
Measles outbreak investigation in Kumi District, Uganda, May–July 2025
Authors: Kyomugisha D. Aman1*, Paul Okello1, Yasiini Nuwamanya2, Sharon Namasambi1, Deborah Aujo1, Vianney John Kigongo1, Benon Kwesiga1, Richard Migisha1. Institutional Affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Ministry of Health, Kampala, Uganda. 2Uganda National Expanded Program on Immunization, Ministry of Health, Kampala, Uganda. Correspondence*: Tel:+256759803507, Email: akyomugisha@uniph.go.ug.
Summary
Background: In July 2025, Kumi District in Eastern Uganda reported a Measles outbreak among children admitted in high-volume healthcare facilities. We investigated to determine the scope of the outbreak, identify risk factors for transmission, and recommend evidence-based control measures.
Methods: A suspect case was acute onset of fever and maculopapular rash with ≥1 of cough, coryza, or conjunctivitis in a Kumi District resident from 1 May–31 July 2025. A confirmed case was suspected case with a positive measles-specific IgM test. We reviewed health facility records and conducted community case searches. We conducted descriptive epidemiology, environmental assessment, and an age-matched case-control study (1:2) to identify risk factors for transmission. Vaccine coverage and effectiveness were estimated for the first Measles vaccine dose (MR1).
Results: We identified 177 cases, including 6 (3%) confirmed and 2 (1.1%) deaths. Among the cases, 104 (61%) were vaccinated with one dose. Children aged 6–8 months (AR=41/10,000), males (AR=7/10,000) and Northern Division (AR=76/10,000) were most affected. Poor isolation and triage practices were observed in high-volume healthcare facilities. Visiting healthcare facilities (aOR=20, 95% CI:5.9–70), playing around neighbouring homes (aOR=5, 95% CI:1.2–21), and attending religious gatherings increased odds of infection (aOR=1.9, 95% CI:1.03–3.5). Vaccination with ≥1 dose was protective (aOR=0.35, 95% CI:0.16-0.77). Vaccine coverage among controls was 73% for MR1 and 13% for MR2. Vaccine effectiveness for MR1 was 65% (95% CI:23–84).
Conclusion: Sub-optimal vaccine coverage and poor isolation and triage practices in healthcare facilities fueled transmission of measles in this outbreak. We recommended mass vaccination to increase vaccination coverage and refresher trainings for health workers emphasizing effective infection prevention and control.
Introduction
Measles is a highly infectious disease caused by Measles virus and has an incubation period ranging from 7–21 days. Measles presents with fever, maculopapular skin rash, coryza, cough and conjunctivitis ((1)). It is transmitted from person to person through respiratory droplets or direct contact.
Measles is a leading cause of deaths globally, with more than 95% of the deaths occurring in developing countries and its case fatality is usually between 0.1% in developed settings to 30% in refugee settings (1–3). Measles vaccination has been found to be effective in preventing Measles transmission and 82 countries have been able to achieve Measles elimination (4). Measles vaccination is 93% effective at preventing Measles after 1 dose of vaccine and approximately 97% effective after 2 doses (5). Measles vaccination coverage of over 95% for both doses should be attained in order to achieve HERD immunity ad therefore prevent community transmission (1).
On 1 July, 2025, the Kumi District Health Officer received an alert from the in-charge of Kumi HC IV. They had noticed an influx of suspected Measles cases on the paediatrics in-patient ward at Kumi HCIV. Blood samples tested positive for Measles antibodies and this confirmed an outbreak. We investigated to determine the scope of the Measles outbreak, identify risk factors for transmission and recommend evidence-based control measures in Kumi District.
