
Temporal and Spatial Comparison of Malaria Incidence Between Urban and Rural Areas in Uganda, 2020–2024
Authors: Maria Nakabuye1, Michael Mutegeki1, Charity Mutesi1, Ronald Elly Kimuli², Gerald Rukundo², Benon Kwesiga1, Richard Migisha1 Institutional affiliations:1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, ²Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256 706233470, Email: nakabuyemaria.mn@uniph.go.ug
Summary
Background: Although malaria has traditionally affected rural populations, recent evidence indicates increasing transmission in rapidly growing urban areas of sub-Saharan Africa. We compared the spatial and temporal distributions of malaria incidence in urban and rural Uganda to inform targeted interventions.
Methods: We analyzed monthly District Health Information Software-2 (DHIS2) malaria data (2020–2024) for 10 cities and their corresponding districts in Uganda. Urban areas were city divisions and district town councils. Rural areas were sub-counties from the districts corresponding to each selected city. To calculate annual malaria incidence per 1,000 population, we abstracted monthly data of malaria confirmed outpatient cases from DHIS2 as the numerator and population data was obtained from Uganda Bureau of Statistics as the denominator. A linear regression model with a year × setting interaction term assessed differences in incidence trends between rural and urban settings.
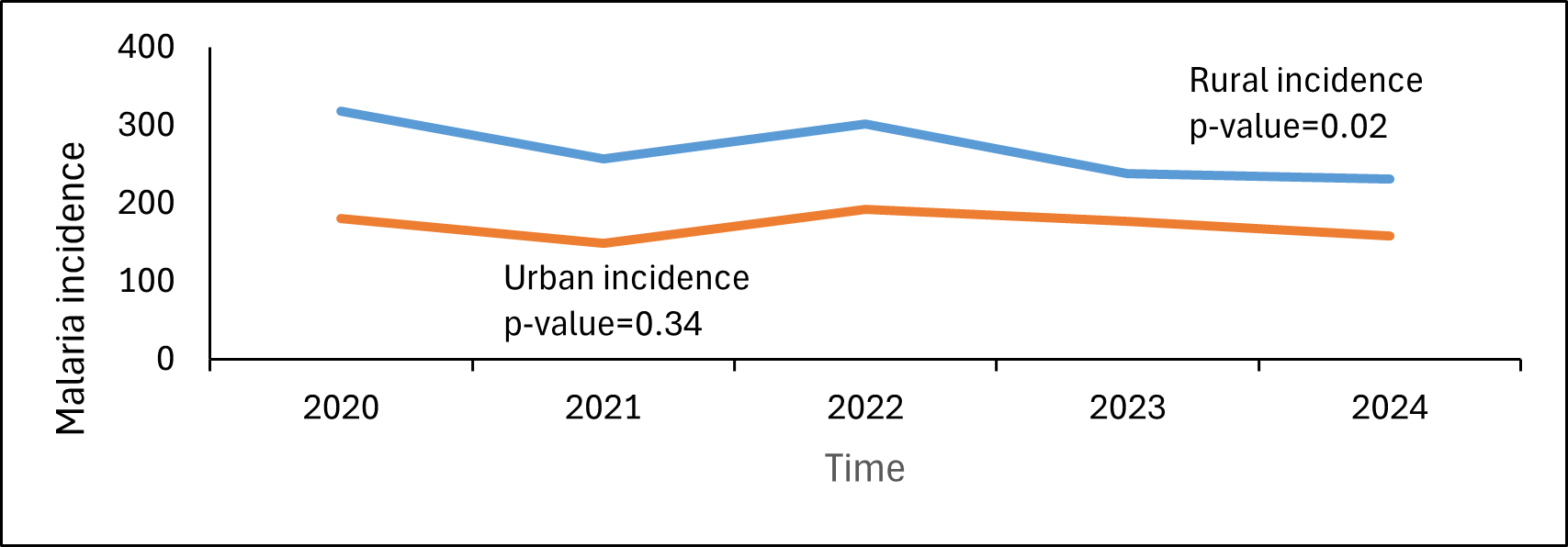
Results: Malaria incidence trend differed significantly between settings (interaction p=0.047) with rural setting showing a higher incidence. Rural incidence declined (p-value=0.02) from 318 (573,115/1,800,600) to 254 (460,619/1,814,024) while urban incidence decreased from 249 (606,421/2,434,300) to 198 (544,457/2,744,443) per 1,000 population though not significantly. We observed spatial variation, with rural areas such as Gulu (mean incidence of 810 per 1,000 population) and Lira districts (281 per 1,000 population) showing high burden, and persistent urban hotspots like Soroti City, which recorded a mean incidence of 949 per 1,000 population.
