
Mumps Outbreak in a Children’s Home, Wakiso District, August 2017
Authors: Denis Nixon Opio1, Kizito Suzan1, Eyu Patricia1 Okethwangu Den- is1, Claire Biribawa1, Benon Kwesiga1; Affiliation: 1Uganda Public Health Fellowship Program
Summary
On the 28 July 2017, Public Health Emergency Operations Centre, Uganda received an alert of 12 suspected cases of mumps among children in a Children’s Home with a school in Wakiso District. We investigated to verify the existence of the outbreak, determine the scope, identify exposure factors, and recommend control interventions. We defined a suspected case as acute onset of swollen/ painful salivary glands in a person living in Wakiso District from 1 June-15 September 2017. We identified cases through medical record review at the school clinic; controls were asymptomatic children at the school. We administered a questionnaire to the children, teachers, and parents about children’s exposures and hygienic behaviors. We identified 25 case-persons. Overall attack rate (AR) among children <10 years was 21%. The AR was highest in nursery class (64%) and primary 1 (46%) and lowest in preparatory (6.3%) and primary 2 class (4.6%). Both nursery and primary 1 classes had 5-6 children per table, while preparatory and primary 2 classes had 2-3 children per table. Being in primary 1 [(OR=9.6(95% CI; 2.7-34.2)] and close interaction with a sick child [OR=15.5 (95% CI; 3.4-70.1)] were associated with mumps infection at the children’s home. This was a mumps outbreak that affected children in lower primary classes at the children’s home. Crowding in the classroom and late diagnosis may have contributed to the outbreak. We recommended vaccination of all asymptomatic children<10 years, isolation of symptomatic children for 5 days after symptom onset, and reducing the number of pupils per table in classes where possible. The Uganda Ministry of Health should consider including MMR vaccine in routine vaccination schedules.
Background
Mumps is an acute viral illness transmitted by respiratory drop- lets and saliva[1]. The incubation period ranges from 12-25 days but parotitis typically develops 16-18 days[2]. In the absence of vaccination, mumps is epidemic with peaks after every 2-5 years [3]. Vaccination of Mumps in Uganda is not available in Public Health Facilities. In recent years, increasing outbreaks of Mumps infection have been reported in Sub-Saharan Africa, the most affected countries in 2016 were Kenya, Ghana and Rwanda[4]. Several upsurges of mumps have occurred in Uganda but were neither reported nor investigated. On the 28 July 2017, Ministry of Health was alerted of 12 suspected cases of Mumps from a children’s home in Wakiso District. We investigated the epidemiologic characteristics, risk factors for the transmission and developed recommendations to control future outbreaks.
Methods
We defined a suspected case as acute onset of swollen/painful salivary glands in a person living in Wakiso District from 1st June 2017 onward and a confirmed case as any suspected case with positive IgM mumps result. We actively searched for cases in the school, children homes and reviewed health facility records. We collected blood samples for laboratory confirmation of the out- break and inspected classrooms and children homes for sitting arrangement in class, sleeping arrangement at home and person- al hygiene facilities. We carried out descriptive analysis and an unmatched case control study in which we randomly selected 3 asymptomatic school controls for each case identified using stratified sampling giving a total of 25 cases and 87controls.
