
Malaria Outbreak facilitated by agricultural activities, residing near water logged areas and participating in late night campaign activities: Nabitende Subcounty, Iganga District, December 2020-February 2021
Authors: Immaculate Atuhaire*, Esther Kisakye1, Sherry Ahirirwe1, Hildah Nansikombi1, Shaban Senyange1, Stella Martha1, Rose Nampeera1, Patience Mwine1, Rose Nampeera1, Sarah Elayete1, Alice Asio1, Veronica Masanja1, Allan Komakech1, Edirisa Nsubuga1, Andrew Kwiringira1, Kwesiga Benon1, Daniel Kadobera1, Alex R. Ario1, and Julie Harris2 Affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda,2US Centers for Disease Control and Prevention, Kampala, Uganda Corresponding author*: Email: atuhaire@musph.ac.ug, Tel: +25677 816 066
Summary
Background: Despite implementation of prevention measures, malaria remains the leading cause of illness and death in Uganda. In Feb 2021, Ministry of Health–Uganda identified an upsurge in malaria cases in Iganga District, Eastern Uganda, and thus necessitated epidemic response and control. We investigated this outbreak to establish the scope and magnitude of the outbreak, possible exposures and to make public health recommendations. Methods: We defined a malaria case as a positive malaria test result using mRDT or microscopy in a resident of Iganga District from 1 May 2020 to 28 Feb 2021. We identified cases by reviewing medical records in all health facilities in the affected sub county. We conducted a case-control study. We defined a case-household as a household with at least one self-reported and/or confirmed (by patient book) resident with malaria for the period of 1 May 2020 to 28 Feb 2021 in Nabitende sub-county. Results: Nabitende subcounty had 6,620 cases with an Attack rate(AR)=20/100. Females were the most affected with an AR=21% (3462/16600) compared to the males with an AR=11% (1796/16900). The mean age of cases line-listed was 17 years with a range of 0-96 years. Age-group that contributed high numbers was 0-5 years that accounted for 53.7%. Malaria in Nabitende subcounty had a Case Fatality Rate of 0.05%. Participating in recent political campaigns in late nights (OR=1.6; 95%CI=1-2.5), residing near waterlogged places (OR=2.5; 95%CI=1.4-4.4), and having a household located <500m from a swamp (OR=2.3(CI=1.4-3.8) were strongly associated with this outbreak. Also, the distance of households (<500m) to the rice and sugarcane fields during the outbreak was associated with malaria disease [rice; OR=2.2, CI (1.2-4.2), Sugarcane; OR=1.67, CI (1.03-2.7). Conclusion: This outbreak was triggered by favourable breeding sites within the community among which include: waterlogged places, distance from rice farms, and the household being near the swamp and it was also facilitated by participating in political campaigns late in the nights. We recommend increased coverage of mosquito nets and larviciding the water-logged areas.
Introduction
Despite wide implementation of malaria prevention measures such as indoor residue spraying, Long-lasting insecticide treated nets, and mass distribution campaigns, Uganda has the 3rd highest burden of malaria cases globally, accounting for 5% of all the world’s cases with 38.8 million malaria cases (1), (2).
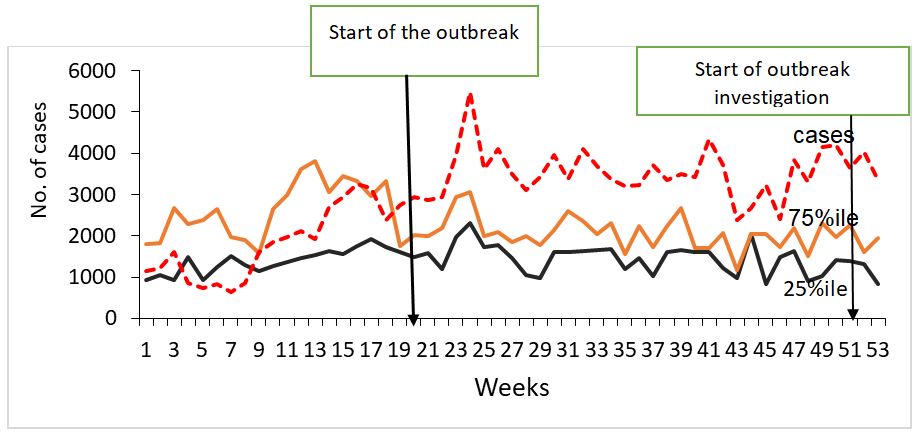
In February 2021, Ministry of Health (MOH) identified an upsurge in malaria cases in Iganga District, Eastern Uganda, exceeding expected limits (compared with malaria normal channels) (Figure 1). Using data extracted from the District Health Information System (DHIS2) and Subcounty populations, we calculated attack rates per subcounty. Calculated attack rates showed that Nabitende Subcounty was the most affected with an AR of 14/100 compared to other sub counties. We thus conducted an investigation in Nabitende Subcounty to determine the magnitude of the problem, identify risk factors for transmission, and recommend evidence-based control measures.