Conclusion: Rural Uganda continues to carry a higher burden and experienced a more significant decline than urban areas. Localized urban hotspots exist. Uganda should sustain vector control and case management in rural areas while implementing targeted surveillance-driven interventions in urban hotspots focused on hotspot identification, improved housing and drainage of breeding sites.
Background
Uganda is among the countries with the highest malaria burden globally. Malaria remains endemic throughout the country and is a leading cause of morbidity and mortality, accounting for approximately 30-40% of outpatient visits(1).
Global malaria control and elimination strategies emphasize the scale-up of key interventions such as insecticide-treated nets, indoor residual spraying, malaria chemoprevention, and prompt diagnosis and treatment alongside strengthened malaria surveillance systems to guide targeted interventions. In Uganda, these interventions have contributed to reductions in malaria burden in several parts of the country, however, their implementation has largely focused on high-transmission rural districts where malaria burden has historically been greatest (1).
Historically, malaria has been considered a disease that disproportionately affects rural populations, particularly those with limited access to healthcare, preventive measures, and adequate housing (2). However, malaria risk is closely linked to socio-economic conditions such as poverty, housing quality, and access to healthcare, which may affect vulnerable populations in both rural and urban settings (3-6).
In some contexts, urban malaria remains a substantive threat, with incidence rates that are higher than those reported in rural areas. One systematic review noted that prevalence estimates in urban areas ranged from as low as 0.06% to as high as 58%, with many studies reporting 10 and 30% (7). Factors such as unplanned urban growth, informal settlements, poor drainage, standing water from construction activities, and migration from high-transmission rural areas may sustain or even increase malaria transmission in these environments (8-10). We determined the burden and compared incidence trends of malaria in rural versus urban settings in Uganda from 2020 to 2024.
Methods
This was a descriptive study of monthly, routinely collected malaria surveillance data submitted into District Health Information Software-2 (DHIS2) by health facilities in Uganda cities and their respective districts using malaria confirmed outpatient cases recorded in the Health Management Information System (HMIS)-105 from 2020 to 2024.
We stratified study locations into urban and rural areas in accordance with the classification framework of Uganda Bureau of Statistics (UBOS). Urban areas were defined as city divisions for all Ugandan cities (except Kampala City since it doesn’t have a corresponding district) and district town councils within the districts corresponding to each selected city. For comparison, rural areas were defined as sub-counties within the same districts corresponding to each selected city. For each district, rural malaria incidence was computed using data from all sub-counties excluding the city divisions and town councils classified under the urban category. We compared data of 10 cities and their corresponding districts. Cities included; Lira, Gulu, Soroti, Fort portal, Masaka, Mbarara, Hoima, Arua, Mbale and Jinja. The corresponding districts were; Lira, Gulu, Soroti, Kabarole, Masaka, Mbarara, Hoima, Arua, Mbale and Jinja.
We abstracted monthly data of confirmed outpatient malarias from DHIS-2 at division, sub-county, and town council level. Population data to calculate incidence was obtained from UBOS from 2020 to2024. We calculated annual malaria incidence using the malaria confirmed outpatient cases as the numerator and the respective population estimates as the denominator, per 1000 population. Line graphs were used to visualize temporal trends of malaria incidence across both urban and rural areas and these were disaggregated by sex and age. Age was categorized into age categories <5 years and ≥5 years. The seasonal Mann-Kendall test was used to test for significance of trends in malaria incidence. We used linear regression to test whether malaria incidence trends differed between urban and rural areas. We drew choropleth maps using Quantum Geographic Information System (QGIS) to show the spatial distribution of annual malaria incidence across the Ugandan cities corresponding districts.
