
Malaria Outbreak facilitated by Roadside Pools in Zombo District, Uganda, January – June 2019
Authors: Irene B. Kyamwine1*, Daniel Eurien1, Benon Kwesiga1, Daniel Kadobera1, Lilian Bulage1, Alex R. Ario1 Affiliations: 1 Uganda Public Health Fellowship Program, Ministry of Health, Kampala, Uganda * Corresponding Author: Irene B Kyamwine, E-mail: ikyamwine@musph.ac.ug; Tel: +256781711102
Summary
As part of national strategy, Uganda in 2014 began implementing multifaceted interventions to facilitate malaria elimination. However, the country still routinely has outbreaks. Zombo District had an up- surge of malaria cases starting January 2019. We investigated to determine the outbreak scope, identify exposures for transmission, and recommend evidence-based interventions. We defined a case as positive malaria rapid diagnostic test (mRDT) or microscopy from 1 January-30 June 2019 in a resident of or visitor to Zombo District.
We reviewed medical records in all district health facilities to identify cases. In a case-control study, we compared exposures between case- patients and asymptomatic village- and age-matched controls. We conducted entomological and environmental assessments in the same sub-county. We identified 63,451 case-patients (AR=24%) and 100 deaths. Children <5 years were most affected (AR=34%). Females (AR=28%) were more affected than males (AR=20%). Sub-county AR ranged from 7.3% (Nyapea) to 34% (Kango). All 14 mosquitoes captured in homes were engorged with blood. All seven breeding sites observed had Anopheles larvae. Among 149 case-patients and 149 controls, 83 (50%) case-patients and 63 (43%) controls lived <500 meters from roadside pools (OR: 2.7, 95% CI: 1.4-5.2); 17 (11%) case-patients and seven (4.7%) controls lived <500 meters from a swamp (OR: 6.0, 95% CI: 1.3–27). Fifty-one (76%) controls and 56 (38%) case-patients wore protective clothes in evenings (OR: 0.49, 95% CI: 0.27-0.87), and 90 (60%) controls and 80 (54%) case-patients slept under a mosquito net in the 2 weeks before symptom onset (OR: 0.74, 95% CI: 0.46–1.2). We described an outbreak attributed to poor use of protective measures and standing water with mosquito larvae. We recommended increased awareness on malaria prevention measures, creation of proper drainage offshoots, prompt treatment for the sick, and use of bed nets.
Introduction
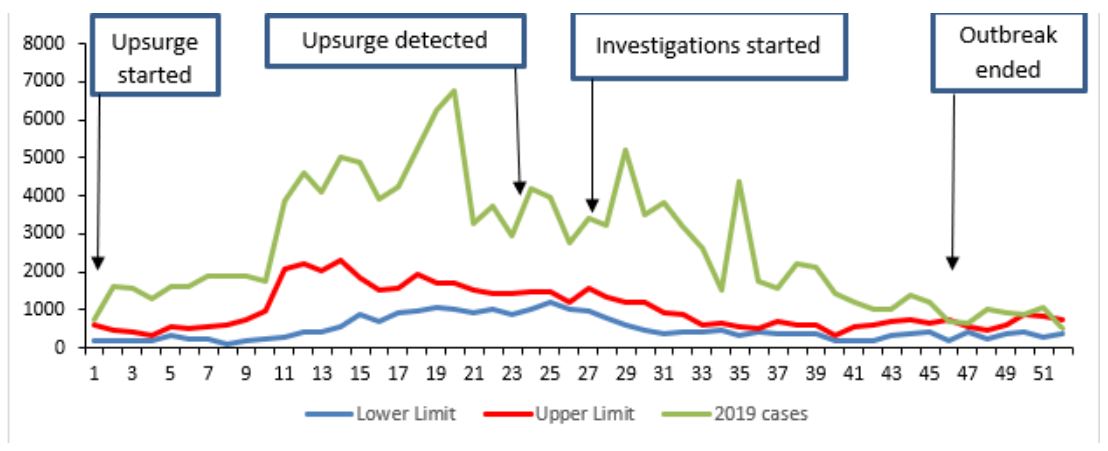
