
Black Water Fever among children in Districts of Bugisu, Bukedi, and Busoga Region, Eastern Uganda, January 2019 – July 2021
Authors: Alice Asio1*, Veronica Massanja1, Andrew Kwiringira1, Stella Martha Migamba1, Esther Kisaakye2, Lilian Bulage1,2, Daniel Kadobera1,2, Benon Kwesiga1,2, Alex R. Ario1,2 Institutional affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda, 2Uganda National Institute of Public Health, Kampala, Uganda *Correspondence: Email: aasio@musph.ac.ug, Tel: +256788006553
Summary
Background: In May 2021, districts in Eastern Uganda reported an increase in suspected black water fever (BWF) affecting children, most <12 years of age. We investigated to confirm the outbreak, generate information on the causative agent, and describe the case-patients in terms of person, place, and time.
Methods: A suspected case was an onset of dark/red urine with at least one of the following: fever >37oC, anorexia, fatigue, abdominal pain, abdominal distention, anemia, jaundice, headaches, or vomiting in a patient attending Mbale, Soroti or Jinja Regional Referral hospitals (RRHs) of Eastern Uganda during January 2019 to May 2021. To describe the case-patients, we abstracted medical record data for cases identified from January 2019-May 2021. To generate information on the possible causative agent and also rule out other conditions in the case-patients, we collected blood, stool, and urine samples from 20 case-patients and 20 randomly selected non-case-patients (children admitted in the same ward as the case-patients) matching them with the hospital and tested them for ten different tests per case-patient and per non-case-patient. We defined non-case-patients as any patient with malaria admitted in pediatric wards of Mbale and Soroti RRHs who never passed out dark colored urine in their lifetime. We tested non-case-patients to find out if there could be any differences in BWF case-patients and non-case-patients. We also conducted pathogen discovery to find out the causative organism. We described the case-patients in terms of age of onset of illness, number of episodes, and intervals between episodes.
Results: According to the records review, we identified 4,913 case-patients, including 26 who died (CFR=0.5%). All 4,913 presented with dark-coloured urine, 2,617 (53%) with high-grade fever, and 2,295 (47%) with anaemia. Most case-patients (65%) were reported from Soroti RRH. The attack rates were similar in 2019 (AR=2.3/10,000) and 2020 (AR= 2.5/10,000). Males [2019: AR=3.2/10,000, 2020: AR= 3.3/10,000, and 2021(Jan-May): AR=1.5/10,000] were more affected than females in all the years of the records review period.
Among the 40 participants (20 cases and 20 non-cases-patients), the mean age was 4.5 (SD=2.4), ranging from 1 to 8 years. Case-patients and non-patients were nearly comparable in mean age (4.5 years among cases and 4.0 years among non-patients), and sex distribution (65% of case-patients and 55% of non-cases-patients were males). Among the case-patients, 20% (4/20), 20% (4/20), and 20% (4/20) developed the illness at the age of 2, 3, and 6-years respectively. 45% (9/20) of the case-patients had 1 to 3 episodes since the onset of the illness. 55.2% (48/87) of the case-patients experienced varying intervals between episodes and 70% (14/20) experienced the relapses of the illness after every 2-3 weeks. From the laboratory investigation, all the case-patients 100% (20/20) had low hemoglobin compared to the non-patients at 0% (0/20). None of the case and non-cases-patients tested positive for Hep B, syphilis, HIV, stool, and blood cultures never identified any organism in both stool and blood. Both case-patients (20/20) and non-case-patients (20/20) had malaria parasite seen on PCR and only 55% (11/20) of case-patients and 100%(20/20) of non-case-patients tested malaria positive by MRDT. Pathogen discovery findings are not yet out.
Preliminary conclusion: BWF caused substantial morbidity among children in Eastern Uganda during our study period. Case-patients experienced repetitive episodes. Future studies should focus further of the causative agent(s), triggers of BWF, and expand case capture sites to identify geographic boundaries of this problem in Uganda.
