Epidemiological assessment of COVID-19 cluster among attendees of a church activity, Omoro District, Northern Uganda, September 2020
Authors: Patricia Thiwe1*, Daniel Emong1, Bob Omoda Amodan1, Daniel Kadobera1, Lilian Bulage1, Josephine NamayanjaI, Immaculate Akusekera1, Alex R. Ario1; Affiliation: 1 Uganda Public Health Fellowship Program, Kampala, Uganda; *Corresponding author: Email: pthiwe@musph.ac.ug. Tel: +256782096256
Summary
On 2 October 2020, a cluster of COVID-19 infections was reported in Omoro District in northern Uganda. Despite government directives banning public gatherings, many infected persons had reportedly attended a farewell party at Church X on 5 September. We conducted a retrospective cohort study to determine the source of infections, understand the outbreak magnitude, and identify risk factors for transmission.
We developed a line list by reviewing records and interviewed the index case-patient, church farewell party attendees, and several community members to ascertain possible exposures. We conducted a retrospective cohort study among attendees of the farewell event held on 6 September 2020 at Church X in Omoro District.
Twenty-three confirmed case-patients were identified, including 12 in the Church X cluster. Illness onsets ranged from 23 August to 29 September. The index case, Mr. A was a businessman, Church X choir member, and Church X treasurer with onset on 23 August. Mr. A interacted with the second case Mr. B multiple times before the farewell party Close contact with Mr. A and Mr. B at the farewell party was associated with infection (RR 2.6; 95%CI 1.1-6.7).
Improved adherence to national guidelines and government directives for COVID-19 were recommended.
Background
Since the inception of the SARS-CoV-2 pandemic in late 2019, clusters of infections have been widely reported associated with family gatherings, workplaces, choirs, shopping centres, and night clubs (1, 2). These clusters have often represented super-spreader incidents, in which transmission is facilitated largely by one highly infectious person with many contacts
(3, 4). For reasons that aren’t fully clear, super-spreaders contribute disproportionately to the pandemic by infecting larger number of cases than most infected persons (5). Identification of transmission and risk factors within such clusters is key to providing evidence-based recommendations that can avert such incidents (6).
To reduce the risk of such incidents, Uganda, along with many other countries, implemented recommendations to ban public gatherings including places of worship, weddings, music shows, rallies, bars and other entertainment centers; these directives were given by the president of Uganda on 18 March 2020 (7). In addition, persons with symptoms of COVID-19 were urged to stay home and isolate themselves from others.
On 21 March 2020, Uganda registered its first case of COVID-19 (8)(9). By mid-June 2020, the epidemic had begun to shift in Uganda from sporadic cases to clusters of community cases (10). On 17 August 2020, the District Health Officer of Omoro District, in Northern Uganda, was notified of the first confirmed COVID-19 case in the district. By 2 October 2020, the district had 29 confirmed cases. Of these, several were reportedly linked by residence, social events, or both.
We investigated this cluster of case-patients in Omoro District to understand its source, risk factors, and recommend prevention measures.
We conducted the investigation in Omoro Town Council, Omoro District. Omoro District is located in Northern Uganda and has a population of approximately 200,000 persons. Opit Mission, the site of the church associated with the outbreak (Church X), is a complex housing a church, priests’ residence, convent, health facility, and schools. Wiyagweng community is in the neighborhood, also located within Omoro Town Council, about two kilometers from Opit Mission. The second cluster of infections was in Wiyagweng where the index case-patient resided.
We defined a confirmed case as a positive PCR test for SARS-CoV-2 infection in a resident of Omoro District, 4th September-5th October 2020.
We abstracted information for all confirmed cases from the district COVID-19 case management line list. Information collected included socio-demographic characteristics of the respondents (age, sex, occupation, village of residence); date of sample collection and date of confirmation; whether or not the case-patient had symptoms at sample collection; symptoms developed, if any; underlying medical condition. We visited both Opit Mission and the community to interview case-patients who had been discharged from the treatment units and visited Gulu Regional Referral Hospital to interview case-patients who were still under admission. Seven case-patients, who were admitted in a non-traditional isolation facility (Namboole Stadium) in Kampala, were interviewed over telephone.
We described the case-patients by person, place, and time. We constructed an epidemic curve to describe the distribution of cases in the district over the outbreak period. We also computed attack rates by sex, age, and events attended. Maps were drawn in QGIS version 3.2.1 to show residences of cases.