Globally malaria remains a major cause of ill-health and deaths with approximately 219 million cases occurring in 2017 compared to 239 million cases in 2010 (1). Approximately 75% of cases and deaths were from Sub-Saharan Africa; where approximately 60% of the population is at risk (2). In Uganda, malaria remains a leading cause of morbidity and mortality with over 90% of the population living at risk of developing the disease (3,4). Uganda is ranked fourth among the highest malaria-burden countries in the world, with some of the highest transmission rates in the world (5). Malaria accounts for up to 50% of outpatient visits, 15–20% of admissions and up to 20% of hospital deaths (4). According to the Uganda Malaria Indicator Sur- vey 2009, malaria parasitemia was high in most regions of the country, with hyper-endemicity (prevalence of 50–75%) demonstrated in three regions, meso-endemicity (prevalence 10–50%) in six, and hypo -endemicity (prevalence < 10%) in one region (6). The subsequent Malaria Indicator Survey conducted in 2015, showed a reduction in parasitemia risk in all regions of the country (4). This decline in parasitemia has been attributed to interventions, including the increased coverage of insecticide-treated mosquito nets (ITNs), integrated community case management, and indoor residual spraying (IRS) (6,7). However, Zombo District did not participate in the 2017 IRS conducted by Ministry of Health (1) and is currently not implementing integrated community case management (ICCM) which is another control measure for malaria among children less than five years. On 3rd June 2019, through routine analysis of malaria surveillance data, Zombo District showed an upsurge of malaria cases which exceeded the action threshold from Epi week 1 of 2019 (Figure 1). We investigated to determine the scope of the outbreak, identify the exposures for increased transmission, and provide evidence-based control and prevention measures.
We defined a malaria case as a positive malaria test result by mRDT or microscopy from 1 January to 30 June, 2019 in a resident or visitor of Zombo District. We reviewed health facility records at all the health facilities in Zombo district to identify cases. We performed descriptive analysis by person, place, and time. We randomly selected a sub-county that had an attack rate greater than 20% (Abanga sub-county). We conducted environmental and entomological assessment in Abanga sub-county and interviewed 20 confirmed case-patients that we sampled conveniently for hypothesis generation. We conducted pyrethrum spray catches (PSC) in the five parishes of the same sub county. We conducted a matched case-control study in all the parishes. We recruited 149 cases and 149 controls.