Introduction
Malaria is the leading cause of death in Uganda, accounting for 27% of the total deaths, of which 50% are among children under five years (President’s Malaria Initiative Uganda, Malaria Operation Plan FY 2018). Blackwater fever (BWF) is thought to be a complication of either severe malaria or malaria treatment. Among patients with BWF, red blood cells burst in the bloodstream (haemolysis), releasing hemoglobin directly into the blood vessels and into the urine, frequently leading to haemoglobinemia, hemoglobinuria, jaundice, anuria, kidney failure, and sometimes death ( 4). Treatment for BWF includes blood transfusion, antimalarials, folic acid and fluids. Children are more commonly affected than adults with sickle cell (12).
The causes of BWF remain unclear, and it is not known why some children with malaria develop BWF while others do not. Previous studies have suggested a link between BWF and quinine treatment or other antimalarials (8), rainy seasons, and low parasitemia (13). Other studies have suggested possible genetic contributors, such as genotype AA or G6PD deficiency (8, 5,10). The persistence of PCR-detectable parasitemia after administration of artemisinin-combination therapy (ACT) is often observed in asymptomatic children from endemic areas. The development of resistance to chloroquine led to the reintroduction of quinine and the introduction of mefloquine and halofantrine, and this has previously been associated with a reappearance of BWF (16). Treatment requires prompt transfusion to replace lost red blood cells, and sometimes a change in antimalarial drugs. Some of the countries that have reported BWF are France (1990-1999), Niger, Sierra Leone in 1889, Congo, Burundi and others (9, 14,6,13, 15). In all these countries, BWF was suggested to be associated with quinine use.
Although BWF is linked to malaria, it is not present everywhere malaria is present. Starting in 2009, cases of BWF began being reported in Eastern Uganda in the districts of Manafa, Soroti, Katakwi, Namutumba, and Namisindwa. Other areas of the country appear relatively unaffected. On May 29, 2021, a story ran in the Ugandan Newspaper New Vision about suspected BWF affecting children <12 years of age in Eastern Uganda. They reported that there were 13-16 admissions of children to Mbale Regional Referral Hospital from Mbale and the surrounding regions each day, and that some of the cases were fatal. The article noted that response to the conventional antimalarials – primarily artemether-lumefantrine – was poor. The Hospital Director reported that some of the cases were coming from outside their catchment area, i.e., Bukedea and Kumi both located in Bukedi region and Namutumba located in Busoga region. We investigated to confirm the outbreak, generate information on the causative agent, and describe the case-patients in terms of person, place, and time.
Methods
Outbreak setting
Cases were reported in the Eastern, is one of the four regions of Uganda. It has 37 districts with mixed tribes: Busoga, Bugishu, Bugweri, Samia, Teso, Jopadhola, and Kumam. The region has an approximate population of 13.6 million persons, representing approximately 14% of the country’s population. The major economic activity in this region is agriculture; growing of rice, millet, coffee, groundnuts, millet among other activities. Additionally, the population practices fishing in the lakes and rivers including swamps found in eastern Uganda. Furthermore, the eastern region has natural features like Mt Elgon, and many rocks.
Case definition and finding
We defined a suspected case as any patient with onset of dark/red urine with at least one of the following: high-grade fever, loss of appetite, fatigue, abdominal pain, abdominal distention, anemia, jaundice, headaches, or vomiting who attended either Mbale, Jinja, and Soroti RRHs of Eastern Uganda from January 2019 to May 2021.
We conducted records review in Soroti, Mbale, and Jinja RRHs to understand the historical pattern, seasonality, geographical patterns, and case-patients’ characteristics January 2019-May 2021. The current and past medical records were reviewed for the suspected cases including the deceased.
Laboratory investigations
To generate information on the possible causative agent and also rule out other conditions in the case-patients, we collected blood, urine, and stool samples from 20 case-patients and 20 non-patients from Mbale and Soroti RRHs. We considered Mbale and Soroti hospitals because they were the only hospitals receiving many case-patients, an average of 5-7 case-patients daily and Jinja RRH had no case-patients during the study period. A non-case-patient was any patient with any other condition admitted in pediatric wards of Mbale and Soroti RRHs who never passed out dark colored urine in their lifetime. We tested non-case-patients to find out if there could be any differences in BWF case-patients and non-case-patients. We tested for malaria parasites using both microscopy and PCR, Hep B using HBsAg test, sickle cell disease detect using HB electrophoresis, urinalysis using microscopy and ASTRA Care Dipsticks for proteins, Glucose, Ketones Leukocytes, Nitrites, Urobilinogen, Blood cells, Bilirubin, pH and Specific gravity, syphilis using T-pallidum Ab test, blood culture using ELISA (Giemsa staining and BD Bactec blood culture systems), HIV using HIV-1/2rapid test and CBC. We also conducted pathogen discovery to identify the possible causative agent.
