
Anthrax outbreak associated with handling and consuming meat from animals that died suddenly, Ibanda District, Uganda, May 2023
Authors: Brian Kibwika1*, Edith Namulondo1, Dorothy Aanyu1, Yasiini Nuwamanya1, John Rek1, Dominic Kiza1, Adams Kamukama1, Innocent Ssemanda1, Susan Waako1, Mariam Komugishai1, Benigna Namara1, Daniel Orit1, Lawrence Tumusiime1, Shem Mwebaza2, Leah Naluwagga Baliruno2, Priscilla Atim2, Anthony Kiyimba2, Martha Annet Nankya2, Eugene Arinaitwe2, Gloria Bahizi2, Samuel Gidudu2, Richard Migisha1, Doreen N. Gonahasa1, Benon Kwesiga1, Daniel Kadobera1, Ario Riolexus Alex1 Institutional affiliations: 1Uganda Public Health Fellowship Program – Field Epidemiology Training Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Uganda Public Health Fellowship Program-Laboratory Leadership Program, Uganda National Institute of Public Health, Kampala, Uganda *Correspondence: Tel: +256782007573, Email: bkibwika@uniph.go.ug
Summary
Background: On March 24, 2023, Ibanda District reported seven suspected anthrax cases, after reportedly slaughtering, and eating meat from animals that died suddenly before slaughter at Kakijerere II village, Kagongo Division Ibanda District, Western Uganda. They all presented with blisters, oedema, and skin lesions typical of anthrax infection. Four days later, 6 cases were confirmed to be positive using PCR at Uganda Virus Research Institute (UVRI), Arua. We investigated the outbreak to determine its magnitude, identify possible exposures associated with it, and recommend evidence-based control interventions.
Methods: We defined a suspected cutaneous case as an acute onset of skin lesions (papule or vesicle) plus ≥2 of; skin itching, reddening, swelling, or regional lymphadenopathy that occurred between February 1, 2023 to April 21, 2023, in a person living in Ibanda District. A suspected gastrointestinal case was an acute onset of ≥2 of the following symptoms (abdominal pain, vomiting, diarrhoea, sore throat, mouth lesions, neck swelling), that occurred between February 1, 2023 to April 21, 2023 in a person living in Ibanda District. A confirmed case was a suspected case-patient with PCR-positive result for Bacillus anthracis. We identified cases by active case search in the affected community from house to house, reviewing health facility records, and snowballing from identified cases. We collected human, animal, and soil samples to test for the presence of Bacillus Anthracis. We conducted a case-control study with 24 cases and 108 controls (1:4 ratio). A control was defined as a resident of Kagongo division, Ibanda District from February 1, 2023 to April 21, 2023 with no symptoms at all and picked from the villages where the cases originated.
Results: We identified 24 cases (18 suspected and 6 confirmed), with one death (case fatality rate =4.2%), 18 (75%) were male. Of the 24 cases, 13 were cutaneous and 11 gastrointestinal, with a mean age of 37 years. The overall attack rate (AR) was 15.2/1000 and males were the most affected (AR=23.0/1000). The outbreak lasted for 32 days, from 3rd March 2023 to 3rd April, peaking on 16th March 2023. In the case-control investigation, 79% (19/24) of case patients compared to 16% (17/108) of control-persons ate meat from an animal that had died suddenly (aOR = 22.3; 95% CI: 3.5–139.3). In addition, 46% (11/24) of case patients compared to 1% (1/108) had participated in slaughtering an animal that had died suddenly (aOR = 51; 95% CI: 4.2–608.5). Compared to persons that did not eat or have contact with an animal that died suddenly, the odds of acquiring anthrax were highest among persons who ate and had contact with an animal that died suddenly (OR=178.2, 95% CI: 6.2-470), followed by persons that did not eat meat but had contact (OR=81, 95% CI:2.7-2431), with the lowest being among persons that ate the meat but had no contact with the animals that died suddenly (OR=54, 95% CI:6.2-470). We found evidence of Bacillus anthracis in the soil samples picked from the suspected grazing area from farm D where animals had recently died suddenly.