Results
Between 2020 and 2024, a total of 3,698,997 malaria cases were reported in urban areas and 2,542,090 malaria cases in rural areas. In urban settings, malaria incidence declined (p-value=0.34) from 249 per 1,000 population (606,421/2,434,300) in 2020 to 198 per 1,000 population (544,457/2,744,443) in 2024. In rural settings, malaria incidence reduced (p-value=0.02) from 318 per 1,000 population (573,115/1,800,600) to 254 (460,619/1,814,024) per 1,000 population between 2020–2024 (Figure 1). The trend in malaria incidence differed between rural and urban areas since the interaction between year and setting was statistically significant (p=0.047).
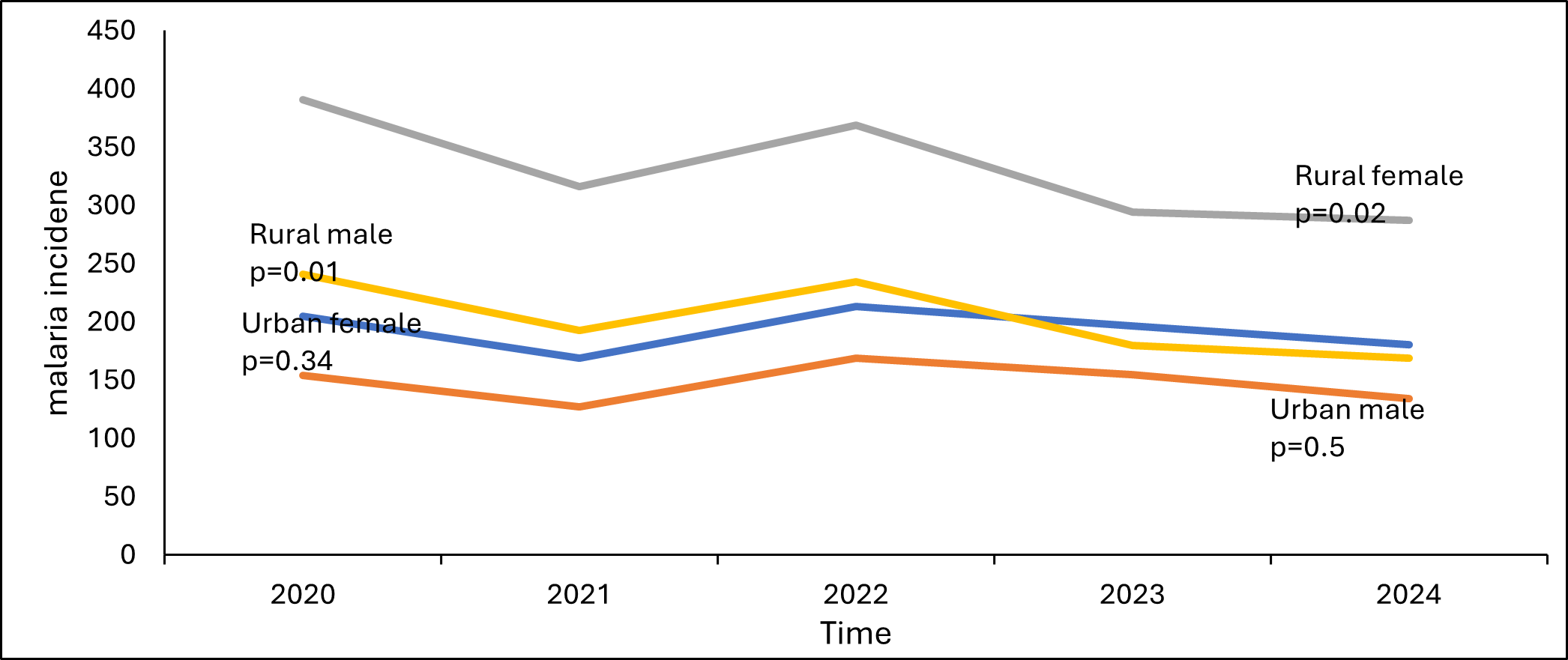
Both males and females demonstrated declining trends in rural and urban areas. Although incidence remained consistently higher among males and females from rural areas compared to their urban counterparts, rural populations experienced a statistically significant malaria incidence decline, with females showing a reduction from 393 (357,944/911,800) to 306 (292,302/955,290), p=0.02 and males from 242 (215,171/888,800) to 196 (168,317/858,734), p=0.01 (Figure 2).