We recruited cases sequentially and kept recruiting the cases until we reached the desired number. Non-case-patients were randomly selected from children admitted within the same ward. We administered a questionnaire to caretakers/parents.to collect information on socio-demographics, clinical presentation, natural history of the current suspected BWF episode, history of previous BWF episodes, medical history before the onset of the first episode of suspected BWF
Descriptive epidemiology
We analyzed data using Epi Info 7.2.2.6. Regarding the records review data, we generated epidemic curves, attack rates by year, sex, and age group using annual population estimates for the region by the Uganda Bureau of Statistics. We then generated proportions by number of episodes experienced by case-patients, distribution of case-patient by age group, age at onset of the illness, and number of intervals between the episodes. We also generated proportions to describe the case-patients by symptoms and signs experienced. We described the 20 case-patients and 20 non-case-patients by the laboratory investigation outcomes.
Ethical considerations
We obtained permission to conduct this this investigation from the Ministry of Health of Uganda through the office of the Director General Health Services. The Office of the Associate Director for Science, U.S. Centers for Disease Control and Prevention, determined that this activity was in response to a public health emergency with the primary intent of public health practice (epidemic disease control activity). It was determined therefore to not be human subjects research.
Furthermore, we obtained permission from the hospital directors of Mbale RRH, Soroti RRH, and Jinja RRH to access the paediatric wards suspected BWF related records, case-patients, and non-case-patients. Since all our participants were below 18 years of age, we sought verbal consent from their parents or guardians to allow us interview them and collect samples.
Results
Descriptive epidemiology
Distribution of case-patients by signs and symptoms, age group, and sex at Mbale, Soroti, and Jinja regional referral hospitals, January 2019-May 2021.
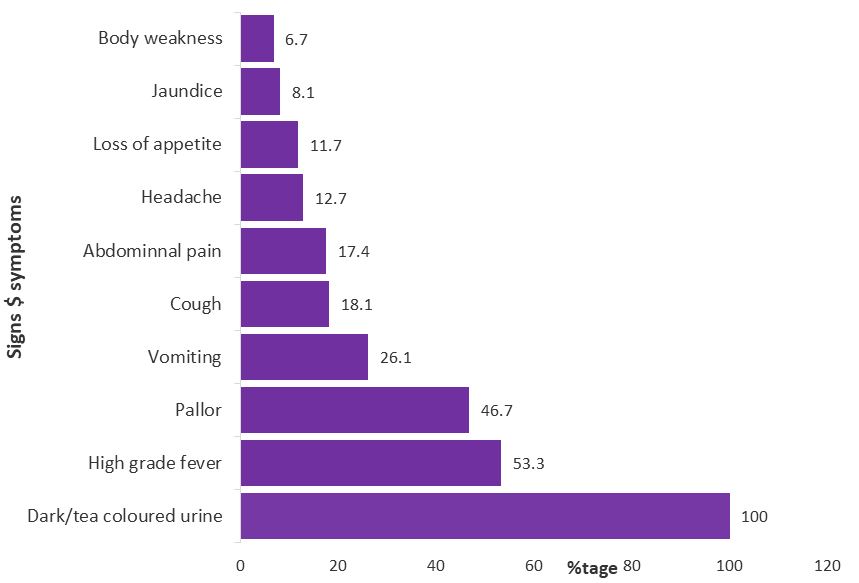
In total, 4,913 case-patients were identified, including 26(CFR=1%) for whom the hospital records recorded as dead. All the case-patients presented with dark coloured urine (100%), 2,617 (53.3%) with high grade fever, and 2,295 (46.7%) with anaemia (Figure 1).