Twenty-three case-patients were interviewed about exposures before their illnesses using a modified standard COVID-19 case investigation form. The variables captured included basic sociodemographic information including age, sex, and residence at the time of illness, attending church or social events during August and September, including attending mass or choir practice at Church X, attending any burials, and attending the farewell party. We also asked about contact with the primary and secondary case-patients and use of personal protective equipment either at Church X or in the community.
Retrospective cohort study
Based on the hypothesis generation findings, we conducted a retrospective cohort study among attendees of the farewell event held on 6 September 2020 at Church X in Omoro District. A list of all the 69 attendees of the farewell event was obtained from the church authorities and 62 attendees interviewed using a questionnaire.
We used Epi Info 7.2 for entering, cleaning, and analyzing data. We calculated frequencies and proportions to describe the demographic characteristics. We used 2×2 tables to cross tabulate the outcome variable with exposures and stratified the outcome variable with other exposures to obtain risk ratios, and their 95% Confidence Intervals.
Ethical considerations
This was a public health emergency, and the Ministry of Health (MoH) gave the directive to have it epidemiologically investigated. Additionally, the Office of the Associate Director for Science, U.S. Centers for Disease Control and Prevention, determined that this activity was in response to a public health emergency with the primary intent of public health practice (epidemic disease control activity).
We sought verbal consent from the case-patients so as they understand the nature of the study, risks and benefits. During data collection respondents’ data was kept confidential. Information was stored in password protected computers and was not shared with anyone outside the investigation team
Results
Church X and the primary case-patient, Omoro District, September 2020
Church X had approximately 850 members. Its choir had approximately 30 choir members who practiced every Wednesday, Friday, and Saturday. Despite a presidential directive in Uganda banning church gatherings (implemented on 18 March 2020)(7), Church X continued conducting mass (every Sunday) and choir practice every Wednesday, Friday, and Saturday throughout this time.
The primary case, Mr. A, was a 45-year-old businessman and a resident of Wiyagweng village, residing in a parish (village) near the parish where Church X is located. He was a Church X choir member and also the treasurer at the church, and interacted closely with church leadership. He first developed cough and general weakness on 23 August 2020. He
later developed chest pain and shortness of breath. On 9 September, he remained unwell and went to Opit Health Center III where he was advised to proceed to the Gulu Regional
Referral Hospital for a COVID-19 test. On 12 September, he was informed by the district surveillance person that he was positive and was isolated at Gulu Regional Referral Hospital. Due to Mr. A’s underlying Hepatitis B and worsening condition, he was later referred to the larger Mulago National Referral Hospital.
During late August and early September, Mr. A interacted multiple times with the second case, Mr. B. Mr. B was a 64-year-old leader (parish priest) at Church X. Mr. B had symptom onset on 31 August but was not tested for COVID-19 until 10 September.
During much of 2020, Church X had been under renovation. On September 5, the church organized a farewell party for the builders who had come to renovate the church.
The event was attended by approximately 62 persons belonging to the church leadership and/or choir, including Mr. A, and was held in the church garden. At the time of the farewell event, both Mr. A and Mr. B had already developed symptoms. On September 6, a mass was held at the church, attended by both Mr. A and Mr. B.
Clinical and demographic characteristics of case-patients in a church and community COVID19 cluster, Opit Town Council, Omoro District Uganda, September 2020
A total of 23 confirmed COVID-19 case-patients (median age 36 years; range 2-81 years) were identified as being in 2 linked clusters; a community and church cluster.
No deaths were recorded. Most (17; 74%) were male. About half (11; 48%) of the case-patients belonged to Church X, including four (17%) choir members (Tables 1 and 2).
The most common sign and symptoms were cough (13; 57%) and headache (11, 48%) (Table 1).
Table 1: Clinical and demographic characteristics of case-patients in a church and community COVID19 cluster, Opit Town Council, Omoro District Uganda, September 2020
| Characteristic | Frequency
(N=23) |
Percent |
| Age | ||
| ≤17 | 2 | 9 |
| 18-60 | 19 | 83 |
| ≥61 | 2 | 9 |
| Sex | ||
| Female | 6 | 26 |
| Male | 17 | 74 |
| Belong to Church X | ||
| Yes | 12 | 52 |
| No | 11 | 48 |
| Choir member | ||
| Yes | 4 | 17 |
| No | 19 | 83 |
| Church X Event attendance | ||
| Farewell party | ||
| Yes | 15 | 65 |
| No | 8 | 35 |
| Attended September 6 Mass | ||
| Yes | 10 | 43 |
| No | 13 | 57 |
| Signs and symptoms | ||
| Cough | 13 | 57 |
| Headache | 11 | 48 |
| Chest pain | 8 | 35 |
| General weakness | 6 | 26 |
| Running nose | 5 | 22 |
| Chills | 3 | 13 |
| Shortness of breath | 4 | 17 |
| Sore throat | 3 | 13. |
Attack rates among a church and community COVID19 cluster case-patients, Opit Town Council, Omoro District Uganda, September 2020
Attack rates were highest among those who attended the farewell party at 24.2/100 followed by choir members at 13.3/100, Wiyagweng neighbouring community at 6.9, and lowest among the general church members at 1.4/100.