Methods
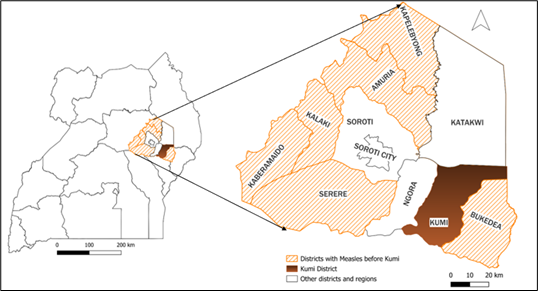
Kumi District is situated in Eastern Uganda, forming part of the Teso Sub-region. It is bordered by Katakwi in the North, Bukedea in the East, Ngora in the West and Pallisa in the South. Kumi District has a population of 286,992; which is largely rural across the 14 sub-counties and 4 town councils; with the district headquarters in Southern Division. Prior to Kumi declaring an outbreak, 6 other districts within Teso Sub-region had reported measles outbreaks including; Bukedea, Serere, Kaberamaido, Kalaki, Amuria, and Kapelebyong.
We defined a suspected Measles case as acute onset of fever and maculopapular rash, with at least one of the following symptoms: cough, runny nose (coryza) or conjunctivitis in a resident of Kumi District from 1 May, 2025 to 31 July, 2025.
A confirmed case was defined as a suspected case that had tested positive for IgM Measles-specific antibody test.
We line listed suspected measles cases by reviewing records at 3 high volume healthcare facilities. We conducted active case search in healthcare facilities and communities.
We conducted descriptive epidemiology of the identified cases. We then visited the Measles isolation ward at Kumi HC IV to observe triage and isolation practices. We also observed interactions of children in the community.
We conducted 56 hypothesis generating hypotheses to identify potential exposure factors that could have occurred within a 21-day period prior to onset of symptoms. The exposures of interest included not being vaccinated, visiting a health facility, receiving a visitor from another district, visiting a communal water collection point, travelling to another district and attending a religious gathering or burial. We also discussed with the district health team about potential exposures.
We conducted a 1:2 age-matched case control study in Northern Division, the most affected subcounty, to test the hypotheses that were generated. We interviewed 105 cases and 210 controls. Controls were selected randomly from neighbourhood households which had no case from 1 May 2025 to 31 July 2025.
We assumed that the controls are representative of the general population and estimated vaccine coverage amongst the controls with the following formula;
Vaccine coverage () 100
We estimated vaccine effectiveness for MR1 vaccine with the following formula;
Vaccine effectiveness ()
Where is the adjusted odd ratio of receipt of one vaccination dose.
The outbreak investigation was conducted in response to a public health emergency on behalf of the National Rapid Response Team of the Ministry of Health in Uganda. Kumi District Health Office and Chief Administrative Office granted local approval to investigate. The Office of the Associate Director for Science at the US Centres for Disease Control and Prevention (CDC) Uganda determined that this investigation was non-research and that its primary intent was public health practice or disease control. Verbal informed consent was obtained from participants or guardians as proxy for minors prior to the start of each interview.
Results
Descriptive epidemiology
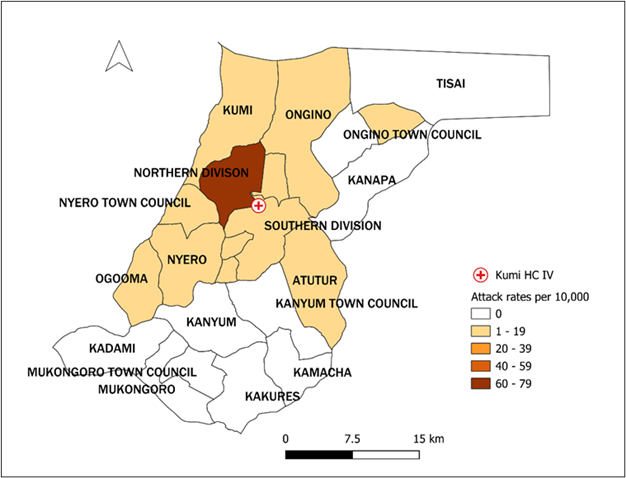
Between 1 May 2025 and 31 July 2025, we identified 177 cases of which 6 (3%) were confirmed and 2 (1%) died. The majority of cases (105, 70%) had received ≥1 dose of MR vaccine. Children aged 6-8 months (AR=41/10,000) and those aged 9-59 months (AR=24/10,000) were the most affected. Males (AR=7/10,000) were slightly more affected than females (6/10,000). The most affected sub-counties were Northern Division (AR=76/10,000) and Ogooma sub-county (AR=10/10,000) (Figure 2). In addition to fever and rash, the majority (>80%) also presented with cough and coryza.