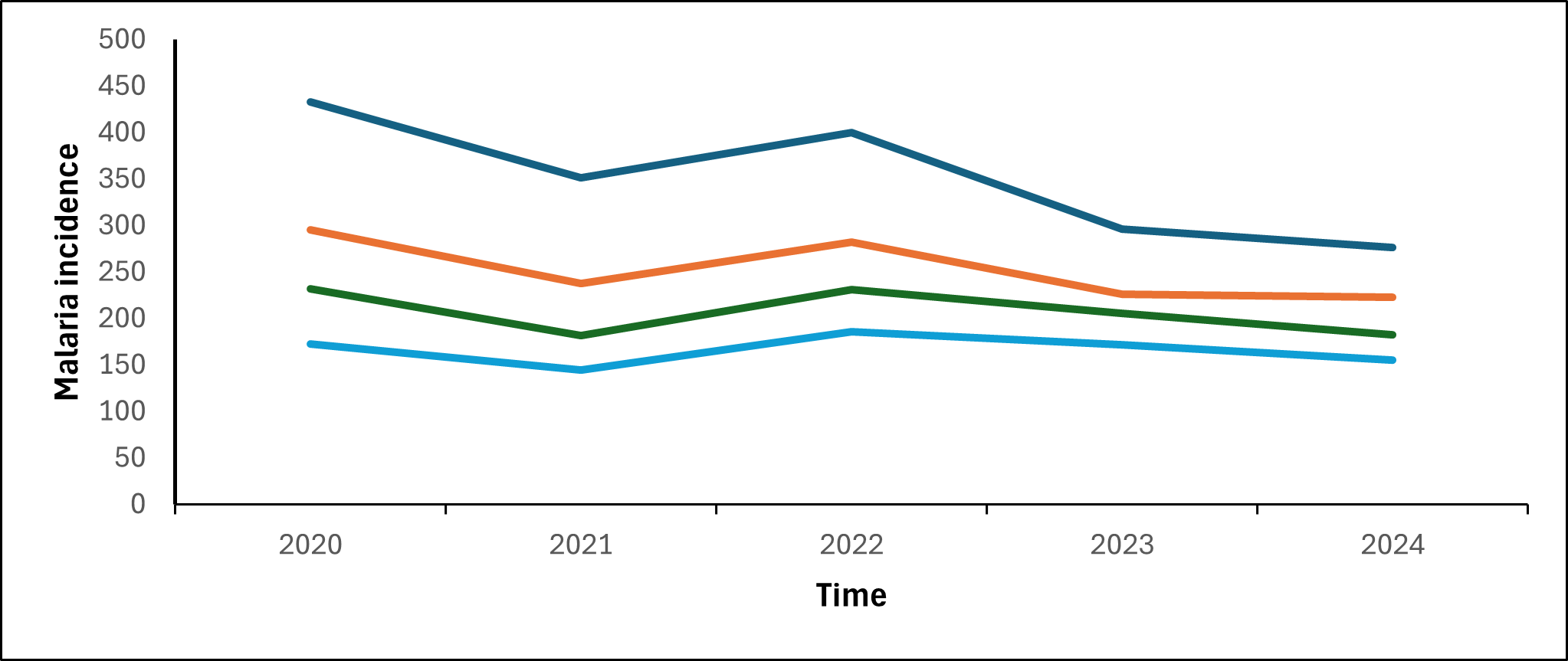
Malaria incidence declined over time in both children <5 years and individuals aged ≥5 years across rural and urban areas. Although incidence remained consistently higher in rural populations compared to their urban counterparts, the decline in rural areas was statistically significant, with reductions observed among <5 years from 433 (129,450/298,900) to 303 (91,301/301,128), p=0.02 and individuals ≥5 years 295 (443,665/1,501,700) to 244 (369,318/1,512,896), p=0.02 (Figure 3).