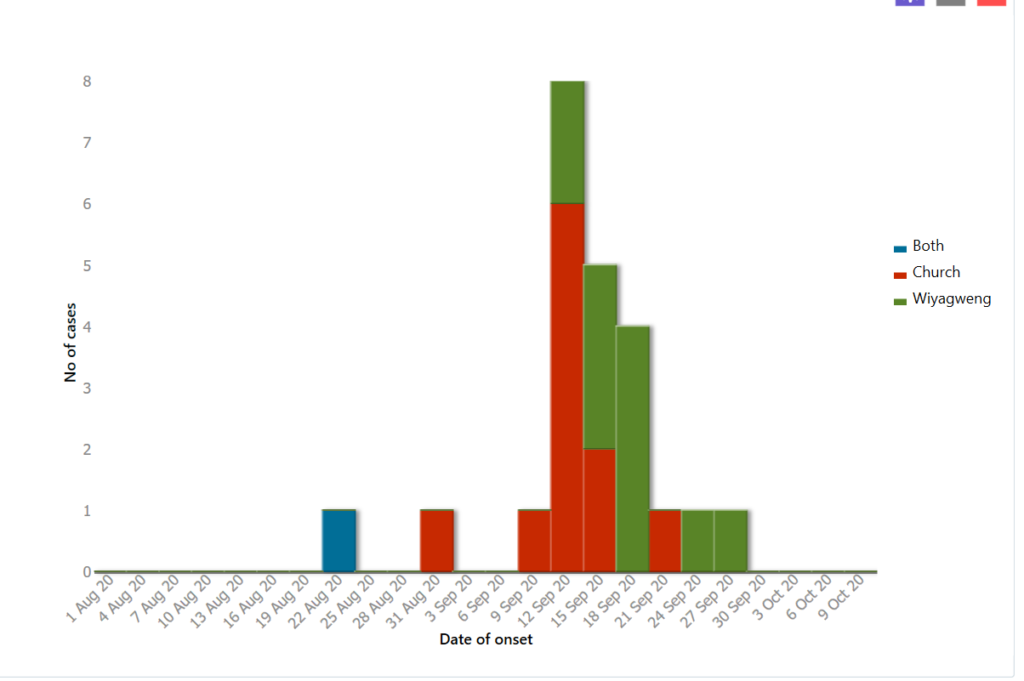
Distribution of case-patients over time in two clusters of COVID 19 cases, Omoro District, September 2020
The epidemiological curve showed point-source outbreak, with most cases having onset 3-21 days after the farewell party (Figure 1).
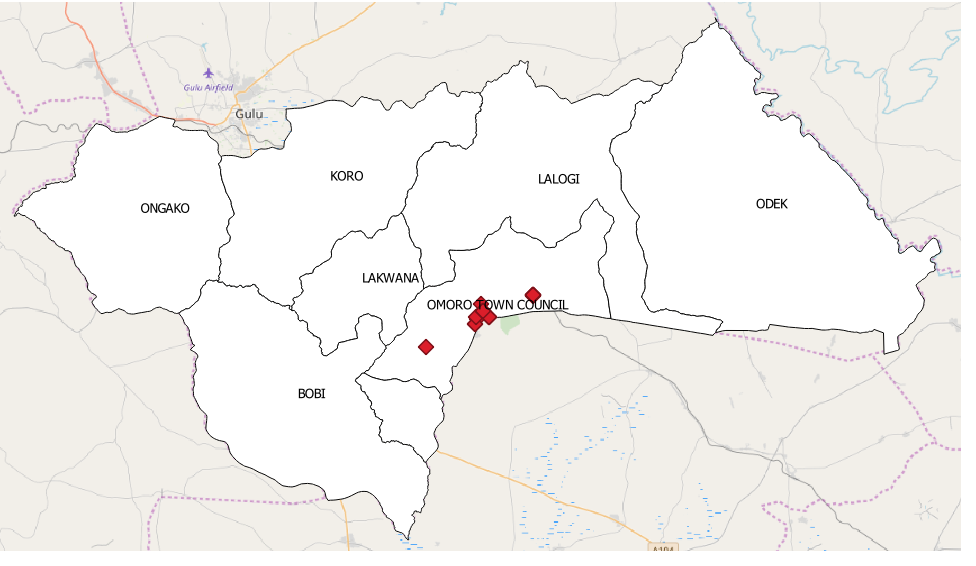
Distribution of case-patients by place of residence
All the case-patients (100%) resided in Omoro Town Council, with 45.5% residing in Lagude parish and 36.4% in Parwech parish (Figure 2). The rest were from nearby Opit North, Thegot, and Lukwi parishes.