The epidemic curve (Figure 3) shows a protracted outbreak from May–July 2025. The outbreak started with sporadic cases linked to attendance of religious gatherings that had symptomatic children followed by clusters related to symptomatic visitors from affected neighbouring districts and then widespread community transmission propagated by hospital exposure in high volume healthcare facilities. There was a mass vaccination campaign in response to widespread community transmission.
Environmental assessment findings
At Kumi HC IV, we observed that suspected measles patients were mixed with other patients within the inpatient ward during drug dispensing and there was unrestricted access to the isolation ward which also served as a walkway to public toilets. In the community, symptomatic children were playing freely with healthy children.
Hypothesis generation findings
Of the 56 hypothesis generating interviews conducted, 68% had received at least one dose of Measles vaccine. We hypothesized that attending religious or social gatherings (66%), visiting a health facility (32%) and not being vaccinated (32%) during the exposure period were potentially associated with an increased risk of measles transmission.
Case-control investigation findings
Among those interviewed, 215 (68%) of respondents had history of receiving ≥1 MR vaccination. Vaccination (aOR=0.4, 95%CI=0.2–0.8), visiting a health facility during the exposure period (aOR=20, 95%CI=5.7–71), playing around neighbouring homes during the exposure period (aOR=5.7, 95%CI=1.4–24) and attending a religious gathering during the exposure period (aOR=1.9, 95%CI=1.03–3.5) were significantly associated with measles transmission in Kumi District (Table 1).
Vaccine coverage and effectiveness
The estimated vaccine coverage of 73% among controls who had history of receiving ≥1 MR vaccine dose. The estimated vaccine effectiveness was 65% (95%CI=23-84).
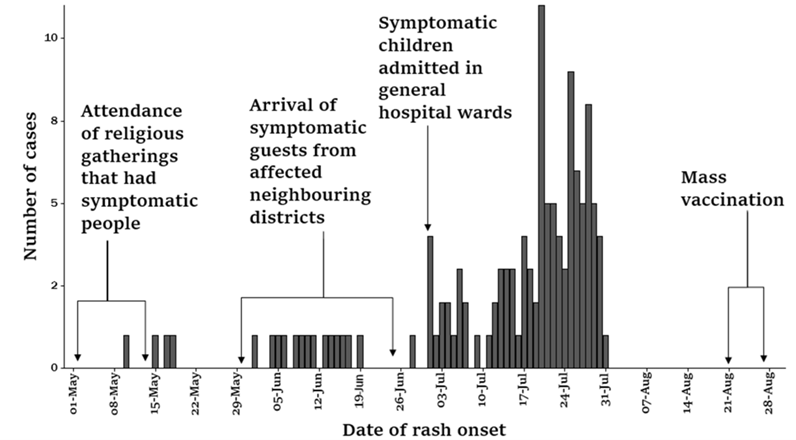
Table 1: Risk factors for Measles transmission in Kumi District, May-July 2025
| Exposures | Cases
n (%) |
Controls
n (%) |
cOR (95% CI) |
aOR (95% CI) |
| Vaccination | ||||
| No | 43 (41) | 57 (27) | Ref | Ref |
| Yes | 62 (59) | 153 (73) | 0.3 (0.2–0.7) | 0.4 (0.2–0.8) |
| Visited health facility in exposure in exposure period | ||||
| No | 272 (86) | 199 (95) | Ref | Ref |
| Yes | 43(14) | 11 (5) | 18 (5.43–59) | 20 (5.7–71) |
| Play area in exposure period | ||||
| At home | 91 (87) | 202 (96) | Ref | Ref |
| Away from home | 14 (13) | 8 (4) | 5.8 (1.9–18) | 5.7 (1.4–24) |
| Attended social gatherings in exposure period | ||||
| None | 35 (34) | 110 (52) | Ref | Ref |
| Burials | 6 (6) | 1 (0.5) | 15.2 (1.8–128) | 2.9 (0.2–33) |
| Religious | 57 (56) | 87 (41) | 2 (1.2–3.3) | 1.9 (1.03–3.5) |
| Multiple | 4 (4) | 12 (5.7) | 1 (0.3–3.3) | 0.8 (0.2–3.3) |
| cOR – Crude Odds Ratio aOR – Adjusted Odds Ratio |
Discussion
This investigation confirmed a protracted measles outbreak in Kumi District driven by significant immunity gaps and high-risk social and clinical exposures. Between
