
The state of ambient air pollution, Kampala City, January-May 2021
Authors: Alex Ndyabakira1,2*, Daniel Kadobera1, Lilian Bulage1, Daniel A. Okello2 1 Uganda Public Health Fellowship Program, Kampala, Uganda 2 Directorate of Public Health and Environment, Kampala Capital City Authority, Kampala, Uganda
Summary
Outdoor (ambient) air pollution is increasingly associated with non-communicable diseases killing over four million people globally and over 30,000 people nationally annually[1]. Cities in sub Saharan Africa are known to have high pollution levels. We downloaded data from the air quality monitoring network for Kampala Capital City Authority (KCCA) and studied the trends of ambient air pollution. Concentrations of particulate matter (PM) 2.5, the pollutant with the greatest health hazard was largely (65-110 μg/m3) higher than the World Health Organization (WHO) cut off (24 hour mean value of 25 μg/m3) for all the sites during the observation period. Urgent community-based and inclusive initiatives are needed to address the challenge of high pollution levels in Kampala city.
Background
Even to the naked eye, the sky over Kampala city has changed in the recent past, with worsening visibility. One can no longer view the clear hills across the neighborhood. This is due to changes in concentrations of the atmospheric contents that might have led to air pollution. Air pollution is a leading cause of global disease burden, especially in low and middle-income countries[1]. Health conditions associated with air pollution exposure include: respiratory diseases such as chronic obstructive pulmonary disease (COPD), lung cancer, and acute respiratory infections in children, and cardiovascular diseases. In addition, exposure to ambient air pollution increases morbidity and mortality, and is a leading contributor to global disease burden. Given that 91% of the world’s population lives in places where air quality exceeds world health organization (WHO) guideline limits (24 hour mean value of 25 μg/m3 for PM2.5) and that at the global level, ambient air pollution leads to about 4.2 million annual deaths, pollution deserves urgent attention. Air pollution disproportionately affects the cities in the developing world where pollution levels are usually higher than the WHO cut off. Moreover, this causes double burden of disease given that communicable diseases are highly prevalent in developing countries.
Although many substances are known to potentially contaminate air, the WHO has identified carbon monoxide (CO), particulate matter (PM), ozone (O3), nitrogen dioxide (NO2), and sulfurdioxide (SO2) as the pollutants with greatest public health importance. The United States (US) National Ambient Air Quality Standard (NAAQS) designates all of the above plus airborne lead (Pb) as criteria pollutants. In order to promote and protect public health, the WHO and the US Environmental Protection Agency (USEPA) have defined guideline limits for the pollutants that should not be exceeded[2]. The WHO limits for PM2.5, the pollutant with the greatest health risks due to its ability to cross lung tissue and enter blood circulation is 25 μg/m3 (24-hour mean) while the limits for the same pollutant set by the USEPA is 35 μg/m3 (24-hour mean). Data on the magnitude of air pollution in African cities is limited, particularly as it relates to Sub-Saharan Africa. The WHO database provides an average PM2.5 value for Africa of 78 μg/m3 annual mean (which is three times the set limit) and may be worse for Sub-Saharan Africa where Kampala city falls. A study conducted in the cities of Kampala and Jinja in 2015 revealed that the mean concentrations of PM2.5 were 132.1 μg/m3 and11.4 μg/m3, respectively[3]. This mean PM2.5 concentration is 5.3 times the WHO cut-off limits. Another study done in Mpererwe, Kampala city suburb done earlier in 2014 had found similarly very high levels of pollutants[2].
Given that the number of vehicles has been increasing (with worsening idling in jam) coupled with government’s policy on industrialization, the concentration of PM2.5 is expected to have increased. We established the spatial variation and trends of ambient air pollution for Kampala city, January –May, 2021.