Results
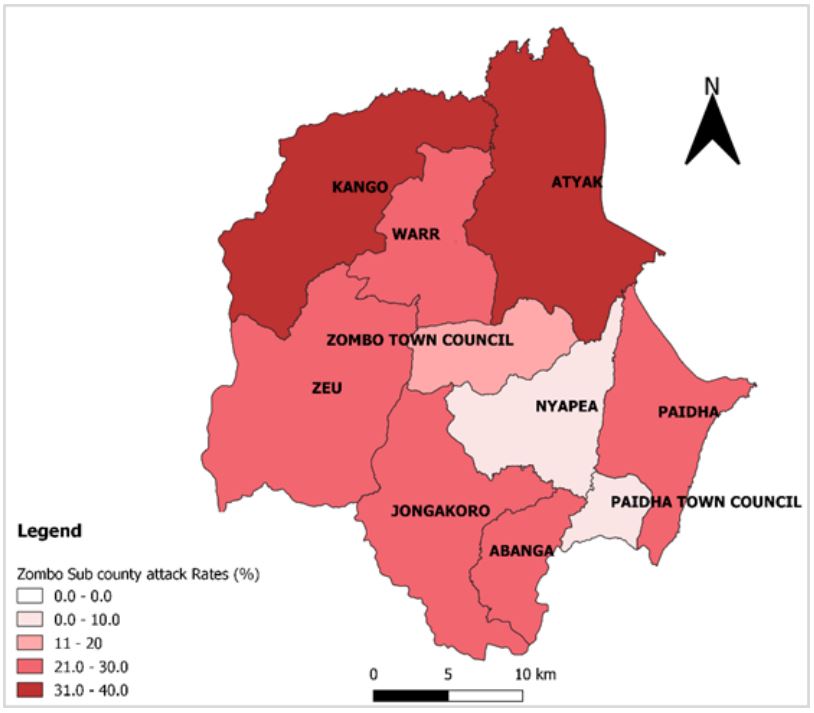
We identified 63,451 malaria cases-patients during 1 January to June, 2019 and 100 malaria related deaths (CFR= 16 /10,000 population). The overall attack rate was 24%, and median age of 10 years (range: 0.038 to 98 years). Age-group < 5 years was most affected (AR: 34 %) followed by 5–18 year (AR:29) and >18 years (AR: 14%). Females were more affected (AR:28%) compared to males (AR: 20 %). The outbreak affected all the 13 sub units of Zombo District with Kango sub-county being most affected (AR: 34%) followed by Atyak (AR: 31%) (Figure 2)
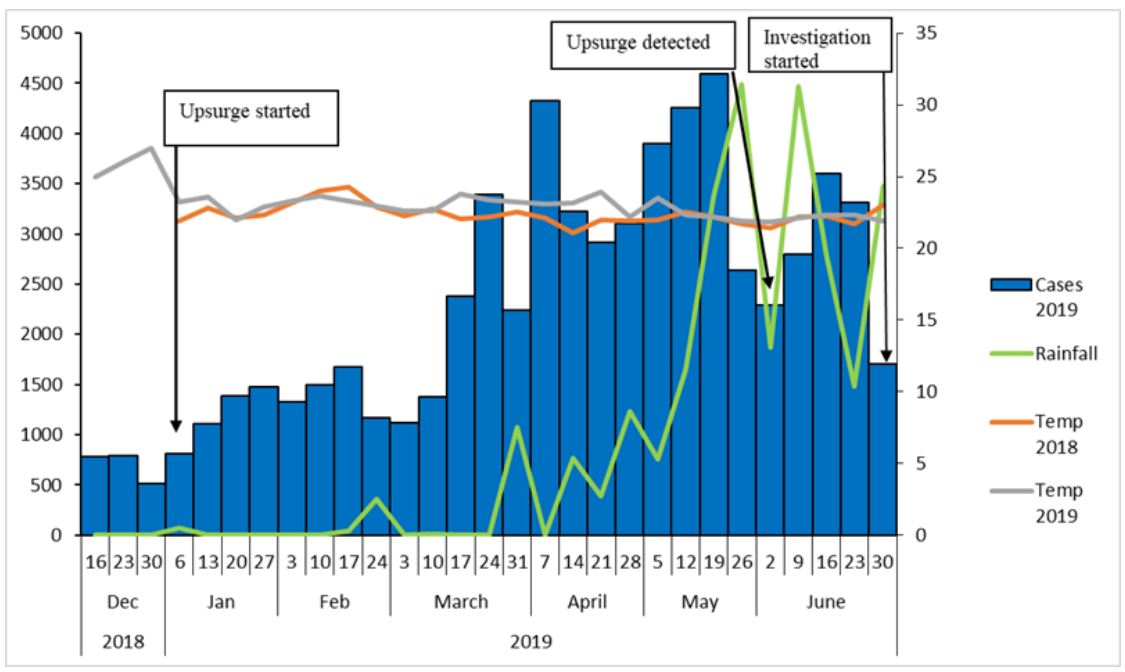
There was a gradual increase of cases from December 2018 to January 2019 peaking in April and May 2019. A gradual decline is noted in June. However, the upsurge was detected in June 2019, seven months after the onset. There was low consistent rainfall peaking in May and June 2019. With every peak of rainfall there was an in- crease in the number of cases at least three weeks after. The epi-curve is indicative of a continuous transmission pattern that has been sustained from January to June 2019 (Figure 3).
Hypothesis generation findings
Of the 20 case-patients interviewed, 85% (17/20) lived in houses with a mud wall and grass roof, 75% (15/20) reported having dam- aged mosquito nets, 70% (14/20) reported entering bed after 9:00pm , 70% (14/20) had history of a sick person in the neighbor- hood before onset of symptoms, 65% (13/20) had water logging present near their household, 65% (13/20) reported closing doors and windows after 7pm, 60% (12/20) reported wearing protective clothes in the evening, 60% (12/20) reported using mosquito net, 55% ( 11/20) reported history of sick person in the household, and 50% (10/20) reported gathering around a fire place in the evening. Based on the findings, we hypothesized that: Entering bed after 9pm, living in an area with water logging, having a sick person in the household or neighborhood and wearing protective clothing in the evening were associated with the outbreak.
