 districts of Uganda from January 2020─December 2021. Completeness was defined as the number of submitted reports divided by the number of expected reports from the same health facility, district, or region. Timeliness was defined as the number of reports submitted by the deadline (15th day of the succeeding month) divided by reports received. Facilities, districts, or regions with completeness or timeliness <80% were regarded as having submitted incomplete or untimely reports.
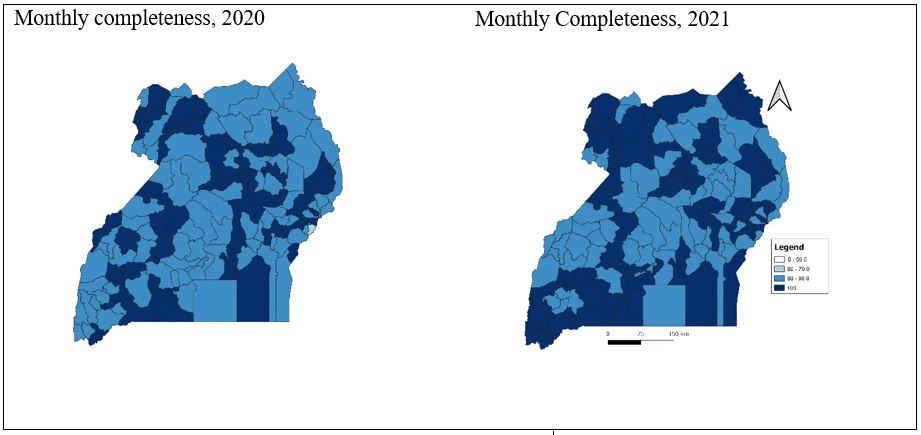
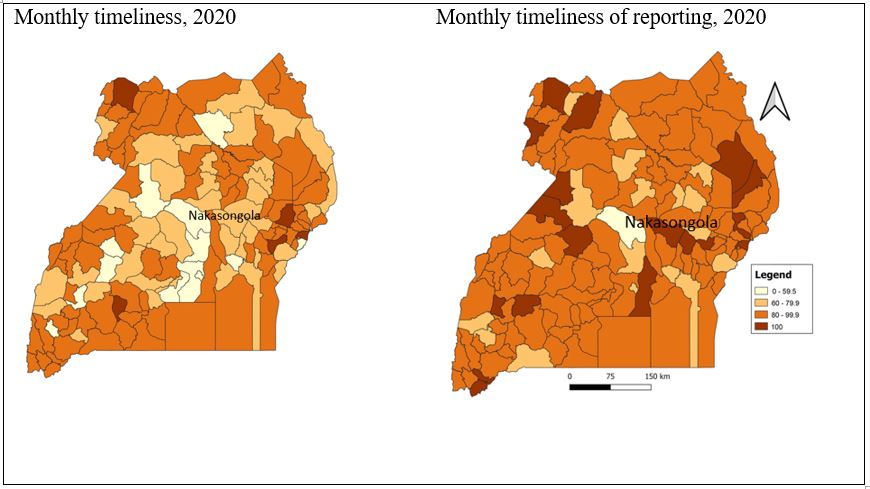
Results: Overall, there was good general performance with the median completeness of facility OPD reports being high in 2020 (99.5%; IQR 97.8-100%) and 2021 (100%; IQR 98.7-100%), as was the median timeliness (2020, 82.8%, IQR 74.6-91.8%; 2021, 94.9%, IQR 86.5-99.1%). In terms of regions, no region reported below the 80% OPD completeness target; Kampala region (comprising Kampala, Wakiso, and Mukono districts) was the only region that consistently failed to reach ≥80% OPD timeliness (2020: 44%; 2021: 65%). Nakasongola was the only district which consistently performed poorly in submission of timely reports in both years (2020:54.4%, 2021:58.3%). National Referral Hospitals consistently failed to meet the timeliness target in both years (2020:47.2%;2021:74.1).