Methods
Study setting
We conducted the study in Kampala city. Kampala, like other fast-growing African cities is affected by high levels of pollution and consequently poor air quality. Kampala city has about 23% of its area fully urbanized, 60% semi-urbanized, and 17% considered rural. The city’s day and night population are 3 million and 1.5 million people, respectively. The average annual temperature is 21.9° C and relative humidity ranges from 53–89%. This reflects on the likely extent of human activity that results in air pollutant generation.
Study design
We used spatial, longitudinal calibrated air quality monitoring data obtained from the 24 air quality monitors deployed across Kampala City by the City Authority, January- May 2021. Monitor readings are calibrated based on the BAM (beta attenuated monitor) station at Nakawa, one of the five KCCA urban division headquarters. These monitors take continuous readings for main pollutants, temperature, and humidity.
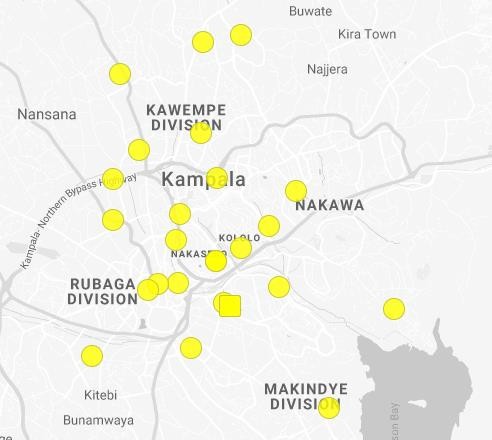
Kampala City Council Authority has been monitoring the status of air quality across the city since 2019. The monitors are well situated across the city to represent different land use patterns as well as places prone to idling of cars during rush hour (Figure 1). These are low cost monitors which measure temperature, humidity, and ambient air concentrations of pollutants. These data are then calibrated based on a standard monitor (BAM) before being relayed via the internet for download on a computer. These data can be downloaded at resolution of reading per minute, hour 24 hour or monthly mean. An analytics platform is included for easy data visualization even to a non-technical person. The concentrations of the pollutants are converted into an air quality index, which is color coded on a continuum from green (healthy air) to purple (hazardous air) to guide citizens on choice of timing for different activities such as Exercise.
Study variables and data analysis
We obtained data on air PM 2.5 and analyzed these using STATA 14. Data was downloaded at a resolution of 24 hours and therefore 24-hour means (daily averages) were used. We established trends of levels of PM2.5 and exceedances (in the past 28 days, the number of days for which the pollution level exceeds the WHO PM2.5 cut off) and displayed the information on graphs against the WHO cut off as reference per site for selected locations. Exceedances were categorized into unhealthy for sensitive groups such as persons with allergic airway conditions like asthma (>40-65 μg/m3), unhealthy for all persons (>65-150 μg/m3), very unhealthy (>150-250 μg/m3), and hazardous (>250-350 μg/m3).
Ethical considerations
We did not seek ethical approval for this assessment. The assessment is based on routine air quality monitoring data generated by KCCA. It does not contain any personal identifiers. However, we sought and obtained permission from KCCA to access and use the data to inform air quality improvement interventions in Kampala city.
Results
Mean pollution levels in selected areas, Kampala City, January-May, 2021
Over all, the pollution levels in Kampala exceed WHO cut offs most of the time. Throughout the study period, the average level of pollution was higher than the WHO cut off (25micrograms/cubic metre) (Figure 2). All sites recorded an average daily value of more than twice the WHO cut off. Sites with less human activity tended to have lower average levels of pollution as compared to city center for instance the pollution levels in Kyanja remained lower than those of Bwaise, a busy city suburb during the whole observation period (Figure 2).

Mean particulate matter 2.5 exceedances, May 2021
The mean PM exceedances over the last 28 days (during the month was May) was either unhealthy for sensitive groups or unhealthy with more than 50% of the time registering unhealthy for all city residents in all monitoring sites except Bwaise surbub. In Bwaise, it was over 90% unhealth for all city residents and very unhealthy 10% of the time (Figure 3).