Case control study results
On average, every household had 2 mosquito nets (max: 7, Min: 0 and mode: 1). There was a significant difference in malaria infection with increase in household size. Overall mosquito net owner- ship was 78% (233/298). Twenty one percent (32/149) of case- patients and 13% (20/149) of control persons reported sleeping under a damaged mosquito net (OR: 1.7, 95% CI: 0.94–3.1). 54% (80/149) of case-patients and 60% (90/149) of control persons slept under a mosquito net 2 weeks before symptom onset (OR: 0.74, 95% CI: 0.46–1.2) . Fifty six percent (83/147) of case-patients and 43% (63/147) control persons lived within 500 meters of a road side pool 2 weeks before symptom onset (OR: 2.7, 95% CI 1.4 -5.2) ; 11% (17/149) of case-patients and 4.7% (7/149) control per- sons lived within 500 meters of a swamp two weeks before symptom onset (OR: 6, 95% CI: 1.3–27). 59% (88/148) of case-patients and 16% (24/148) of control persons had a household member with malaria 2 weeks before symptom onset (OR: 11, 95% CI: 5.07– 27); and 59% (88/148) of case-patients and 16% (24/148) of control persons had a neighbor with malaria prior to onset of symptoms (OR: 11, 95% CI: 5.07–27). 38% (56/149) of case-patients and 76% (51/149) of control persons wore protective clothes in the evening, (OR: 0.49, 95% CI: 0.27-0.87).
Environmental and entomological assessment
We observed road side pools of stagnant water, pits from brick laying and puddles in Abanga Sub-County. Seven breeding sites were sampled of which 85% (6/7) were man made and 15% (1/7) were from natural sites such as gullies. Of the six man made breeding sites, 67% (4/6) were roadside pools, 17% (1/6) from brick laying, and 17% (1/6) murram excavation pits. All the sampled breeding sites were found to have anopheles larvae at different stages. The highest number of larvae (250/50 mls of water)

Of the 27 households reached for the PSC, 63% (17/27) had a mosquito net and only 26% (7/27) had a ceiling. Fourteen adult anopheles mosquitoes were caught in the 27 households. Of which 79% (11/14) were Anopheles gambiae and 21% (3/14) Anopheles funestes species. The indoor resting density was 2 mosquitoes /household / night. All 14 (100%) mosquitoes were blood fed. Early morning collections showed higher numbers that decreased with increasing hours of the day, indicating that the mosquitoes in the locality are endophagic (bite predominantly indoors) and rest outdoors (Exophilic) based on few mosquitoes caught in the later hours of the day.
Discussion
In this study we identified 63,451 malaria cases and CFR: 16/10,000 population. The upsurge was noted in epi week 1 of 2019 peaking in March and April 2019. Children below 5 years and females were most affected. Consistent low levels of rainfall that started in epi week 49 of 2018 and continued throughout the outbreak period. This outbreak was associated with living within 500 meters to a road side pool or swamp and wearing protective clothing in the evening was protective from malaria infection. Entomological assessment showed multiple water breeding sites of Anopheles mosquitoes.
This investigation revealed that those who had mosquito breeding site around their houses were more likely to be diseased by malaria than those who didn’t have mosquito breeding site. This is consistent with other studies in Ethiopia (8,9). Human activity like brick laying, swamp farming, and road construction led to creation of temporary pools of water, that had poor drainage potentiating breeding of the malaria vectors. These breeding sites were sustained by low levels of continuous rainfall and consistently high temperatures throughout this period which are factors that facilitate increased breeding of mosquitoes.
This is consistent with an environmental study in Cameroon that demonstrated increased density of malaria parasite higher in the rainy season (21). These breeding sites could not dry in short periods by themselves. The breeding sites were found to have anopheles larvae at different stages signifying that mosquitoes were avail- able at all times not causing interruption in transmission.