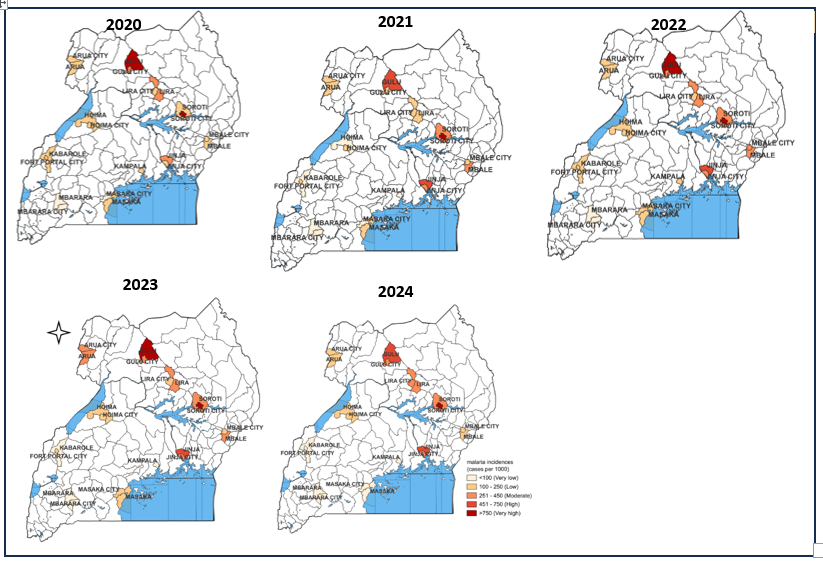
Over the study period, Gulu District, Soroti City, and Lira District consistently reported the highest malaria incidence. In most settings, urban areas exhibited lower incidence than their corresponding districts, including Gulu, Lira, Mbale, Jinja, and Fort Portal cities. Arua, Hoima, Masaka, and Mbarara cities showed incidence comparable to their respective districts. Soroti City consistently experienced higher malaria incidence than its corresponding district throughout the study period (Figure 4).
Discussion
Malaria incidence in Uganda declined between 2020 and 2024 in both urban and rural areas, the declines may reflect intensified vector control and case management interventions in high-burden districts, including indoor residue spraying in targeted districts, long-lasting insecticide nets distribution cycles, and improved diagnostic access. The rural burden remained higher than urban areas throughout the study period. Previous studies have reported rural environments to present with greater ecological suitability for malaria transmission due to factors such as extensive vegetation, agricultural activities, and greater availability of mosquito breeding sites (11, 12).
Sex-disaggregated patterns showed comparable trends among males and females, with both sexes experiencing higher incidence in rural areas. Across both urban and rural areas, females recorded a consistently higher malaria incidence than males. Studies suggest that women are generally more likely than men to seek health care services. Age-disaggregated results are consistent with existing literature indicating that children under five were more affected by malaria due to their limited immunity (5). This trend persisted in both urban and rural areas highlighting the need for sustained pediatric-focused malaria prevention and case management interventions.
Spatial analysis revealed that certain rural districts, such as Gulu and Lira, consistently recorded high incidence, while some cities, notably Soroti, emerged as an urban hotspot with incidence surpassing that of its corresponding district.
Recommendations
Malaria incidence declined in both urban and rural areas of Uganda between 2020 and 2024, with rural areas continuing to experience a higher burden, malaria control efforts should prioritize sustaining and strengthening core interventions in high-transmission rural areas. At the same time, targeted strategies should be implemented in identified urban hotspots, such as Soroti City, to address localized drivers of transmission. These strategies may include intensified surveillance, focal vector control, and environmental management targeting urban-specific risk factors such as informal settlements, urban agriculture, and peri-urban mosquito breeding sites. Additionally, interventions should prioritize vulnerable populations, particularly children under five years and females, who were disproportionately affected in both settings.