Conclusion: There was an overall good performance in submission of complete and timely monthly OPD reports in both 2020 and 2021 in the DHIS2 across most districts and regions in Uganda. There is need to strengthen the good reporting practices exhibited and offer support to regions, districts, and health facilities with challenges to timeliness.
Introduction
Timely and complete reporting of routine public health information about diseases and public health events are important aspects of a robust surveillance system[1]. Through public health disease surveillance systems, information is continuously and systematically collected, analysed, interpreted, and disseminated to guide the planning and implementation of public health programs[2]. Recurrent outbreaks which sometimes can lead to widespread epidemics and transmission to other countries demonstrate the need of having a surveillance system that provides complete information that allows it to detect changes in disease patterns in time so as to mount a response. Despite the increased efforts of strengthening health information reporting at different levels, Low-Income Countries (LIC) are still challenged with untimely, incomplete, and inaccurate surveillance information which in turn affects the planning, monitoring, and evaluation of health sector performance and service delivery[3].
The introduction of a paperless system is one of the ways employed to improve the timeliness and completeness of reporting public health information and events in Uganda. The Ministry of Health (MoH) in Uganda operates a web-based information system known as the District Health Information System (DHIS 2) in which the data that are routinely generated from health facilities are filled in on a weekly and monthly basis. In this system, all the primary data received from lower-level health facilities which are captured in paper format are entered into the DHIS2 at the district level [3]. This interchange and transfer of data from paper into the DHIS2 is likely to cause considerable distortions in terms of accuracy, timeliness, and completeness [4]. The DHIS2 has undergone three significant revisions and upgrades since its inception in 2010 and thus has the following versions: 2010-2014, 2015-2019, and 2020-2024. These revisions and upgrades were aimed at improving system performance and to also incorporate the new districts and regions that have been created from time to time.
The Integrated Disease Surveillance and Response (IDSR) indicators guide that for a report to be timely, 80% of health facilities must have submitted in time and for a report to be complete 80% of the expected reports should have been submitted [5]. A weekly epidemiological report published in January 2022 indicated that only 8 of the 15 regions in Uganda met the completeness target of 80% and no region met the timeliness target [6]. Subpar timeliness or completeness may lead to delayed detection of infectious diseases and the potential for larger outbreaks than would otherwise occur. Although data on completeness and timeliness of surveillance data is collected in the DHIS2 version 2020-2024; it has not been routinely analysed. The reporting of outpatient department (OPD) data in the years 2020 and 2021 could have been interrupted by the coronavirus disease 2019 (COVID-19) pandemic that was at the peak in this period [7], and therefore there could be some areas of weakness in the surveillance system. Therefore, by periodically evaluating the timeliness and completeness of reporting of routine surveillance data, it is possible that specific barriers and challenges to reporting can be identified and immediately improved upon. Ultimately, improvement across these metrics should enable rapid and timely response to disease outbreaks and mounting of control measures. We estimated the timeliness and completeness of monthly OPD disease surveillance reports submitted to the DHIS2 in Uganda from January 2020-December 2021 so as to provide evidence-based recommendations to the Ministry of Health.
Methods
Study setting and design
We conducted a descriptive quantitative study that involved analysis of monthly OPD disease surveillance reports submitted to the DHIS2 from January 2020 to December 2021. Uganda has 146 districts which are distributed across 15 regions as designated by Ministry of Health[8]. These regions are Acholi, Ankole, Bugisu, Buekdi, Bunyoro, Busoga, Kampala, Karamoja, Kigezi, Lango, North central, South Central, Teso, Tooro and West Nile.
The health care system has several government and privately owned health facilities which are organized in a hierarchical order[9]. At the bottom are the community health works also known as the Village Health Team (VHT) members who report observations to the lowest Health Centers (HC) at the community level all way to the highest level of health facilities. That is, the lowest health centers being HCIIs (found at parish level), HCIIIs (found at sub-county level), HCIVs (found at county/health sub-district level), district hospitals (found at district level), regional referral hospitals (found at region level) and the national referral Hospital found at national level.