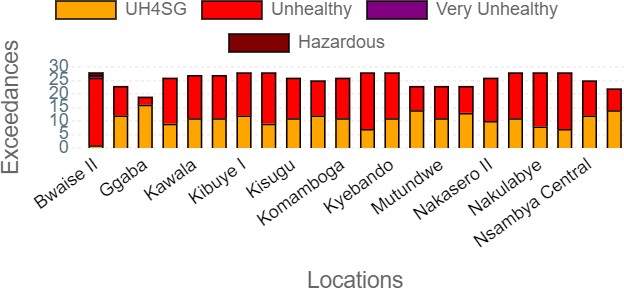
UH4SG=Unhealthy for sensitive group
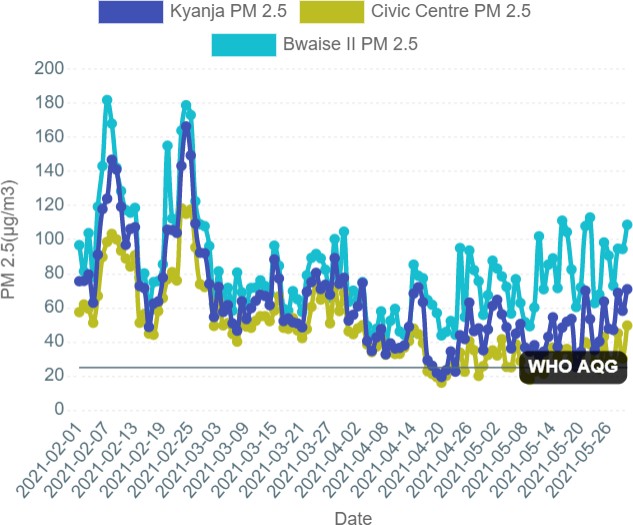
Trend of mean 24-hour particulate matter 2.5 levels in selected areas, January- May, 2021
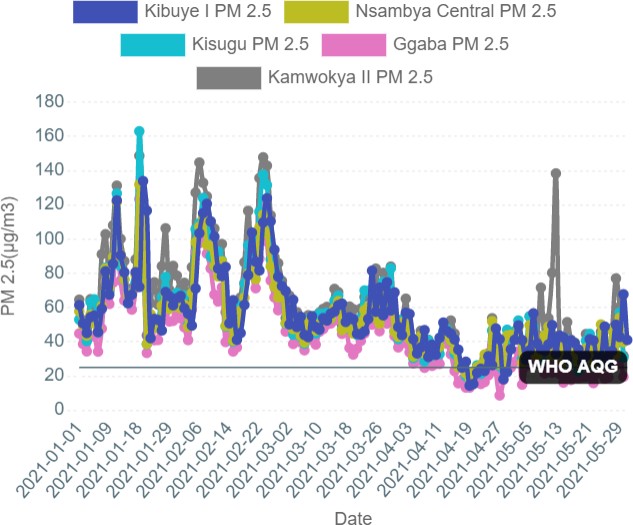
The pollution levels in the green upscale Kampala (civic center) remained lower than for Kyanja residential area with unpaved roads and Bwaise suburb which has many human activities including traffic idling due to jam, manufacturig plants, and some unpaved roads (Figure 4). The levels of PM2.5 remained consistently above the WHO threshold during the observation perid except at Kyanja and civic center sites during late April-early May.