Attack rates by age group and sex
The mean age of case-patient was 6 years (range, 21 days to 24 years). The most affected age group across the years was 5-9 years [2019: AR=4.7/10,000, 2020: AR= 5.0/10,000, and 2021(Jan-May): AR=2.5/10,000]. Males [2019: AR=3.2/10,000, 2020: AR= 3.3/10,000, and 2021(Jan-May): AR=1.5/10,000] were more affected than females in all the years of the assessment (Table 1).
Table 1: Attack rates by age group (N= 4,729)
| Year | Age group(yrs.) | Cases | Population <24yrs | Attack rates/10,000 |
| 2019 | 0-4 | 637 | 2,022,728 | 3.1 |
| 05-9 | 827 | 1,747,861 | 4.7 | |
| 10-15 | 323 | 1,798,804 | 1.8 | |
| 16-24 | 1 | 2,022,094 | 0.005 | |
| 2020 | 0-4 | 712 | 2,097,700 | 3.4 |
| 05-9 | 875 | 1,747,428 | 5 | |
| 10-15 | 400 | 1,910,296 | 2.1 | |
| 16-24 | 4 | 2,087,638 | 0.02 | |
| 2021(Jan-May) | 0-4 | 305 | 2,173,868 | 1.4(5Months) |
| 05-9 | 430 | 1,746,995 | 2.5 (5Months) | |
| 10-15 | 212 | 2,021,788 | 1.0(5Months) | |
| 16-24 | 3 | 2,153,182 | 0.01(5Months) | |
| Sex (4,695) | ||||
| 2019 | Female | 619 | 3,541,080 | 1.7 |
| Male | 1,166 | 3,636,670 | 3.2 | |
| 2020 | Female | 748 | 3,623,140 | 2.1 |
| Male | 1,219 | 3,742,580 | 3.3 | |
| 2021(Jan-May) | Female | 359 | 3,705,200 | 1.0 (5 months) |
| Male | 584 | 3,848,490 | 1.5 (5 months) |
Distribution of case-patients by regional referral hospital admitted and address of residence
Out of 4,913 case-patients, most case-patients were reported from Soroti RRH (64.9%), 21.3% were from Jinja RRH, and 13% from Mbale RRH. Among the 4,433 (90%) patients who had a known address, 95% were from the Eastern Region; 4% were from Central Region, and 1% were from Northern Region.
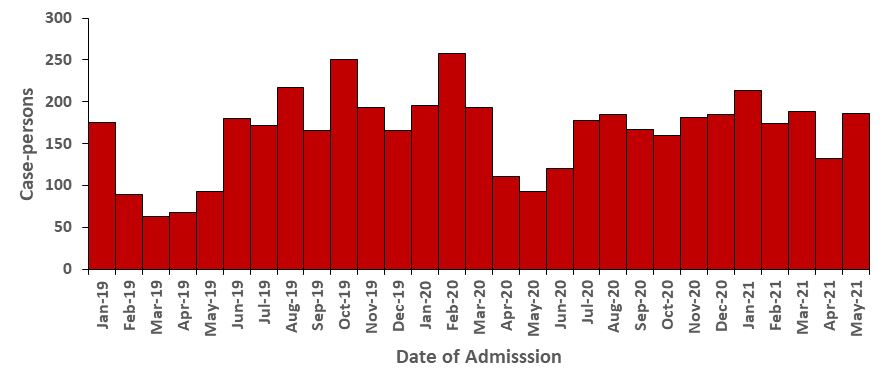
Distribution of case-patients by date of admission and attack rates over time
The number of case-patients admitted at health facilities have been increasing over years from 2019 to date (Figure 2). Case-patients admitted at health facilities increased gradually over years from 2019 [2019: AR=2.3/10,000, 2020: AR= 2.5/10,000, and 2021(Jan-May): AR=1.2/10,000].