Methods
Outbreak setting
The Investigation was conducted in Iganga District. Iganga District is located in the Eastern part of the country. It has a population of 10,836500 with an annual population change of 3%.
Iganga experiences a warm, muggy, and cloudy weather through the year. Over the course of the year, the temperature typically varies from 62°F to 86°F and is rarely below 60°F or above 93°F. The wetter season lasts 8.2 months, from March 16 to November 23, with a greater than 54% chance of a given day being a wet day. The month with the most wet days in Iganga is April, with an average of 22.9 days. The drier season lasts 3.8 months, from November 23 to March 16 (3).
Case definition and Finding
We defined a confirmed case as a positive malaria test result using mRDT or microscopy in a resident of Iganga District from 1 May 2020 to 28 Feb 2021. Using the case definition, we systematically abstracted case-patient information on age, sex, village, subcounty, date of onset of fever, diagnostic test done and the test result from all the health facilities in Nabitende subcounty (the most affected subcounty).
Descriptive Epidemiology
We described the identified cases by date of admission and constructed an epidemic curve. We abstracted rainfall data from the National Aeronautics and Space Administration (NASA) (4) and examined rainfall patterns for the same period by superimposing the line graph on the epidemic curve to compare the number of cases by admission to rainfall patterns over the same period. We also calculated the attack rates by sex, village and parish of residence. We did not calculate attack rates by age-group because of failure to obtain the population breakdown by age.
Hypothesis generation
To identify possible contributors to the malaria outbreak, we conveniently sampled and conducted key informant interviews with 18 community members, seven health facility in-charges, and nine community leaders in the most affected sub-county.
Environmental assessments
We walked through the most affected villages to find out whether there were environmental and human factors that may have facilitated the upsurge in malaria cases during the outbreak period.
Case-control study
To test the hypotheses developed based on descriptive epidemiology, we conducted unmatched case-control study in the five most affected villages. We defined a case-household as a household with at least one self-reported and/or confirmed (by patient medical book) resident with malaria for the period of 1 May 2020 to 28 Feb 2021 in Nabitende sub-county. Self-reported cases had to describe drugs prescribed to be considered. Control households were those in which none of the household members had suffered from malaria in the period of 1 May 2020-28 Feb 2021. We interviewed one case or control per case- or control-household.
Each case or control was asked about ownership of mosquito nets, where they obtained the mosquito nets, if they participated in late night campaigns, wearing of long-sleeved clothes in the evening, treatment and completion of doses, if they slept under the mosquito nets the previous night, residing near water logged places, staying near the swamp and which agricultural field they were involved in and any human activity in the swamp. We collected data using Kobocollect and exported them to Epi Info 7.2.2.0 software for analysis. We calculated frequencies and proportions for categorical variables, and means and medians for continuous variables. We analysed outcome variables against possible exposures. For the case-control study, we developed case-control sets for analysis and obtained Mantel–Haenszel odds ratios. The magnitude of association was calculated with odds ratios at 95% confidence interval.
Results
Descriptive epidemiology
We identified 6,620 cases in Nabitende subcounty leading to an attack rate (AR)=20/100 and 3 deaths (case fatality rate=15/10000).
Females were the most affected with an AR=20% (3,462/16,600) compared to the males with an AR=11% (1,796/16,900). The mean age of cases was 17 years with a range of 5 months to 96 years. Age-group that contributed the highest number of cases was 0-5 years that accounted for 53.7%.
Table 1: Attack rates by parish, Nabitende Subcounty, Iganga District, December 2021- February 2021
| Parish | Frequency | Population | Attack rate/100 |
| Kasambika | 1247 | 5113 | 24 |
| Itanda | 1385 | 6164 | 23 |
| Bugono | 646 | 3398 | 19 |
| Ituba | 1123 | 7635 | 15 |
| Nabitende | 565 | 6222 | 9 |
| Naluko | 293 | 4519 | 6 |
In Nabitende sub-county, three parishes of Kasambika parish, Bugono parish, and Itanda parish were the most affected (Table 1).