Conclusions: Our investigation revealed that the anthrax outbreak in Kagongo Division in Ibanda District was caused by handling and consuming meat from animals that died suddenly. We recommended increased surveillance and reporting of sudden livestock deaths and enforcement of livestock movement and quarantine, especially in known affected parts of the district.
Background
Anthrax is an acute zoonotic bacterial disease that is irregularly distributed worldwide in places where outbreaks occur regularly and is caused by Bacillus anthracis; a gram-positive, rod-shaped, spore-forming bacteria that are thought to survive for long in the carcasses and burial sites of infected animals. There are no reports of person-to-person transmission of anthrax, and the main transmission pattern to humans is mainly through handling or eating meat from infected animal carcasses, contact with their products (e.g. hair, wool, hides, bones), or by breathing in spores(1),(2),(3).
Historically human anthrax infection has been classified into four forms, depending on the route of exposure, with each having a differing degree of severity and incubation period; cutaneous (1–12 days), inhalational (1–60 days), gastrointestinal (1–6 days), injectional (1–10 days). Cutaneous anthrax is the most frequently reported form of human anthrax infection, accounting for up to 95% of cases, and is characterized by itching and skin lesions starting 1–7 days after infection, followed by depressed eschars(4).
Approximately 2,000 to 20,000 cases of human anthrax are reported globally annually, with most occurring in rural areas with low livestock vaccination rates. Uganda has reported anthrax outbreaks in the past among humans and livestock, and these outbreaks have mainly occurred in areas where people commonly keep livestock primarily within western, eastern, and northern Uganda(5),(6),(7).
On March 24, 2023, seven suspected anthrax case patients were reported to the District Health Team after reportedly skinning, carrying, and eating meat from an animal that died suddenly at Kakijerere II village, Kagongo division Ibanda District, Western Uganda. They all presented with blisters, oedema, and skin lesions typical of anthrax infection.
A total of seven human samples (7 whole blood and 7 swabs) were collected from suspected case patients and shipped via the hub system to Uganda Virus Research Institute (UVRI) Arua for analysis using PCR, of which 6 returned positive for Bacillus anthracis. Additionally, three cows were reported to have died suddenly within the same kraal in Kakijerere II village. We investigated to determine the scope and magnitude of the outbreak as well as identify possible exposures and recommend evidence-based control and prevention measures.
Methods
Outbreak area
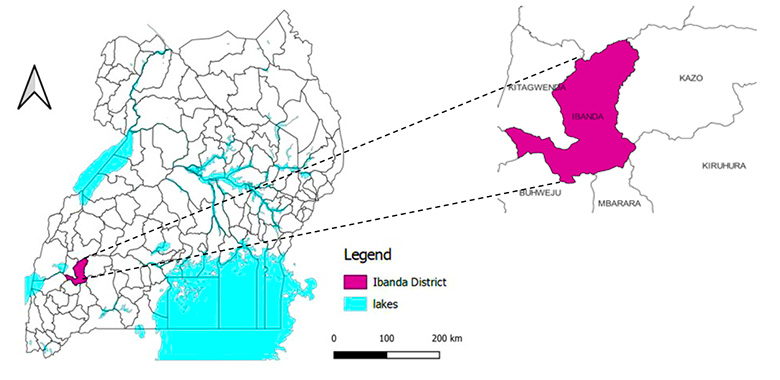
This outbreak occurred in Kagongo division Ibanda District which is located in southwestern Uganda (Figure 1). The District has a population of approximately 277,300 living in over 600 villages in 17 sub-counties with an average population density of approximately 287.2/km. Agriculture forms the backbone of the economy of the District, although most of it is at subsistence level.