May–July 2025, children aged 6-59 months were most affected. Key drivers of transmission included suboptimal vaccine coverage and effectiveness alongside intense exposure at healthcare facilities, within community through play and at religious gatherings.
Children below the age of vaccination were vulnerable due to early waning of maternal antibodies as suggested in some studies (6)Vaccination was protective; however, the estimated coverage among controls was below the ≥95% threshold required for herd immunity (7–9). These findings suggest that the population remained highly vulnerable due to high numbers of unvaccinated children. The accumulation of susceptible individuals contributed to the magnitude and duration of the outbreak (3,4).
Health facility exposure emerged as the dominant transmission pathway. Environmental assessments revealed gaps in infection prevention and control with mixing of suspected measles patients with other patients and ineffective isolation. These findings highlight high-volume healthcare facilities as amplification points as reported in other studies (10–13).
Social interactions played a significant role in propagating the virus as symptomatic children interacted freely at religious and neighbourhood gatherings as reported in other studies in Uganda (14).
Study limitations
Not all suspected cases were laboratory confirmed, which may have resulted in misclassification. Vaccination status was partly based on caregiver recall when vaccination cards were unavailable, introducing potential reporting inaccuracies. Exposure histories were collected retrospectively and may have been affected by recall bias. The analytical study was conducted in the most affected sub-county, which may limit generalizability to the entire district.
Conclusion
We confirmed a propagated measles outbreak that was amplified by gaps in infection prevention and control in health facilities, as well as by community interactions in areas with sub-optimal immunization coverage.
Public health actions
Following the dissemination of our findings, a district-wide mass measles vaccination campaign was conducted on 21–25 August 2025 following this investigation.
Recommendations
District health authorities could provide refresher training to strengthen infection prevention and control practices in pediatric wards. Targeted mop-up vaccination activities could increase MR1 and MR2 coverage in affected communities. Health facilities could strengthen triage, isolation, and patient-flow systems, while surveillance teams could enhance early detection and rapid response to prevent similar outbreaks.
Conflict of interest
The authors declare that they had no conflict of interest.
Authors’ contribution
KDA conceived, designed, analyzed, interpreted the study and wrote the draft bulletin. KDA, PO, SN, DA conducted the investigation and contributed to report writing, VJK reviewed the draft bulletin. YN, BK, RM reviewed the bulletin to ensure intellectual content.