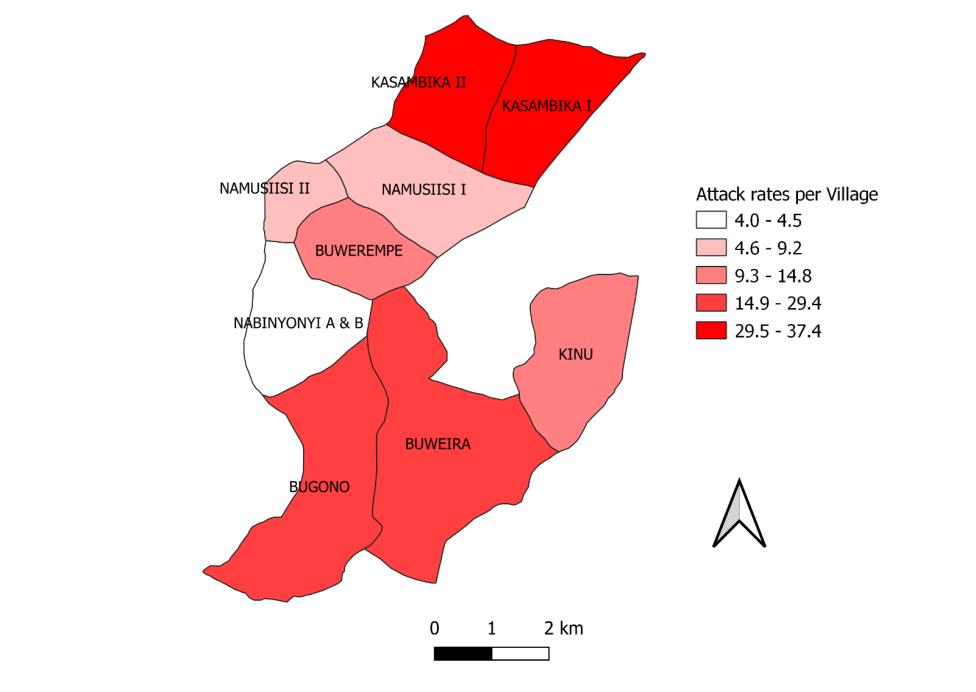
In these three parishes, Kasambika, Buweira , and Bugono, villages were most affected with an AR more than 14/100 persons (figure 2). As a result, we focused our case control study in these areas.
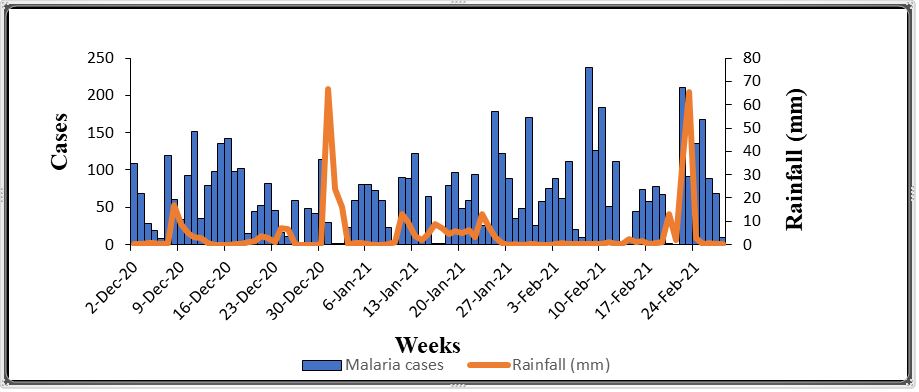
There was no distinct relationship between rainfall and the number of malaria cases recorded (Figure 2).
Hypothesis generation findings
During our walks through the villages, we observed most households were located in very close proximity to farm fields (sugar cane plantations, sweet potato plantations, rice farms, banana plantations). Interviews with 14 household heads indicated that 5 households had changed had their proximity to the farm fields in recent months, suggesting this as a possible factor associated with the outbreak. During home visits, we identified holes in houses where mosquitoes could pass through, even if the door was closed.