Case definition and case finding
We defined a suspected cutaneous anthrax case as acute onset of skin lesions (papule or vesicle) plus ≥2 of; skin itching, reddening, swelling or regional lymphadenopathy that occurred between February 1, 2023 to April 21, 2023 in a person living in Ibanda District. We defined a suspected gastrointestinal anthrax case as acute onset of ≥2 of the following symptoms (abdominal pain, vomiting, diarrhea, sore throat, mouth lesions, neck swelling), that occurred between February 1, 2023 to April 21, 2023 in a person living Ibanda District. A Confirmed anthrax case was defined as a suspected case patient with PCR-positive results for Bacillus anthracis.
We conducted house to house and health facility active case search using a standard case definition to identify case patients in the affected areas since February 1, 2023. We also used snow-balling by asking already identified case patients to lead us to people with similar signs and symptoms in the community. We interviewed identified case-patients to identify possible exposures for contracting anthrax.
Descriptive epidemiology
We calculated proportions to describe the distribution of cases by age, sex, and symptoms. We further described case-patients by time of onset of symptoms using an epidemiological curve and calculated attack rates to describe the distribution of cases by place (village).
Laboratory investigations
In humans, seven whole blood and swabs were collected from anthrax-suspected cases and available fluids from lesions. In animals, seven swabs and body tissue (ear lobe) were collected from carcasses and animals already butchered. In addition, four soil samples from the suspected grazing area and the three slaughter areas were sampled. Rumen extracts from one of the slaughter areas were sampled. All samples were packaged using a triple package technique (tertiary leak-proof plastic container with ice packs for all except for soil samples) and transported using the hub system to the Uganda Virus Research Institute (UVRI) in Arua and the National Animal Disease Diagnostics and Epidemiology Centre (NADDEC) laboratory in Entebbe Uganda for human, animal, and soil sample testing. Anthrax confirmation was based on the identification of Bacillus anthracis by real-time PCR assay and GIEMSA blood smear for animal samples. Soil sample DNA extraction was done using the UltraClean® Soil DNA Isolation Kit MO BIO laboratories.
Environmental investigations
We interviewed case-patients and community center health workers to identify possible sources of contaminated meat and treatment options sought by those affected.
We inspected animal farms in the affected villages to identify those that had reported sudden death of cattle, goats or sheep between February 1, 2023 and April 21, 2023. We additionally gathered information on the farm management practices and how the meat and other animal products were distributed. We interviewed the identified dealers of meat for animals that had died suddenly to obtain information on the dates when the animals died and where the meat had been distributed/sold after slaughter.
Hypothesis generation interviews
We conducted 15 hypothesis generation interviews with the suspected cases to identify possible sources and factors associated with contracting anthrax. The interviews focused on consuming and handling meat from animals that had died suddenly, keeping of hides of animals that died since March 2023 and animal ownership by the respondent.
Case-control study
We conducted an unmatched case control study in the affected villages in Kagongo Division to test the generated hypotheses. We recruited and interviewed case-patients who met the case definition in the case-control study. For each case-person, we selected 4 control persons. A control-person was an individual who never had any signs of cutaneous or gastrointestinal anthrax from February 1, 2023 to the time of the investigation, resident in the same village as the case-person. To randomly select control-persons, we obtained the locations of case patients’ household and spun a bottle while at these households to obtain the first control-person household. The bottle was spun after every interview until the four different households were got. All members in the households were then listed and one was chosen randomly as a control-person.
For each case and control, we obtained information on their meat consumption history, contact with dead livestock (slaughtering, dressing, carrying), eating meat of an animal that had died suddenly, the clinical characteristics, as well as demographic variables.
We used logistic regression to identify factors associated with anthrax infection. Variables that had a p-value <0.2 at bivariate level were included in the final model for multivariable analysis and corresponding adjusted odds ratios (aOR’s) and 95% confidence intervals were reported. Common reference group analysis was conducted to assess the differences in the odds of infection based on combinations of the risk factors of anthrax in this study.