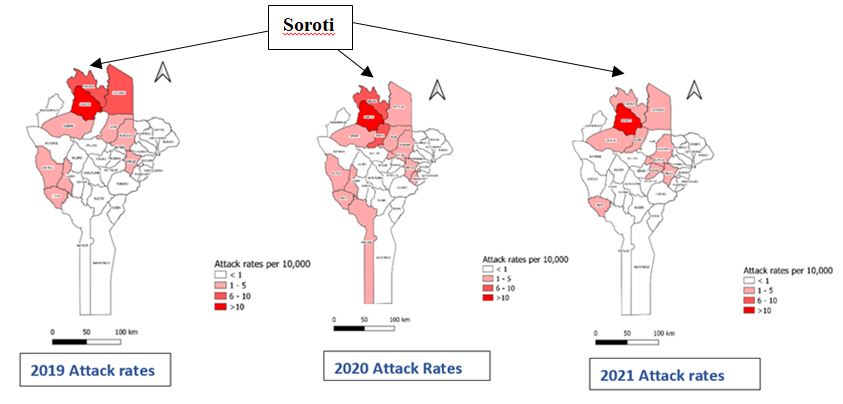
Attack rates of black water fever cases by district, eastern Uganda, January 2019-May 2021
District-specific attack rates varied over the eastern region, with Soroti District being the most affected across the years.
Description of 20 case-patients recruited for laboratory investigations
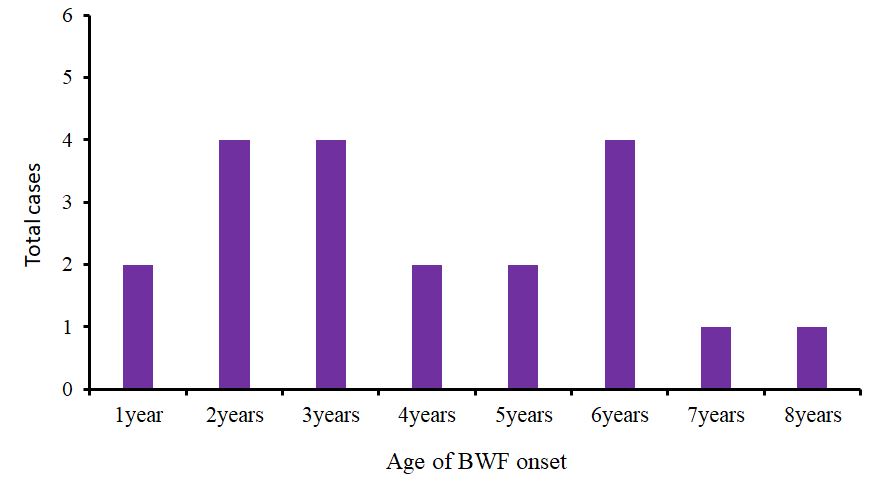
Age of onset and nature of episodes of black water fever
Twenty percent (4/20), 20% (4/20), and 20% (4/20) developed the illness at the age of 2, 3, and 6years respectively. 45% (9/20) of the case-patients had 1 to 3 episodes since the onset of the illness. 70% (14/20) of the case-patients experienced varying intervals between episodes and 70% (14/20) experienced the relapses of the illness after every 2-3week (Figure 4). All the case-patients had had recurrent episodes which subsides on treatment with anti-malarials, antibiotics, blood transfusion, and steroids and 30% (6/20) of the case-patients started getting episodes of the illness in 2018. 45% (9/20) of the case-patients had 1 to 3 episodes, 20% (4/20) had 7 to 9 episodes, 20% (4/20) had >10 episodes while 15% (3/20) had 4-6 episodes since the onset of the illness. 70% (14/20) of the case-patients experienced varying intervals between episodes, 25% (5/20) had an interval of 1-3weeks and 5% (1/20) had one-week interval between episodes.
Laboratory investigation findings
Laboratory investigation results as per records review
A total of 1,221 out of 4,913 case-patients were tested for malaria by RDT; 81.2% (991/1221) tested positive. Out of 4913, 775 were tested using microscopy; 61.5% (477/775) tested positive. A total of 682 out of 4,913 patients had their hemoglobin levels recorded. Among children less than 1 year, 95% (19/20) had low hemoglobin levels. For children aged 1-5 years and 6-11years, low hemoglobin levels were reported at 96.2% (378/393) and 95.6% (237/248) respectively. All those aged 12-24 years had low hemoglobin levels.