Data source
We extracted data from the DHIS2 from all the regions of Uganda which comprise the 146 districts. The DHSI2 is a web-based open-source health management information system used to collect aggregate data which is routinely generated across health facilities [10]. The DHIS2 also has capabilities for data analysis, data management, and data visualization. The DHIS2 automatically determines completeness and timeliness. The reports that are submitted by the deadline date are considered to be timely and the proportion of the actual number of reports submitted against the expected number of reports are regarded as complete. The monthly OPD reports are submitted in 3 different categories namely; nationals, refugees, and foreigners. For the purpose of this study, OPD reports from only nationals were considered.
Generation of surveillance data
Routine surveillance data are generated at the community through routine surveillance activities carried out by the VHTs. The disease surveillance reporting system follows a hierarchical order from the community level to the national level through the DHIS2.
At the health facility level, information is first collected as patient-specific data using paper-based IDSR surveillance tools and later transferred into the electronic format-the DHIS2 as aggregated data. The monthly OPD report is an aggregated report for all OPD occurrences at each health facility. It contains data on OPD attendances, referrals, diagnosis, infectious disease and epidemic prone diseases, non-communicable diseases, maternal and child health, family planning, and immunisation services.
The IDSR defines completeness as the proportion of reports submitted divided by the number of expected reports from the same health facility, district or region in a given time period while timeliness is defined as proportion of reports submitted by the deadline divided by actual reports received in the given time period. Health facilities are expected to submit complete monthly reports by the 15th of the succeeding month. The facilities with percentages below the 80% are regarded as having submitted incomplete or untimely reports. Data from different health centers are sent to the district and then later merged into regions constituting different districts.
Data abstraction and analysis
We captured different variables for the years of 2020 and 2021. These years were considered because we wanted to evaluate the immediate past performance trends of the reporting indicators especially after the COVID 19 response period of 2020-2021. A data abstraction form was used to extract information on expected number of reports, actual number of reports, actual number reports on time. It is from these variables that the monthly completeness and timeliness were computed. Completeness was calculated as the number of actual monthly OPD reports received divided by the expected number of reports in a given year and expressed as a percentage. Timeliness was calculated as the number of actual monthly OPD reports received on time (by the 15th of every month) divided by the expected number of reports in a given year and was also expressed as a percentage. We determined the overall proportions of completeness and timeliness of reporting by year at national level, region, district, level of health facility, and health facility ownership. We analysed data using EPI INFO version 7.0
Ethical considerations
Since our study used routine surveillance data reported by health facilities in the DHIS2 which were also aggregated with no individual patient identifiers, we did not seek for ethical approval. However, we sought permission to use the data from the Uganda Ministry of Health. The US Centers for Disease Control and Prevention (CDC) also provided the non-research determination (NRD) for non-human subjects. Data were only accessed by the study team.
Results
Completeness and timeliness of monthly outpatient department reporting, overall, region, level of health facility, and level of ownership, Uganda, 2020-2021
Overall, in 2020 the expected number of reports was 69,468 and of these, 68,935 reports were submitted and 52,430 were submitted in time corresponding to 99.2% completeness and 75.5% timeliness. However, in 2021, the expected number of reports of was 69,659 and of these 61,490 were submitted in time corresponding to 99.8% completeness and 88.1% timeliness. The median completeness of facility OPD reports was high in 2020 (99.5%; IQR 97.8-100%) and 2021 (100%; IQR 98.7-100%), as was the median timeliness (2020, 82.8%, IQR 74.6-91.8%; 2021, 94.9%, IQR 86.5-99.1%).
There was a general improvement in reporting in terms of completeness and timeliness from 2020 to 2021. This trend is similar across all regions, level of health facilities, and type of ownership of health facility. Regarding completeness, all regions scored above the required reporting target of 80% in 2020 and 2021. However, 7 out of 15 regions did not reach the timeliness reporting target in 2020 and in 2021, only Kampala region did not score above the timeliness target. Kampala region was the only region which consistently failed to meet the 80% timeliness target in both years (2020: 44.4%; 2021: 64.7%).