These holes were located in the space between the wall and the roof. We also identified trenches in rice fields that contained standing water, in which mosquito larvae were found. Water containers around homes as well as harvesting pots/ containers were also found to contain mosquito larvae. During the discussion with the community members, we learned that there had been a recent policy change on the sales of sugarcane to the factories. This effectively reduced the price and demand for sugar and made it substantially less profitable for farmers. As a result, many farmers had changed from sugarcane planting to rice planting. We considered this as a possible factor associated with the outbreak, since rice fields much more often hold standing water compared with sugarcane fields.
Among other exposure factors, we inquired about drug stockouts, which might facilitate outbreaks by allowing people to go untreated for their malaria infection, health facilities in-charges confirmed that they had no antimalarial stock-outs in health centres between May 2020-Feb2021. We also inquired about staying outside houses in late night hours, community members reported that they had participated in recently concluded elections.
Due to the COVID-19 outbreak, campaigns were not supposed to be conducted in person. To reduce the chance of detection, activities were instead conducted in the evenings and late-night hours. The election activities involved moving from door to door to solicit votes and also holding late-hour meetings. This increased the risk of people being exposed to mosquitos (describe how it works).
Table 2: Factors associated with malaria infection, Nabitende subcounty, Iganga District, December 2021- February 2021
| Exposure | %cases exposed | %controls exposed | OR | CI |
| Political campaigns in late hours | 68.8 | 31.2 | 1.6 | 1-2.5 |
| Water logging | 70.6 | 29.3 | 2.5 | 1.4-4.4 |
| Household close to the swamp (<500m) | 66.4 | 33.6 | 2.3 | 1.4-3.8 |
| Rice(<500m) | 48.0 | 15 | 2.5 | 1.2-4.2 |
| Sugarcane(<500m) | 168 | 90 | 1.7 | 1.0-2.7 |
| Ownership of mosquito nets | 64.4 | 35.6 | 1.4 | 0.9-2.1 |
| Water holding containers outside household | 65 | 35 | 1.6 | 0.8-3.3 |
| Open spaces on the house | 64.1 | 35.9 | 1.3 | 0.8-2.0 |
| Completion of antimalaria drugs | 78.7 | 21.3 | 1.5 | 0.4-4.9 |
| Changed occupation | 55.7 | 44.3 | 0.7 | 0.4-1.3 |
| Human activity in the swamp | 72.9 | 27.1 | 1.7 | 0.2-2.0 |
Participating in recent political campaigns (OR=1.6; 95%CI=1-2.5), residing near water logged places (OR=2.5; 95%CI=1.4-4.4), and having a household located <500m from a swamp (OR=2.3(CI=1.4-3.8) were strongly associated with this malaria outbreak. Also, distance of households (<500m) to the rice and sugarcane fields during the outbreak was associated with malaria disease [rice; OR=2.2, CI (1.2-4.2), Sugarcane; OR=1.67, CI (1.03-2.7)] (Table 2).
Discussion
Malaria has remained a big challenge in Uganda regardless of all the interventions implemented. Our findings indicated that the Malaria outbreak in Iganga had occurred six months before with Nabitende sub-county being the most affected, three parishes of Kasambika, Itanda and Bugono were the most affected. In these parishes, five villages: Kasambika, Buweira , and Bugono were more affected with an attack rate of more than
14/100 population. Participating in political campaigns late at night, residing near water logged places (within <500M), having household close to the swamp and having rice and or sugar farm field within 500m to the households were strongly associated with the outbreak.
People residing in households near waterlogged places were more likely to suffer from malaria. Waterlogged places tend to act as the breeding sites for the mosquitos. These findings are in agreement with a study done in Kyotera District identified waterlogging as significant factor associated the outbreak at the time (5). It is also in agreement with the study done by Godfrey N. who established that there was a strong association between staying near water logged areas and suffering from Malaria in a study done in northern Uganda (6)
Distance less than 500m from the household was also found to be significantly associated with malaria infection. Rice fields provide suitable breeding sites/places for anopheles mosquitos. While in the field, we saw trenches in the rice fields and these are dug by the owners of these rice fields to retain water in their farms. These later turn into breeding sites and since most of the rice farms were in a distance of <500m from households, mosquitos can fly and feast on people.
Households close to the swamps (<500m) were also associated with this malaria outbreak in Nabitende sub-county. These findings are similar to those of a study done by Baymot who found out that people living near swamps were more likely to be infected with malaria compared to those who stayed far (7). This is due to the presence of breeding sites in the swamps coupled with the fact that mosquitoes can fly up to a distance of 500m (8).