Laboratory investigation results for case-patients and non-case-patients
The case-non-cases-patients study included 40 participants (20cases and 20non-cases-patients) with a mean age of10.9(SD=11.2), ranging from 1 to 14 years. Case-patients and non-cases-patients were comparable in mean age (12.6 years among cases and 9.2 years among non-cases-patients), and sex distribution (65% of case-patients and 55% of non-cases-patients were males).
Hundred percent of the case-patients (20/20) had low hemoglobin while the non-case-patients had 20% (4/20) with low hemoglobin. 50% (10/20) of the case-patients had low platelet count compared to 40(8/20) for the non-case-patients (Table 2).
Table 2: Complete blood count findings for case-patients and non-case-patients
RBC (3.9-5.3*12/l) |
HB (11.5-14.5g/dl) |
Heamacrite(0.35-0.44l/l) |
MCV(73-85f/l) |
MCH (73-89pg) |
MCHC (30-37g/dl) |
RDW (11-16) |
Platelets(150-450*10g/l |
||
| Case | Normal | 3(15) | 0 | 18(90) | 16(80) | 12(60) | 12(60) | 8(40) | 8(40) |
| Low | 16(80) | 20(100) | 2(10) | 2(10) | 6(30) | 8(40) | 0 | 10(50) | |
| High | 1(5) | 0 | 0 | 2(10) | 2(10) | 0 | 12(60) | 2(10) | |
| Non-cases-pati
ents |
Normal | 6(30) | 16(80) | 4(20) | 17(85) | 16(80) | 9(45) | 7(40) | 10(50) |
| Low | 14(70) | 4(20) | 14(80) | 0 | 2(10) | 11(55) | 0 | 8(40) | |
| High | 0 | 0 | 2(10) | 3(15) | 2(10) | 0 | 12(60) | 2(20) |
Hundred percent (20/20) of the case-patients had low basophils compared to 85% (17/20) of the non-case-patients. 25% (5/20) case-patients had high WBC count compared to 10% (2/20) non-case-patient (Table 3).
Table 3: White blood cell count results case-patients and non-case-patients
WBC(515*10g/l) |
Neutrophils (1.58*10g/l) |
Lymphocytes (1.5-7*10g/l) |
Monocytes (0.2-0.8*g/l) |
Basophils (0-0.5*10g/l) |
Eosinophils0-0.3*10g/l) |
||
| Case | Normal | 14(70) | 12(65) | 13(65) | 10(50) | 0 | 2(10) |
| Low | 1(5) | 1(5) | 5(25) | 0 | 20(100) | 18(90) | |
| High | 5(25) | 6(30) | 2(10) | 10(50) | 0 | 0 | |
| Non-cases-patients | Normal | 10(50) | 11(55) | 10(50) | 13(65) | 3(15) | 1(5) |
| Low | 8(40) | 3(15) | 5(25) | 2(10) | 17(85) | 19(95) | |
| High | 2(10) | 6(30) | 5(25) | 5(25) | 0 | 0 |
Findings from other laboratory investigations
Blood cultures never identified any organism, no child turned positive for Hep B, none had syphilis, and all HIV test results were negative. Both case-patients (20/20) and non-case-patients (20/20) had malaria parasite seen on PCR and 55% (11/20) of case-patients and 100% (20/20) of non-case-patients tested malaria positive by MRDT.
Key findings
Based on our investigation, cases presented with signs and symptoms typical of BWF, a serious complication of severe malaria. Males were more affected compared to females across all the study period. Case-patients aged 5-9years were more affected. Soroti District registered the highest number of cases compared to all the districts in eastern Uganda. Case-patients developed illness at the age of 2, 3, and 6years with many experiencing between 1 to 3 episodes from the onset of the illness. Case-patients experienced varying intervals between episodes. The laboratory investigations showed significant difference in haemoglobin, and WBC count among the case-patients and non-case-patients.
Preliminary conclusion
BWF caused substantial morbidity among children in Eastern Uganda during our study period. Case-patients experienced repetitive episodes of illness. Future studies should focus further of the causative agent(s), triggers of BWF, and expand case capture sites to identify geographic boundaries of this problem in Uganda.