Ethical considerations
This outbreak investigation was in response to a public health emergency and was therefore, determined to be non-research. The Ministry of Health (MoH) gave permission to investigate this outbreak. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. §§See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.
The authors sought administrative clearance to conduct the investigation from Ibanda District health authorities. The authors also sought verbal informed consent and assent from the respondents accordingly. They were all informed that their participation was voluntary and their refusal would not attract any negative consequences. Unique identifiers were used to ensure confidentiality.
Results
Descriptive epidemiology
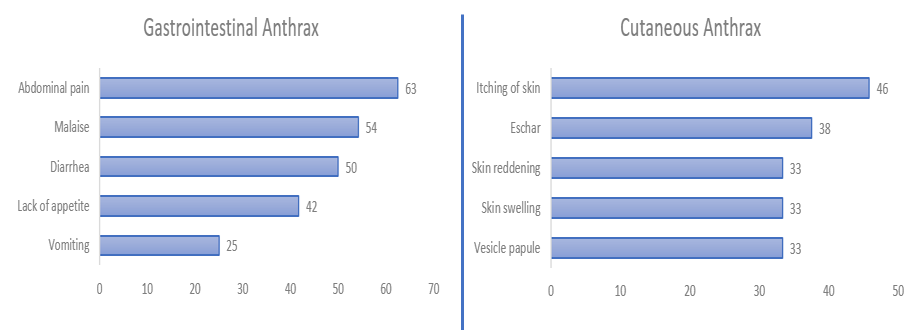
We line listed 24 anthrax case-patients, of which 6 were confirmed and one died (Case fatality rate=4%). Males were more affected (Attack rate [AR]: 22.0/1000) than females (AR: 8.6/1000). The village of Kakijerere I was the most affected (AR: 36.9/1000), followed by Kakijerere II (AR: 20.6/1000), and the least affected villages were Rwampanga (AR: 6.3/1000) and Kashambya (AR: 1.8/1000) (Table 1). Of the 24 cases, 13 were cutaneous and 11 gastrointestinal, with a median age of 32 and a mean of 34; (range: 4-84). The commonest symptoms amongst the case-patients with gastrointestinal anthrax were abdominal pain (63%), general body weakness and fever (54%), diarrhea (50%). Cutaneous anthrax case-patients presented with itching of skin (46%), eschars (38%), skin swelling and reddening (33%) (Figure 2).
After sudden death and slaughtering of the cow on March 3, 2023, cases started to appear from March 4, 2023 (Figure 3). The cases rapidly increased and peaked on March 16, 2023, after the second and the third cow died and were slaughtered. This epidemic curve suggests a multiple-source outbreak. The last case onset occurred on April 3, 2023.

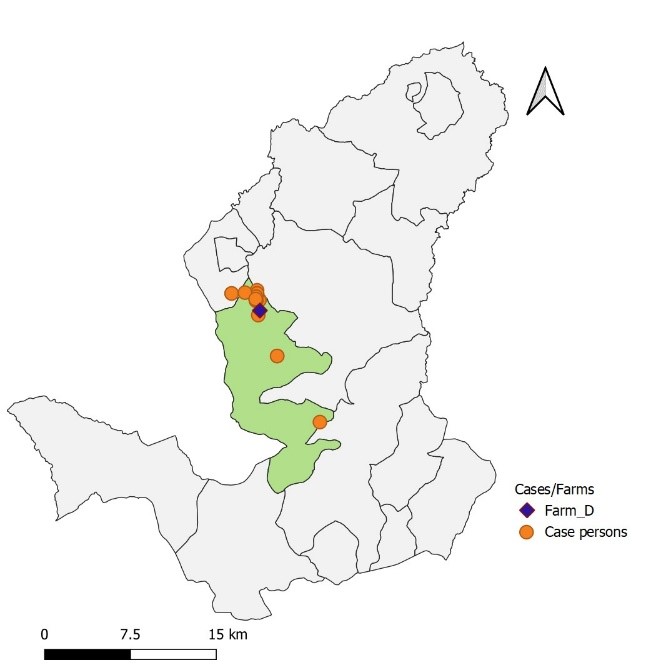
As of April 3, 2023, the outbreak had affected 4 villages in Kagongo Division, with Kakijerere I village being the most affected AR: 36.9/1000), followed by Kakijerere II (AR: 20.6/1000). Most of the case persons lived next to the farm with reported animal deaths in Kakijerere II (Figure 4).