Transmission tree of case-patients in a church and community COVID19 cluster, Omoro District, September 2020
There were two clusters that were linked by the primary case-patient (Figure 3), including one associated with the Church (15 cases, including the primary case) and one associated with the community (9 cases, including the primary case). In the Church X cluster, the second case had a direct link with the primary case. Ten of the fourteen (non-primary case) case-patients in the Church X cluster had a possible transmission from either the primary or secondary case. Six of the eight (non-primary case) case-patients in the community cluster were either family or neighbours of the primary case while the other two were infected by persons infected by the primary case.
Hypothesis generation findings
For hypothesis generation, we assessed exposures including participation in choir practice, attendance of church service, attendance of burial and farewell event. Given the frequent attendance of Mr. A and the secondary case at social and church events during their illnesses, we hypothesized that the outbreak could have been linked to contact with Mr. A and/or the secondary case at the farewell event.
Retrospective cohort
We obtained a list of all choir members and those who attended the farewell event for builders on 5 September. We interviewed a total of 62 people including the case-patients in a retrospective cohort study.
We asked about party attendees’ exposure to Mr. A or Mr. B during the party. In total, nine (14.3%) partygoers were exposed to the primary case and 10 (16.1%) were exposed to the second case. Three (4.8%) reported that they were neither exposed to the primary nor the second case.
Table 2: Risk factors for COVID-19 infections among party attendees, Omoro District, September 2020
| Exposure | Exposed | Not Exposed | Risk Ratios | 95%CI | ||
| Ill | Well | Ill | Well | |||
| Exposure to only Mr. A | 9 | 15 | 6 | 32 | 2.4 | 1.1-5.8 |
| Exposure to only Mr. B | 10 | 17 | 5 | 30 | 2.6 | 1.2-6.7 |
| Exposure to both
Mr. A and Mr. B |
9 | 13 | 6 | 34 | 2.7 | 1.1-6.7 |
| Exposure to neither
Mr. A nor Mr. B |
6 | 32 | 9 | 15 | 0.4 | 0.1-0.9 |
Forty percent (9/22) of party attendees who were in close contact with both Mr. A and Mr. B became ill (RR 2.6; CI 1.1-6.7) while 15% (6/40) of attendees who reported no contact with both Mr. A and Mr. B became ill (RR 0.4; CI 01-0.9) (Table 2).
Discussion
This investigation identified 23 confirmed COVID-19 case-patients from two clusters: one among attendees of a farewell event in the church and one in the community. The index case-patient, Mr. A, was a businessman, choir member, and treasurer at Church X, and resident of Wiyagweng village. He attended the farewell event and multiple Church X services in August. The second case-patient, Mr. B, was a leader in Church X, frequently interacted with Mr. A, and attended the farewell party. Mr. A’s late diagnosis provided an opportunity for spread to Mr. B, the community, and other church members. In addition, although Mr. A developed symptoms on 23 August, he continued interacting with church members and the community until he received his test result on 12 September. Diagnosing and treating people early in the course of infection speeds recovery, reduces the likelihood that they develop severe outcomes, prevents spread to others, and reduces demand on the healthcare system(11). Mr. A and Mr. B both attended the farewell event despite their symptoms and this provided an opportunity to spread.
Despite the presidential directive banning all social gatherings, Church X continued to have choir practice, church mass, and party. The emergence of SARS-CoV-2 in China in late 2019
refocused global attention on national, regional, and pandemic spread through mass gathering events. Since early March 2020, there was a step increase in cancellation of international and national religious, sporting, musical, and other mass gathering events as countries worldwide took measures to contain the spread of SARS-CoV-2 (12). While the outbreak is widespread, such measures should be continued to avert large COVID-19 clusters.