All levels of health facilities scored above the required completeness target in both years. National Referral Hospitals were the only facilities that consistently failed to meet the timeliness target in both years (2020:47.2%;2021:74.1).
Privately owned health facilities failed to score above the required timeliness target in 2020. Although they improved and scored above the timeliness target in 2021, they still performed poorer than government owned facilities (Table 1).
Table 1: Completeness and timeliness of monthly outpatient department reporting per region, level of health facility, and level of ownership, Uganda, 2020-2021
| 2020 | 2021 | |||
| Completeness (%) | Timeliness (%) | Completeness (%) | Timeliness (%) | |
| Region | ||||
| Acholi | 98.7 | 73.2 | 98.9 | 88.7 |
| Ankole | 99.8 | 77.1 | 100 | 89.9 |
| Bugisu | 98.3 | 84 | 100 | 96.9 |
| Bukedi | 97.1 | 82.5 | 96.8 | 86.3 |
| Bunyoro | 96.8 | 72.9 | 99.1 | 87.7 |
| Busoga | 98.6 | 74.1 | 99.9 | 86.1 |
| Kampala | 100 | 44.4 | 100 | 64.7 |
| Karamoja | 98.8 | 81.1 | 98.9 | 93.4 |
| Kigezi | 99.1 | 95.2 | 100 | 99.6 |
| Lango | 100 | 83.6 | 100 | 87.4 |
| North Central | 100 | 70.1 | 100 | 88.2 |
| South Central | 96.4 | 75.3 | 97.6 | 88.8 |
| Teso | 98.6 | 81.1 | 97.3 | 89.4 |
| Tooro | 98.4 | 81.4 | 99.4 | 95.5 |
| West Nile | 100 | 91.3 | 100 | 97.9 |
| National Level | 99.2 | 75.5 | 99.8 | 88.1 |
| Level of health facility | ||||
| Health Center II | 96.6 | 73.8 | 99.8 | 87.4 |
| Health Center IIII | 98.7 | 80.0 | 99.1 | 90.9 |
| Health Center IV | 97.9 | 79.7 | 99 | 89.9 |
| District Hospital | 99.8 | 75.9 | 100 | 88.6 |
| Regional Referral | 99.0 | 67.2 | 100 | 83.8 |
| National Referral | 100 | 47.2 | 100 | 74.1 |
| Health facility ownership | ||||
| Government | 99.1 | 80.4 | 99.7 | 91.6 |
| Private | 100 | 69.9 | 100 | 84.2 |
District monthly completeness and timeliness of outpatient department reports, Uganda, 2020-2021
In 2020, all districts scored above the recommended target for completeness except Namisindwa while in 2021 all districts scored above the required target. In regard to timeliness, 59 (40%) districts failed to submit monthly OPD reports on time in 2020 and 21 (14.4%) districts failed to submit on time in 2021 (Figure 1a). Nakasongola was the only district which consistently performed poorly in submission of timely reports by scoring below 80% in both years (2020:54.4%, 2021:58.3%) (Figure 1b).
Discussion
In our analysis of the monthly disease surveillance reporting data, we found that there was good general performance in completeness and timeliness of reporting. In 2020 almost half the number of regions did not submit reports in time. Kampala region was the only region which consistently failed to reach the timeliness target in both years. At district level, Nakasongola District was the only district which consistently failed to score the timeliness target. Additionally, higher level health facilities like national referral hospitals and referral hospitals performed poorer than lower-level health facilities in terms of submission of timely reports. This study addresses the importance of monitoring routine surveillance data especially that which is collected on a monthly basis for public health action.