Laboratory investigation findings
A total of 19 (seven human, seven animals, four soil, and one rumen content) samples were collected and tested for Bacillus anthracis. Six of the human samples returned PCR positive, while none of the seven animal samples turned positive by microscopic examination. The soil samples from the suspected grazing area, slaughter position 1 & 3 returned positive while slaughter area 2 and the rumen extract returned negative results.
Environmental assessment findings
There was a total of 6 suspected cases of animal anthrax in one farm (Farm D) which had two grazing areas, one in Kakijerere I and another one in Kakijerere II, separated by a marram road. Part of the grazing area in Kakijerere II was tilled for crops from 2021 to December 2022, the grazing in this part resumed in January 2023.
The first three animals to die on farm D were sold to the “dead animal meat dealer X’’ who slaughtered them with the help of others who also got infected and the meat sold in Kagongo Division. The last three animals were buried in 7ft deep pits on the pastureland. However, the burials were not supervised. An organized market dealing in cheap meat from animals that died suddenly was discovered in Ibanda District. The nurse in the community health center indicated that the case-patients bought antibiotics from her drug shop, but the deceased case patient only sought medical attention towards his death.
Hypothesis generation
Based on the 15 hypothesis generation interviews, 84% of respondents indicated they had consumed meat from an animal that had died suddenly, while 58% had handled animal products or participated in slaughtering animals that died suddenly. 32% had animal hides in their homes, while 21% owned animals in their homesteads.
We hypothesized that handling and consuming meat from animals that died suddenly were associated with the March 2023 anthrax outbreak in Ibanda District.
Case-control study findings
In the case-control investigation, 79% (19/24) of case persons compared to 16% (17/108) of control-persons ate meat from an animal that had died suddenly (aOR = 22.3; 95% CI: 3.5–139.3). In addition, 46% (11/24) of case persons compared to 1% (1/108) had participated in slaughtering an animal that had died suddenly (aOR = 51; 95% CI: 4.2–608.5) (Table 2).
Table 2: Distribution of exposure status among cases and controls during an anthrax outbreak: Ibanda District, Uganda, February – April, 2023
| Variables | N (%) | Crude ORs, CIs | Adjusted ORs, CIs | |
| Case (n=24) | Control (n=108) | OR (95% CI) | aOR (95% CI) | |
| Slaughtered a dead animal | 11 (46) | 1 (1) | 91.7 (6.0,1389) | 51 (4.2, 608.5) |
| Ate meat | 19 (79) | 17 (16) | 46.4 (6.5, 328.9) | 22.3 (3.5, 139.3) |
Compared to persons that did not eat or have contact with an animal that died suddenly, the odds of acquiring anthrax were highest among persons who ate and had contact with an animal that died suddenly (OR=178.2, 95% CI: 6.2-470), followed by persons that did not eat meat but had contact (OR=81, 95% CI:2.7-2431), with the lowest being among persons that ate the meat but had no contact with the animals that died suddenly (OR=54, 95% CI:6.2-470) (Table 3).