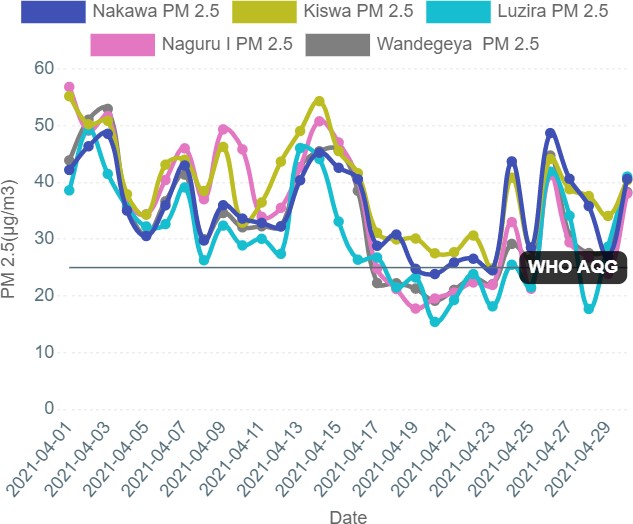
Similar to Figure 4 trends, PM2.5 levels remain higher than the WHO threshold most of the time except during April-May rainy season. Sites with busy human activity such as trading centers, areas prone to jam or with manufacturing plants consistently recorded higher pollution levels compared to residential or the leafy upscale Kampala (Figure 5 and 6).
Discussion
Throughout this observation period, the average level of pollution was higher than the WHO cut off (25micrograms/cubic metre), potentially putting the health of city dwellers at stake. The WHO and US Environmental protection agency put standards for common air pollutants including ozone, nitrogen oxides, and particulate matter to guide countries and cities. Largely in monitored cities, over 80% exceed the cut offs potentially exposing over 90% of the dwellers to unhealthy air. Ambient (outdoor) air pollution is hazardous as it leads to non-communicable diseases in the cardiorespiratory system.
In Kampala city and most of Africa, particulate matter 2.5 (PM 2.5) with the ability to enter the blood stream is the most hazardous. Due to idling of cars in jam around road junctions, road construction and construction sites generating dust participles, unpaved roads, poor waste disposal through burning that generates fumes, and location of factories/manufacturing plants release pollutants into the atmosphere.
These collectively contribute to formation of PM2.5 and PM10 the pollutants of greatest importance. Idling cars also release significant Nitrogen oxides that may also contribute to PM 2.5 if acted upon by environment forms PM2.5. To minimize the effects of pollution on health monitoring of pollutant concentrations, evidence basic interventions and monitoring progress are key.
The city authority has embarked on developing a clean air action that spells out the activities to combat air pollution the city. Some interventions such as paving of roads, non-motorized ways, tree planting, adoption of cleaner energies such as electric transport and cooking, regulation of the construction industry are already underway. Additional steps include the air quality management regulation by national environment management authority which spells out penalties to offenders such as factories emitting beyond the limits.
With such levels of pollution in a densely populated city, it is important that every one is rallied behind addressing the causes. Human-centered designed projects are urgently needed to address obvious health hazard. For instance having low air pollution in the upscale Kampala which also has many trees suggests that planting trees in Kampala may reduce air pollution significantly
Conclusion
This assessment shows that pollution in Kampala city exceeds the WHO cuts potentially putting the health of city residents at risk. Urgent community centered solutions are needed to collectively address this problem
Acknowledgement
We appreciate the support from the partners of the air quality monitoring network at KCCA including Airqo, Clarity movement inc, National Environmental management Authority, and US Embassy in Kampala. We are also grateful to the support rendered by the Uganda Public Health fellowship program during the data analysis and writing.
References
- Organization, W.H., Global health risks: mortality and burden of disease attributable to selected major risks. 2009: World Health
- Schwander, S., et al., Ambient particulate matter air pollution in Mpererwe District, Kampala, Uganda: A pilot study. Journal of environmental and public health, 2014.
- Kirenga, B.J., et al., The state of ambient air quality in two Ugandan cities: a pilot cross-sectional spatial assessment. International journal of environmental research and public health, 12(7): p. 8075-8091.
Read and download full article below;
Reference this page as below
Alex Ndyabakira1,2*, Daniel Kadobera1, Lilian Bulage1, Daniel A. Okello2. The state of ambient air pollution, Kampala City, January-May 2021. Kampala, Uganda National Institute of Public Health. 2021 June 3oth. Available from:https://uniph.go.ug/the-state-of-ambient-air-pollution-kampala-city-january-may-2021.
Comments are closed.