Results
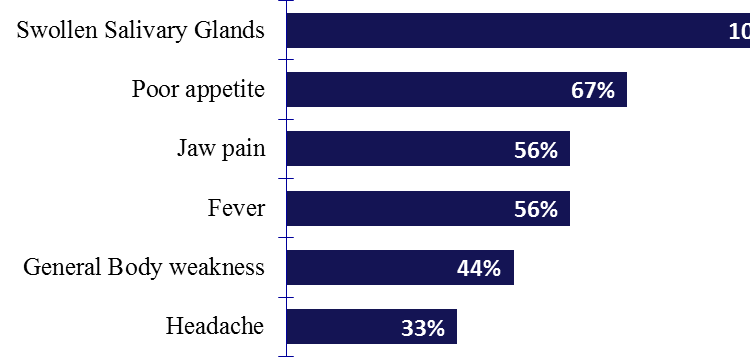
Descriptive Epidemiology We identified 25 suspected cases persons. Of the cases, 24% (6/25) were confirmed with positive IgM for mumps. No deaths occurred. The clinical presentations were consistent with mumps with all cases reporting parotitis
Figure 1: Clinical presentation of cases
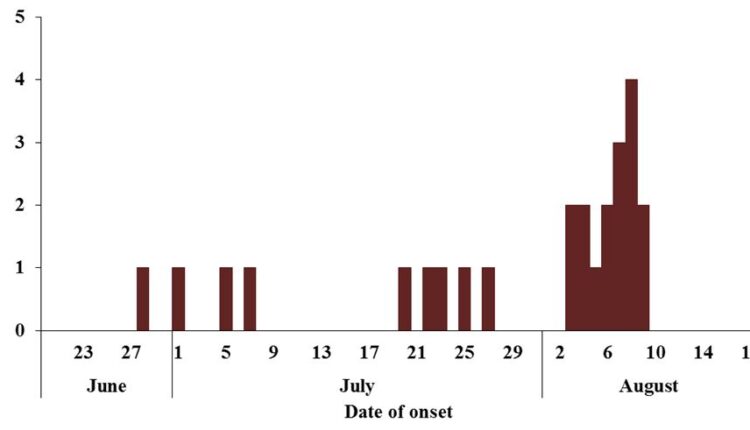
Time Characteristics
The first case was identified on 28 June 2017 and the epidemic peaked in August 2017
Figure 2: Distribution of cases by time of onset in children’s home
Place Characteristics
Overall, the attack rate for mumps at the children’s home was 21%. The attack rate was highest in nursery class (64%) and lowest in primary 2 class (4.6%).
Table1: Attack rates by class
| Class | Cases | Population | AR (%) |
| Nursery | 9 | 14 | 64 |
| Preparatory | 1 | 16 | 6.3 |
| Primary1 | 12 | 26 | 46 |
| Primary2 | 3 | 65 | 4.6 |
| Total | 25 | 121 | 21 |
Tables 2; Number of pupils per table in class
| Class | #Children/table |
| Nursery | 5 |
| Preparatory | 2 |
| Primary1 | 6 |
| Primary2 | 3 |
| Class | #Children/table |
| Nursery | 5 |
| Preparatory | 2 |
| Primary1 | 6 |
| Primary2 | 3 |
Primary 1 had 6 pupils sharing a table while nursery had 5 pupils per table
Persons Characteristics
Table 3: Attack rates by age in children’s home Y, Wakiso District Uganda: Jun-Aug 2017
The median age was 6 years (Range 3-10). The age group ≤4 years was the most affected with AR of 62%.
| Age (Years) | Cases | Population | AR (%) |
| ≤4 | 8 | 13 | 62 |
| 5-7 | 6 | 45 | 13 |
| 8-10 | 11 | 59 | 19 |
| >10 | 0 | 4 | 0 |
| Total | 25 | 121 | 21 |
Table 4: Attack rates by sex in children’s home Y, Wakiso District Uganda: Jun-Aug 2017
The girls had a higher AR (26%) compared to the boys(16%).
| Sex | Cases | Population | AR (%) |
| Boys | 10 | 64 | 16 |
| Girls | 15 | 57 | 26 |
| Total | 25 | 121 | 21 |
Case management
Patients with fever were managed on Paracetamol and Vita- min A while patients with extensive swelling were given Prednisolone.
Vaccine effectiveness and coverage
Vaccine Effectiveness was calculated as thus:
VE = (1 – ORMH) x 100
We found that the vaccine effectiveness was 100%.
Cumulatively, 24% (73/310) of all children in this school had been vaccinated against mumps between 2013 and 2017. By March , vaccination coverage was 13% among children from Nursery to P2 classes. MMR vaccine in this school is only given in single dose to children going for trips abroad.