Table 3: Distribution of exposure status among cases and controls during an anthrax outbreak: Ibanda District, Uganda, February – April, 2023
| Ate meat | Touched meat | Cases n (%) | Controls n (%) | OR | 95% CI
|
| Didn’t eat | No contact | 1 (4.8) | 81 (81.8) | Ref |
|
| Ate meat | No contact | 8 (38.1) | 12 (12.1) | 54 | 6.2-470
|
| Didn’t eat | Contact with meat | 1 (4.8) | 1(1.0) | 81 | 2.7-2431
|
| Ate meat | Contact with meat | 11 (52.3) | 5 (5.1) | 178.2 | 19.0-1669
|
Discussion
Based on the epidemiologic, laboratory, and environmental assessments, we determined that this was a multiple point source cutaneous and gastrointestinal human anthrax outbreak associated with handling and eating meat from cows that had died prior to slaughter. Our results were consistent with other anthrax outbreak investigations conducted which indicated that the infection was as a result of consumption and contact with animals that had died suddenly(8),(9).
Ibanda District is situated adjacent to the cattle corridor of Uganda which is documented to have sporadic anthrax outbreaks over the years (5),(7),(10). Prior to the outbreak, animals dying suddenly in the community were reported, an indication of a possible anthrax as seen in previous outbreaks(5), (11), (12), (13). The outbreak was observed in four neighboring villages that were located near farm D, where the implicated animals had recently died suddenly and the meat sold to the communities by meat traders. Interviews with dealers in meat of animals that die suddenly also indicated that the Kagongo Division is one of their main areas of operation. Meat dealers of a similar kind have been documented to have distributed meat that lead to an anthrax outbreak in Kagongo in the past(14), which affirms the presence of the illegal trade in meat from animals that die suddenly.
The positive soil samples picked from the suspected grazing area and slaughter positions 1 and 3, further indicated that the animals that were slaughtered and sold to the Kagongo community had died of anthrax. This finding is consistent with studies that indicated survival of Bacillus anthracis in soil(2),(15),(16).
Adult males were the most affected. This group is most likely to be engaged in exposures to animal carcasses such as slaughter, skinning, transportation, and selling of such meat as evidenced in other studies relating to anthrax. (17),(18).
There was one human death reported in this outbreak, and according to a community health center nurse, it was due to delayed access to healthcare by the deceased case-patient, yet cutaneous anthrax has been shown to be fatal if not treated(4). The low case fatality rate could be explained by the prompt treatment that was given to the infected persons as soon as they reported any signs and symptoms consistent with anthrax. This was confirmed by the community health center nurse who saw a number of the case-patients purchasing antibiotics from her drug shop as soon as they experienced signs and symptoms related to anthrax.
The main sources of exposures were handling and consuming meat from animals that had died suddenly. Combination of the two main exposures by an individual posed the highest potential for cutaneous and gastrointestinal anthrax. Previous investigations of outbreaks in Uganda also found the association of anthrax to handling and eating of meat from animals that died suddenly before slaughter(5), (6), (10).
Study Limitations
The investigation had the following limitations: Some cases may not have been picked up during case-finding, given that they may have experienced mild, non-specific symptoms of anthrax. We were also unable to obtain samples of the meat from the implicated carcasses for testing, although the team was able to obtain soil samples from the grazing areas where the animals that died had grazed.
Conclusion
Our investigation revealed that the anthrax outbreak in Kagongo Division in Ibanda District was caused by handling and consuming meat from animals that died suddenly. We recommended increased surveillance and reporting of sudden livestock deaths by veterinary teams to the other sections of the One-Health team in the District so as to mount preparedness and response in case an outbreak occurs. We also recommended health education sessions to be conducted by the District Health Teams in the communities, regarding anthrax. We further recommended efforts to increase the laboratory capacity to handle outbreaks such as anthrax in the district.
Public health actions
Following the dissemination of our findings to the Ibanda district Health Team, continued surveillance in the district and recommendations to the district leadership to stop the markets dealing in meat from animals that died suddenly was done.
Conflict of interest
The authors declare no conflict of interest
Author contribution
BK, EN, SM, GB, SG, RM, DK, ARA, conceived and designed the study. KB, EN, DA, YN, JR, DK, AK, BN, IS, SW, MK, DO, LT, SM, LNB, PA, AK, MAN, contributed to data collection, cleaning and analysis. SM, LNB, PA, AK, MAN, EA, GB, SG, participated in coordination of laboratory work. BK, EN, SM, GB, SG, RM, DK, took lead in developing the original manuscript. All authors contributed to the final draft of the paper. All authors read and approved the final manuscript.