There was good general good performance in completeness and timeliness of reporting. This is due to regular mentorship and improved capacity of district biostatisticians and data personnel to collect and submit disease surveillance data [11]. Additionally, the switch from paper-based reporting to electronic internet based reporting and improved Information and Communication Technology (ICT) capabilities has played a big role in improving performance [12]. These observations are in line with other studies. A study which was done to explore the challenges in implementing surveillance tools of High Income Countries (HIC) in Low Middle Income Countries (LMICs) indicates that improvement of capacity of health workers in data collection through education and mentorship improves on the performance of surveillance information reporting[13]. Furthermore, a study which was done in Tanzania about use of technology innovations and ICT reported that improved ICT services provide an opportunity for better reporting and early detection of diseases[14].
In 2020, almost half of the regions did not achieve the 80% timeliness target. This was likely because of task shifting which was characterized by the COVID-19 pandemic during this time. Various health carders including medical data personnel were assigned other duties of active case finding and contact tracing and left the data departments understaffed thus affecting the timeliness of reporting [15]. Task shifting has been identified as an effective strategy in times of human resource scarcity. However, a Ugandan study, revealed that it may lead to low efficiency in performance of core functions and this affects quality of the tasks assigned [16]. On the other hand, a systematic review done on task shifting in Sub Saharan Africa recognizes that although it is cost effective, it has a risk of competing with other health service priorities [17]. Task shifting should be done without stifling the responsibilities of the mother departments.
At district level, Nakasongola was the only district which consistently performed poorly in submission of timely reports in both years. The reason for this poor performance is not well known but it could be because Nakasongola is a district with several remote areas with low information access[18]. Submission of untimely reporting has been linked to health facilities located in remote areas. A study done in Solomon islands revealed that health facilities located in remote areas had challenges in submitting timely reports[19].
Kampala region did not reach the timeliness target in the period of two years. It is not certain why this region performed this way, but it could be attributed to the large volume of patients it handles because of its big population and the corresponding patient flow. Kampala is the largest city in Uganda with a population of about 1.5 million people[20]. The high workload experienced by Kampala health facilities may have an impact on timeliness of reporting. High workload is known to affect timeliness and completeness of reporting. A study done in the Oceania region in Solomon Islands about malaria surveillance reporting system in the DHSIS2 revealed that high work overload leads to delays in timely reporting [19].
At health facility level, low timeliness was observed in higher health facilities like regional referral hospitals and national referral hospitals as compared to the lower health facilities. The reason for low timeliness in higher level health facilities in Uganda is not well documented. The disease surveillance function and data reporting at higher health facilities is given as an additional task to health workers many of them clinicians who are also involved in other clinical duties. Additionally, the few available data officers at these health facilities are involved in several other duties. These could be one of contributing factors to delays in submitting reports in time.
Limitations
Our study only utilized DHIS2 information in the years of 2020 and 2021. We did not analyze reporting rates for a long duration of time that is, the years before 2020. This could have allowed us ascertain the true reporting trends over the years. We intended to analyze reporting rates during the COVID 19 period to ascertain if surveillance data reporting was affected since this period was characterized with disturbances in the health system.
Conclusion
There was good reporting in terms of completeness and timeliness in both years. However, despite the good reporting, timeliness of reporting was low in Nakasongala District, Kampala Region and in higher level health facilities. We recommend strengthening the practices leading to good reporting and offer support to health facilities with challenges to timeliness through mentorships and continuous support supervision. Further studies are needed to understand and identify barriers to timely reporting.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgements
The authors appreciate the bio-statisticians and surveillance officers who ensure that reporting of surveillance data is routinely done at their respective districts and as well as the DHIS team at the Ministry of Health for managing the DHSIS2 platform. We also appreciate Public Health Fellowship Program and the Ministry of Health, Public Health Emergency Operations Centre for the technical support and guidance offered during this study.
Copyright and licensing
All materials in the Uganda National Institute of Public Health Quarterly Epidemiological
Bulletin is in the public domain and may be used and reprinted without permission; citation as to source; however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Williams, F., A. Oke, and I. Zachary, Public health delivery in the information age: the role of informatics and technology. Perspectives in public health, 2019. 139(5): p. 236-254.