Study limitations
We used routine DHIS2 surveillance data, which are subject to some limitations including data incompleteness that may affect the validity and interpretation of the findings.
Conclusion
Rural areas consistently experienced a higher malaria incidence compared to urban areas across age and sex groups. However, important heterogeneity exists, with urban hotspots such as Soroti City and high-burden rural districts including Gulu District sustaining elevated transmission. Children under five years and females were more affected in both settings.
Conflict of interest
The authors declared no conflict of interest.
Authors’ contribution
All authors contributed to the write-up and review of the bulletin article. MN drafted the initial version of the article. MN, MM, and CM participated in the data collection and data analysis. RM, BK supervised the data collection and reviewed the draft bulletin article for substantial intellectual content. All authors read and approved the final bulletin article.
Acknowledgements
We appreciate the Ministry of Health Division of Health Information for giving us access the data upon which our results are based.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Health Mo. Malaria Reduction and Elimination Strategic Plan 2021-2025. 2023 [
- G. KA. Socio-Economic Determinants and Malaria Risk: Assessing the Impact of Poverty, Housing Conditions, and Healthcare Accessibility in High-Incidence Regions. 2024.
- Tatem AJ, Gething PW, Smith DL, Hay SI. Urbanization and the global malaria recession. Malaria Journal. 2013;12(1):133.
- Wilson Ml Fau – Krogstad DJ, Krogstad Dj Fau – Arinaitwe E, Arinaitwe E Fau – Arevalo-Herrera M, Arevalo-Herrera M Fau – Chery L, Chery L Fau – Ferreira MU, Ferreira Mu Fau – Ndiaye D, et al. Urban Malaria: Understanding its Epidemiology, Ecology, and Transmission Across Seven Diverse ICEMR Network Sites. 2007(1476-1645 (Electronic)).
- Hay SI, Guerra CA, Tatem AJ, Atkinson PM, Snow RW. Urbanization, malaria transmission and disease burden in Africa. Nature Reviews Microbiology. 2005;3(1):81-90.
- Omumbo JA, Guerra Ca Fau – Hay SI, Hay Si Fau – Snow RW, Snow RW. The influence of urbanisation on measures of Plasmodium falciparum infection prevalence in East Africa. 2005(0001-706X (Print)).
- Merga H, Degefa T, Birhanu Z, Tadele A, Lee MC, Yan G, et al. Urban malaria in sub-Saharan Africa: a scoping review of epidemiologic studies. 2025(1475-2875 (Electronic)).
- Merga H, Degefa T, Birhanu Z, Tadele A, Lee M-C, Yan G, et al. Urban malaria in sub-Saharan Africa: a scoping review of epidemiologic studies. Malaria Journal. 2025;24(1):131.
- Merga H, Degefa T, Birhanu Z, Lee M-C, Yan G, Yewhalaw D. Urban malaria and population mobility in sub-Saharan Africa: systematic review and meta-analysis. Malaria Journal. 2025;24(1):264.
- Martens P, & Hall, L. Malaria on the Move: Human Population Movement and Malaria Transmission. . Emerging Infectious Diseases. 2000.
- Villena OC, Arab A, Lippi CA, Ryan SJ, Johnson LR. Influence of environmental, geographic, socio-demographic, and epidemiological factors on presence of malaria at the community level in two continents. Scientific Reports. 2024;14(1):16734.
- Dear NF, Kadangwe C, Mzilahowa T, Bauleni A, Mathanga DP, Duster C, et al. Household-level and surrounding peri-domestic environmental characteristics associated with malaria vectors Anopheles arabiensis and Anopheles funestus along an urban–rural continuum in Blantyre, Malawi. Malaria Journal. 2018;17(1):229.
Comments are closed.