Acknowledgement
The authors would like to thank the management of Mbale, Jinja and Soroti RRH for allowing us carryout the investigation including the hospital staffs: Wandwasi Joseph (CO, Mbale RRH), Abeno Martha (Nurse, Soroti RRH) for helping in the recruiting the participants for the case-non-cases-patients study and collections of samples.
References
- Pasvol G: The treatment of complicated and severe malaria. Br Med Bull. 2005, 75–76: 29-47
- Rogier C, Imbert P, Tall A, Sokhna C, Spiegel A, Trape J-F: Epidemiological and clinical aspects of blackwater fever among African children suffering frequent malaria attacks. Trans R Soc Trop Med Hyg. 2003, 97: 193-197. 10.1016/S0035-9203(03)90116-7.
- Buffet PA, Safeukui I, Deplaine G, Brousse V, Prendki V, Thellier M, et al. The pathogenesis of Plasmodium falciparum malaria in humans: insights from splenic physiology. Blood. 2011;117(2):381–392.
- Ghosh JB. Black water fever. Indian J Pediatr. 2000;67(2):161–162.
- Van den Ende J, Van den Ende J, Coppens G, Verstraeten T, Van Haegenborgh T, Depraetere K, et al. Recurrence of blackwater fever: triggering of relapses by different antimalarials. Trop Med Int Health. 1998;3(8):632–639.
- Tran TH, Day NP, Ly VC, Nguyen TH, Pham PL, Nguyen HP, Bethell DB, Dihn XS, Tran TH, White NJ: Blackwater fever in southern Vietnam: a prospective descriptive study of 50 cases. Clin Infect Dis. 1996, 23: 1274-1281. 10.1093/clinids/23.6.1274.
- Dondorp AM, Fanello CI, Hendriksen ICE et al. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet. 2010, 376: 1647-1657. 10.1016/S0140-6736(10)61924-1.
- White NJ. Malaria. In: Cook GC, Zumla AI, editors. Manson’s tropical diseases. XXI ed. Philadelphia: W.B. Saunders; 2003. p. 1205–95. [Google Scholar]
- Bruneel F, Gachot B, Wolff M, et al. Resurgence of blackwater fever in long-term European expatriates in Africa: report of 21 cases and review.Clin Infect Dis. 2001; 32:1133–40. 10.1086/319743 [PubMed] [CrossRef] [Google Scholar]
- Bisoffi Z, Marocco S, Montero G, Marsiaj M. Acute intravascular haemolysis (blackwater fever) after malarial treatment.Trop Med Int Health. 1999; 4:72–3. [PubMed] [Google Scholar]
- Glanantonio CA, Vltacco M, Mendilaharzu F, Gallo GE, Sojo ET. The hemolytic-uremic syndrome. Nephron. 1973;11(2–4):174–192.
- Djibo A, Souna-Adamou A, Brah Bouzou S, 2000, Blackwater fever in adults with sickle cell anemia. Two fatal cases
- Bodi, J.M., Nsibu, C.N., Longenge, R.L. et al.Blackwater fever in Congolese children: a report of clinical, laboratory features and risk factors. Malar J 12, 205 (2013). https://doi.org/10.1186/1475-2875-12-205
- Mahamadou D, Hassane DM, Zeinabou MTM, et al. A report of Four cases of Black water fever after quinine treatment at Zinder National hospital, Niger Republic, Case Rep Infect Dis. 2019 Aug 25.
- Gobbi, Federico, et al. Blackwater Fever in Children, Burundi, Emerg Infect Dis, 2005 July.
- Danis M, Nozais, et al, 1993, Black water fever after taking 3 observations.
- Olupot-olupot, et al, The clinical spectrum of severe childhood malaria in Eastern Uganda, 2020
- Olupot-Olupot, et al. Characterising Childhood Blackwater Fever and Its Clinical Care at Two Tertiary Hospitals in Eastern Uganda, 2021
- Opoka et al, Blackwater Fever in Ugandan Children With Severe Anemia is Associated With Poor Postdischarge Outcomes: A Prospective Cohort Study,2020
Comments are closed.