- Dureab, F., et al., Assessment of electronic disease early warning system for improved disease surveillance and outbreak response in Yemen. BMC Public Health, 2020. 20(1): p. 1422.
- Kiberu, V.M., et al., Strengthening district-based health reporting through the district health management information software system: the Ugandan experience. BMC medical informatics and decision making, 2014. 14: p. 40-40.
- Garrib, A., et al., An evaluation of the District Health Information System in rural South Africa. S Afr Med J, 2008. 98(7): p. 549-52.
- Lukwago, L., et al., The implementation of Integrated Disease Surveillance and Response in Uganda: a review of progress and challenges between 2001 and 2007. Health Policy and Planning, 2012. 28(1): p. 30-40.
- MOH, Ministry of Health Uganda: Weekly Epidemiological Bulletin; Week 4: 24th-30th Jan 2022. 2022.
- Bakamutumaho, B., et al., Severe COVID-19 in uganda across two epidemic phases: a prospective cohort study. The American journal of tropical medicine and hygiene, 2021. 105(3): p. 740.
- UBOS. Uganda Bereau of Statistics; Statistical Abstract. 2020 [cited 2022 22nd, May]; Available from: https://www.ubos.org/wp-content/uploads/publications/11_2020STATISTICAL__ABSTRACT_2020.pdf.
- Ssempiira, J., et al., Measuring health facility readiness and its effects on severe malaria outcomes in Uganda. Scientific reports, 2018. 8(1): p. 17928.
- Dehnavieh, R., et al., The District Health Information System (DHIS2): A literature review and meta-synthesis of its strengths and operational challenges based on the experiences of 11 countries. Health Inf Manag, 2019. 48(2): p. 62-75.
- Westercamp, N., et al., Effectiveness of in-service training plus the collaborative improvement strategy on the quality of routine malaria surveillance data: results of a pilot study in Kayunga District, Uganda. Malaria journal, 2021. 20(1): p. 1-12.
- Youssef, D., et al., Converting the existing disease surveillance from a paper-based to an electronic-based system using district health information system (DHIS-2) for real-time information: the Lebanese experience. BMC health services research, 2022. 22(1): p. 1-12.
- Jayatilleke, K., Challenges in implementing surveillance tools of high-income countries (HICs) in low middle income countries (LMICs). Current treatment options in infectious diseases, 2020. 12: p. 191-201.
- Karimuribo, E.D., et al., A smartphone app (AfyaData) for innovative one health disease surveillance from community to national levels in Africa: intervention in disease surveillance. JMIR public health and surveillance, 2017. 3(4): p. e7373.
- Hardhantyo, M., et al., Quality of National Disease Surveillance Reporting before and during COVID-19: A Mixed-Method Study in Indonesia. International journal of environmental research and public health, 2022. 19(5): p. 2728.
- Baine, S.O., A. Kasangaki, and E.M.M. Baine, Task shifting in health service delivery from a decision and policy makers’ perspective: a case of Uganda. Human resources for health, 2018. 16(1): p. 1-8.
- Callaghan, M., N. Ford, and H. Schneider, A systematic review of task-shifting for HIV treatment and care in Africa. Human resources for health, 2010. 8: p. 1-9.
- Majalija, S., et al., Pastoral community practices, microbial quality and associated health risks of raw milk in the milk value chain of Nakasongola District, Uganda. Pastoralism, 2020. 10(1): p. 3.
- Wangdi, K., et al., Evaluation of the malaria reporting system supported by the District Health Information System 2 in Solomon Islands. Malaria journal, 2020. 19: p. 1-14.
- Twinomuhangi, R., et al., Perceptions and vulnerability to climate change among the urban poor in Kampala City, Uganda. Regional Environmental Change, 2021. 21: p. 1-13
Comments are closed.