Clusters of COVID-19 and high transmission have been reported elsewhere in health facilities, families, church events, and other gatherings (6, 12-15).With the on and off reopening of in-persons church services and other events, this serves as a signal to the risk of high transmission. This outbreak of COVID-19 underscores the importance of physical distancing, including maintaining at least 6 feet between persons, avoiding group gatherings and crowded places, and wearing cloth face coverings in public settings where other social distancing measures are difficult to maintain during this pandemic.
Limitations
Our findings should be interpreted with the following limitation. Despite an intensive epidemiologic investigation, we were not able to reach six case-patients who were still at isolation centers and did not have phone contacts. We could have possibly missed other exposures related to this cluster. However, the number not reached out of the total case-count for the cluster was too small to have an impact on the study’s overall results and the interpretation.
Conclusion
The social gathering at church X provided an opportunity for a COVID-19 super-spreading event. We recommended adherence to SOPs for COVID by church and community members and halt of church activities by church X.
Acknowledgement
We acknowledge Omoro District Local Government for supporting and permitting us to undertake this investigation. We thank the respondents for agreeing to take part in the investigation, the Ministry of Health, and the Uganda Public Health Fellowship Program for jointly supporting this investigation
References
- Lin G-t, Zhang Y-h, Xiao M-f, Wei Y, Chen J-n, Lin D-j, et al. Epidemiological investigation of a COVID-19 family cluster outbreak transmitted by a 3-month-old infant. Health Information Science and Systems. 2021;9(1):6.
- Qiu YY, Wang SQ, Wang XL, Lu WX, Qiao D, Li JB, et al. [Epidemiological analysis on a family cluster of COVID-19]. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi. 2020;41(4):494-7.
- Majra D, Benson J, Pitts J, Stebbing J. SARS-CoV-2 (COVID-19) superspreader events. The Journal of infection. 2021;82(1):36-40.
- Cave E. COVID-19 Super-spreaders: Definitional Quandaries and Implications. Asian bioethics review. 2020:1-8.
- Kumar S, Jha S, Rai SK. Significance of super spreader events in COVID-19. Indian journal of public health. 2020;64(Supplement):S139-s41.
- Yong SEF, Anderson DE, Wei WE, Pang J, Chia WN, Tan CW, et al. Connecting clusters of COVID-19: an epidemiological and serological investigation. The Lancet Infectious diseases. 2020;20(7):809-15.
- African TE. Uganda'”s Museveni orders closure of schools, bans public gatherings. The East African. 2020.
- Health Mo. COVID-19 situation Report #34. 2020.
- Ministry of Health U. COVID-19 situation Report #230. 2020.
- Uganda U. COVID-19 situation report No.3. 202.
- To KK, Tsang OT, Yip CC, Chan KH, Wu TC, Chan JM, et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2020;71(15):841-3.
- McCloskey B, Zumla A, Ippolito G, Blumberg L, Arbon P, Cicero A, et al. Mass gathering events and reducing further global spread of COVID-19: a political and public health dilemma. Lancet (London, England). 2020;395(10230):1096-9.
- Pung R, Chiew CJ, Young BE, Chin S, Chen MI, Clapham HE, et al. Investigation of three clusters of COVID-19 in Singapore: implications for surveillance and response measures. Lancet (London, England). 2020;395(10229):1039-46.
- Yang HY, Xu J, Li Y, Liang X, Jin YF, Chen SY, et al. [The preliminary analysis on the characteristics of the cluster for the COVID-19]. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi. 2020;41(5):623-8.
- James A, Eagle L, Phillips C, Hedges DS, Bodenhamer C, Brown R, et al. High COVID-19 Attack Rate Among Attendees at Events at a Church – Arkansas, March 2020. MMWR Morbidity and mortality weekly report. 2020;69(20):632-5.
Patricia Thiwe1*, Daniel Emong1, Bob Omoda Amodan1, Daniel Kadobera1, Lilian Bulage1, Josephine NamayanjaI, Immaculate Akusekera1, Alex R. Ario1. Epidemiological assessment of COVID-19 cluster among attendees of a church activity, Omoro District, Northern Uganda, September 2020. Kampala. Uganda National Institute of Public Health. 2021 September 30th. Available from:https://uniph.go.ug/epidemiological-assessment-of-covid-19-cluster-among-attendees-of-a-church-activity-omoro-district-northern-uganda-september-2020.
Comments are closed.