Study limitations
The controls used in our investigation were not tested. It is therefore possible that some of them might have been asymptomatic at the time of our investigation or at a certain point during the period considered for the investigation. Being asymptomatic controls might have led to an underestimation of the outcomes and associations in our study. Additionally, our study was only conducted in one subcounty, and cannot therefore be generalized to the entire district. It is also possible that some of the cases were tested and treated more than once in a healthy facility or at different health facilities because of non-adherence to treatment or reinfection. Testing and being treated more than once might have led to an overestimation of the magnitude of the outbreak.
Conclusion
This Malaria outbreak in Nabitende Sub-county was facilitated by proximity of households to mosquito breeding sites, that is, swamps, and agricultural fields (rice, sugarcane and banana). The change in agricultural practice, from sugarcane to rice farming might have also facilitated the outbreak. We recommended to the officials of Iganga District to strengthen their surveillance system by using Malaria Early Warning System and larviciding breeding sites (water logged places) in the area.
Public health actions
We implemented some immediate control measures in the affected communities and homesteads, and these included: Draining of pots and containers that were found to have stagnant water; we conducted health education about the importance of eliminating active and potential breeding sites for mosquitoes around homes; Emphasizing the need for proper and consistent use of treated mosquito nets; Sensitization of the community members and leaders on malaria and its prevention by using simple cost-effective strategies like wearing long sleeve clothes in evenings, closing windows and doors early, repurposing of old/damaged nets into curtains
Acknowledgement
We acknowledge Makerere university school of public health and Ministry of Health for the technical support during the execution of the study.
References
- World Malaria Report 2020 [Internet]. [cited 2021 May 31]. Available from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2020/
- Spatio-temporal prevalence of malaria and anaemia in relation to agro-ecosystems in Mvomero district, Tanzania | Malaria Journal | Full Text [Internet]. [cited 2021 Jul 2]. Available from: https://malariajournal.biomedcentral.com/articles/10.1186/s12936-019-2859-y
- Iganga Climate, Weather By Month, Average Temperature (Uganda) – Weather Spark [Internet]. [cited 2022 Jan 6]. Available from: https://weatherspark.com/y/97595/Average-Weather-in-Iganga-Uganda-Year-Round
- NASA [Internet]. NASA. [cited 2021 Sep 23]. Available from: http://www.nasa.gov/index.html
- Ministry of Health, Rotary partner to fight malaria [Internet]. [cited 2021 Jul 2]. Available from: https://www.independent.co.ug/ministry-of-health-rotary-partner-to-fight-malaria/
- Malaria Outbreak Facilitated by Appearance of Vector-Breeding Sites after Heavy Rainfall and Inadequate Preventive Measures: Nwoya District, Northern Uganda, February-May 2018 – PubMed [Internet]. [cited 2022 Jan 8]. Available from: https://pubmed.ncbi.nlm.nih.gov/32377206/
- Malaria outbreak investigation and contracting factors in Simada District, Northwest Ethiopia: a case–control study | BMC Research Notes | Full Text [Internet]. [cited 2021 Jul 2]. Available from: https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-019-4315-z
- Kigozi SP, Kigozi RN, Sebuguzi CM, Cano J, Rutazaana D, Opigo J, et al. Spatial-temporal patterns of malaria incidence in Uganda using HMIS data from 2015 to 2019. BMC Public Health [Internet]. 2020 Dec 14 [cited 2021 Sep 2];20(1):1913. Available from: https://doi.org/10.1186/s12889-020-10007-w
Reference this page as below
Immaculate Atuhaire*, Esther Kisakye1, Sherry Ahirirwe1, Hildah Nansikombi1, Shaban Senyange1, Stella Martha1, Rose Nampeera1, Patience Mwine1, Rose Nampeera1, Sarah Elayete1, Alice Asio1, Veronica Masanja1, Allan Komakech1, Edirisa Nsubuga1, Andrew Kwiringira1, Kwesiga Benon1, Daniel Kadobera1, Alex R. Ario1, and Julie Harris2. Malaria Outbreak facilitated by agricultural activities, residing near water logged areas and participating in late night campaign activities: Nabitende Subcounty, Iganga District, Kampala, Uganda. Uganda National Institute of Public Health. 2021 December 30th. Available from:https://uniph.go.ug/malaria-outbreak-facilitated-by-agricultural-activities-residing-near-water-logged-areas-and-participating-in-late-night-campaign-activities-nabitende-subcounty-iganga-district-december-2020-febru.
Comments are closed.