Studies have shown that larval densities fluctuate in malaria endemic populations during seasonal changes in climatology.
During the rainfall periods, temporary pools of water are formed in areas with swamps, ditches, and pools along the road side among others. These sites hold fresh stagnant water that provides active breeding sites for malaria vectors (15). PSC identified Anopheles gambiae and Anopheles funestes species that are mainly endophagic and exophilic which are the species responsible for malaria trans- mission in most of Africa (21). To control the malaria outbreak, mosquito breeding sites therefore need to be cleared by involvement of the local community, draining of temporary pools, environ- mental modification, and use of larvicides to interrupt the breeding cycle.
Wearing protective clothes was protective in this outbreak. This is consistent with a study in Ethiopia were wearing of protective clothing was shown to reduce the odds of malaria infection(15). Wearing of protective clothes helps reduce the exposed body extremities that could have reduced the possibility of mosquito bite (15). Similarly, use of mosquito nets was shown to be protective but most of them were old and some torn, or shared by many people in the home, used for different purposes such as protecting domestic birds, curtains; which could explain why the association was not significant. Other factors such as inconsistence in use and going to bed after 9 pm could explain the insignificant association. This is consistent with a study conducted in Cameroon in which the prevalence of malaria was high even among those who used mosquito nets and another in Ethiopia in which an outbreak resulted from poor vector control measures (17,21).
In this study, children had higher odds of malaria infection compared to older age-groups. Similar findings were found in other studies conducted in Uganda and Cameroon that demonstrated higher odds of malaria infection among children (12, 21). Also, a study conducted in Tanzania on malaria prevalence and socio- demographic factors demonstrated that children and female were more susceptible to malaria (20). This could be explained by protective immunity among adults as a result of previous exposure to malaria compared to malaria naïve children.
We also found that, females were more affected than males. These findings are similar to findings in a study in Zimbabwe (19). This difference could be because adult women do more night activities that expose them to mosquito breeding sites, such as cooking in kitchens detached from their houses, splitting fire wood, fetching water. This could also be explained by the women’s better health seeking behaviours compared to the men (23).
Vector control measures such as indoor residual spraying, replacement of LLINs, draining or chemical spraying of breeding sites for removing the larvae; have not been done in Zombo District. This could explain the increased levels of malaria that surpass the epidemic threshold.
The district does not consistently draw malaria channels to help in the detection of outbreaks early because of this, there was a delay in the detection and response to this outbreak which could explain the high malaria cases and CFR. This is consistent with studies by Adhisu et al 2014, and Workineh et al 2019, which demonstrated that delayed detection and interventions were the propagating factors for the outbreaks.
Conclusions and recommendations
The outbreak affected the entire district with children, females, and Kango sub-county being most affected. There was continuous trans- mission of malaria propagated by road side pools of standing water and swamps and inconsistent use of bed nets.
Wearing protective clothes was protective. We recommended that the district in collaboration with NMCP create awareness on malaria prevention measures like proper mosquito net usage, and a proper road drainage system put in place to avoid water logging. NMCP should have malaria channels drawn at least twice a month for each district to ensure that outbreaks are detected early and responded to promptly.
Reference
- World Health Organization. WORLD MALARIA REPORT 2018. 2018.
- WHO | World Malaria Report 2016 [Internet]. WHO [cited 2019 Jul 30]. Available from: http://www.who.int/malaria/ publications/world-malaria-report-2016/report/en/
- Wanzira: The challenge of using intermittent preventive… – Google Scholar [Internet]. [cited 2019 Jul 30].
- Uganda. Ministry of Health: Monitoring and Evaluation… – Google Scholar [Internet]. [cited 2019 Jul 30].
- Ssempiira: The contribution of malaria control interventi… – Google Scholar [Internet]. [cited 2019 Jul 30].
- Uganda Bureau of Statistics (UBOS) and ICF Macro. Uganda malaria indicator survey 2009. Calverton, Maryland, USA: UBOS and ICF Macro; 2010. – Google Search [Internet]. [cited 2019 Jul 30]
Comments are closed.