Table 5: Vaccination coverage by class in children’s home Y, June to August 2017
Case Control Study
| Vaccinated | ||||
| Class | Yes | No | Total | Coverage (%) |
| P2 | 14 | 38 | 52 | 27 |
| P1 | 0 | 27 | 27 | 0.0 |
| Preparatory | 0 | 2 | 2 | 0.0 |
| Nursery | 1 | 30 | 31 | 3.0 |
| Total | 15 | 97 | 112 | 13 |
We found that the age groups 6-7 and ≤5 years old were significantly associated with development of mumps. Being in primary 1 and nursery classes, and having close contact with a child sick with mumps were also significantly associated with the disease. Other kinds of contact, such as sharing of bed and room with other children, touching eyes, nose, and mouth, sucking fingers and licking pencils and rubbers from the case- patient, played no role during this outbreak
Table 6: Risk factors for mumps outbreak in children’s home Y, from June to August 2017
| Characteristics | Case-patients
% (n=25) |
Controls
% (n=87) |
OR(95% CI) |
| Age | |||
| ≥8 | 53 | 53 | 1 |
| 6-7 | 26 | 26 | 4.4(1.4-14) |
| ≤5 | 21 | 21 | 4.6(1.4-16) |
| Sex | |||
| Male | 47 | 14 | 1 |
| Female | 54 | 56 | 1.1(0.4-2.7) |
| School class | |||
| Primary 2 | 16 | 55 | 1 |
| Primary 1 | 48 | 17 | 9.6(2.7-34 |
| Preparatory | 8 | 0 | 1 |
| Nursery | 28 | 28 | 3.5(0.9-13) |
| Vaccination status | |||
| Yes | 0 | 17 | – |
| No | 100 | 83 | 1 |
| Contact with sick child | |||
| Yes | 92 | 43 | 16(3.4-70) |
| No | 7.7 | 57 | 1 |
Environmental Risk factors for Mumps
We found that children in nursery and primary 1 classes are , there were 2 or 3 children on a table of a similar size as those in the allocated a table for every 5 or 6 children. In preparatory and primary 2 classes other classes. We found that there were washing facilities available for the children to use after using the toilet. These hand-washing facilities are situated just outside the classrooms.
Discussion
Our study shows that talking, sneezing and playing with the index case-patient at close range at Children’s home, Y led to this outbreak. This outbreak was further facilitated by transmission inside the classrooms due to close sitting arrangement of 5-6 pupils per table in Nursery and primary1 class. This was comparable with a study done in Kansas, which showed that relatively closed architectural design of school A and the intersection of many short corridors encouraged a complicated flow pattern of students between classes bringing many students in contact with one an other and may have increased the level of respiratory contact among students(1). Conversely, other kinds of contact, such as sharing of bed and room with other children, touching eyes, nose, and mouth, sucking fingers, and licking pencils and rubbers from the case-patient played no role during this outbreak. Other studies also found that crowded, institutionalized setting such as a school and children’s home play a big role in mumps transmission [5]. The most affected class was P1 class, which is bordered by P2.
This proximity could have facilitated transmission through con- tact with children in P2. However, transmission in P2 was the lowest because of high vaccination coverage of MMR. Hygiene practices in the classrooms and homes were good. All classrooms and homes had hand washing facilities and soap. The classes were well ventilated and clean. Hand washing practices were not significantly associated with the outbreak. This could have been due to the fact both cases and controls had similar access to hand washing facilities. Children’s home Y, and Wakiso District was not yet able to contain the current infection and later on prevent new infections from happening. This was observed in Outpatient Clinic that was the treatment centre for Mumps. This clinic had remained with only 2 doses of MMR vaccine which was not enough to vaccinate the whole school children
Conclusion
The Mumps outbreak has affected children in lower primary classes. Results of the case-control study showed that the virus spread by droplet transmission when sick pupils were talking with their fellow pupils. Additionally, the affected classrooms had between 5-6 children sitting on one table in class. Children’s home Y, does not have enough MMR vaccines to manage the outbreak. The findings of our investigation highlight the importance of preventing droplet transmission during an outbreak and early recognition of mumps clinical characteristics.
Recommendation
We recommended vaccination of all asymptomatic children <10 years in WCH, isolation of symptomatic children for 5 days after symptom onset, and reducing the number of pupils per table in classes where possible. The Uganda Ministry of Health should consider including MMR vaccine in routine vaccination schedules.
References
- Hersh BS, Fine PE, Kent WK, Cochi SL, Kahn LH, Zell ER, et al. Mumps outbreak in a highly vaccinated population. J Pediatr. 1991;119(2):187–93.
- Updated recommendations for isolation of persons with MMWR Morb Mortal Wkly Rep, 2008. 57(40): p. 1103-5.
- CDC, https://cdc.gov/vaccines/parents/diseases/ child/mumps-basics-color.pdf. 2017.
- Heymann, D.L., Control of Communicable Diseases American Public health association, 2015. 20th Edition.
- http://apps.who.int/immunization_monitoring/
globalsummary/timeseries/tsincidencemumps.html. 6.Turabelidze, G., et al., Personal hygiene and methicillin- resistant Staphylococcus aureus infection. Emerging infectious diseases, 2006. 12(3): p. 422.
Comments are closed.