Acknowledgments
The authors convey their gratitude to the Ministry of Health through Uganda National Expanded Program for Immunization (UNEPI) for the technical support provided, Kumi District leadership for the approvals and leading this investigation in the district. We also thank the staff at Kumi Health Centre IV, health inspectors and Village Health Teams for the assistance in identifying and interviewing cases and controls.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission. However, citation as to source is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Do LAH, Mulholland K. Measles 2025. New England Journal of Medicine. 2025 Jun 25. doi:10.1056/NEJMRA2504516
- Measles [Internet]. [cited 2025 Aug 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/measles
- Measles vaccines WHO Position Paper – April 2017 [Internet]. Available from: http://www.who.int/wer
- Minta AA, Ferrari M, Antoni S, Lambert B, Sayi TS, Hsu CH, et al. Progress Toward Measles Elimination — Worldwide, 2000–2023. MMWR Morb Mortal Wkly Rep. 2024 Nov 14;73(45):1036–42. doi:10.15585/MMWR.MM7345A4 PubMed PMID: 39541251.
- Questions About Measles | Measles (Rubeola) | CDC [Internet]. [cited 2025 Oct 9]. Available from: https://www.cdc.gov/measles/about/questions.html
- Waaijenborg S, Hahné SJM, Mollema L, Smits GP, Berbers GAM, Van Der Klis FRM, et al. Waning of Maternal Antibodies Against Measles, Mumps, Rubella, and Varicella in Communities With Contrasting Vaccination Coverage. J Infect Dis. 2013 Jul 1;208(1):10. doi:10.1093/INFDIS/JIT143 PubMed PMID: 23661802.
- Okiror Okello E, Migisha R, Ampaire I, Nsubuga F, Nalwanga J, Kwizera P, et al. Measles outbreak investigation in Kakumiro District, Uganda, February–May 2024. Discover public health. 2025 Dec 1;22(1). doi:10.1186/s12982-025-00446-4
- Oduoye MO, Zuhair V, Marbell A, Olatunji GD, Khan AA, Farooq A, et al. The recent measles outbreak in South African Region is due to low vaccination coverage. What should we do to mitigate it? New Microbes New Infect. 2023 Sep 1;54:101164. doi:10.1016/J.NMNI.2023.101164 PubMed PMID: 37455850.
- Bello IM, Akpan GU, Teshager HF, Jepkorir LE, Girma MB. Factors influencing recurrent measles outbreak in Ethiopia among under-five children: a systematic review. PAMJ-OH 2024; 15:7. 2024 Oct 11;15(7). doi:10.11604/PAMJ-OH.2024.15.7.43800
- Biribawa C, Atuhairwe JA, Bulage L, Okethwangu DO, Kwesiga B, Ario AR, et al. Measles outbreak amplified in a pediatric ward: Lyantonde District, Uganda, August 2017. BMC Infect Dis. 2020 Jun 5;20(1):1–8. doi:10.1186/S12879-020-05120-5/FIGURES/3 PubMed PMID: 32503450.
- Torner N, Ferràs J, Curto L, Rebull J, Sol J, Costa J, et al. Measles outbreak related to healthcare transmission. Vacunas. 2021 Jan 1;22(1):20–7. doi:10.1016/J.VACUN.2020.08.002
- Mfitundinda E, Migisha R, Mary Namusisi A, Wenani D, Kwesiga B, Ayeerwot R, et al. Investigation of a cross‑border measles outbreak in Moroto District, northeastern Uganda, March–September, 2024 [Internet]. Vol. 22. 123AD;22:267. doi:10.1186/s12982-025-00581-y
- Nsubuga F, Bulage L, Ampeire I, Matovu JKB, Kasasa S, Tanifum P, et al. Factors contributing to measles transmission during an outbreak in Kamwenge District, Western Uganda, April to August 2015. BMC Infect Dis. 2018 Jan 8;18(1):1–7. doi:10.1186/S12879-017-2941-4/TABLES/5 PubMed PMID: 29310585.
- Measles outbreak Investigation in Terego District, Uganda, May- June, 2024. – UNIPH [Internet]. [cited 2025 Dec 10]. Available from: https://uniph.go.ug/measles-outbreak-investigation-in-terego-district-uganda-may-june-2024/
Comments are closed.