Acknowledgements
We thank the Ministry of Health for permitting us to respond to this outbreak. We thank the Ibanda district local government and the management of NTC for granting permission and overall guidance to the team.
Copyright and licensing
All material in the Uganda Public Health Bulletin is in the public domain and may be used and reprinted without permission. However, citation as to source is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Anthrax and wildlife – PubMed [Internet]. [cited 2023 Jun 16]. Available from: https://pubmed.ncbi.nlm.nih.gov/11974621/
- Organization WH. Anthrax in Humans and Animals. World Health Organization; 2008. 219 p.
- Aminu OR, Lembo T, Zadoks RN, Biek R, Lewis S, Kiwelu I, et al. Practical and effective diagnosis of animal anthrax in endemic low-resource settings. PLOS Neglected Tropical Diseases. 2020 Sep 14;14(9):e0008655.
- Types of Anthrax | CDC [Internet]. 2020 [cited 2023 Jun 14]. Available from: https://www.cdc.gov/anthrax/basics/types/index.html
- Nakanwagi M, Ario AR, Kwagonza L, Aceng FL, Mwesigye J, Bulage L, et al. Outbreak of gastrointestinal anthrax following eating beef of suspicious origin: Isingiro District, Uganda, 2017. PLOS Neglected Tropical Diseases. 2020 Feb 27;14(2):e0008026.
- Monje F, Kisaakye E, Ario AR, Eurien D, Ntono V, Kadobera D, et al. Anthrax Outbreaks among Domestic Ruminants Associated with Butchering Infected Livestock and Improper Carcass Disposal in Three Districts of Uganda, 2016-2018 [Internet]. In Review; 2020 Jan [cited 2023 Jun 14]. Available from: https://www.researchsquare.com/article/rs-11509/v1
- Musewa A, Mirembe BB, Monje F, Birungi D, Nanziri C, Aceng FL, et al. Outbreak of cutaneous anthrax associated with handling meat of dead cows in Southwestern Uganda, May 2018. Tropical Medicine and Health. 2022 Aug 6;50(1):52.
- Gombe N, Nkomo B, Chadambuka A, Shambira G, Tshimanga M. Risk factors for contracting anthrax in Kuwirirana ward, Gokwe North, Zimbabwe. Afr Health Sci. 2010 Jun;10(2):159–64.
- Chakraborty A, Khan SU, Hasnat MA, Parveen S, Islam MS, Mikolon A, et al. Anthrax Outbreaks in Bangladesh, 2009–2010. Am J Trop Med Hyg. 2012 Apr 1;86(4):703–10.
- Cutaneous anthrax associated with handling carcasses of animals that died suddenly of unknown cause: Arua District, Uganda, January 2015–August 2017 | PLOS Neglected Tropical Diseases [Internet]. [cited 2023 Jun 13]. Available from: https://journals.plos.org/plosntds/article?id=10.1371/journal.pntd.0009645
- Anthrax outbreak investigation in Tengwe, Mashonaland West Province, Zimbabwe, 2022 | PLOS ONE [Internet]. [cited 2023 Jun 14]. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0278537
- Outbreak of Anthrax Associated with Handling and Eating Meat from a Cow, Uganda, 2018 – PMC [Internet]. [cited 2023 Jun 13]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7706970/
- Bakhteeva I, Timofeev V. Some Peculiarities of Anthrax Epidemiology in Herbivorous and Carnivorous Animals. Life. 2022 Jun;12(6):870.
- Gastrointestinal-anthrax-outbreak-investigation-Ibanda-District-Southwestern-Uganda-August-2022-.pdf [Internet]. [cited 2023 Sep 7]. Available from: https://uniph.go.ug/wp-content/uploads/2023/07/Gastrointestinal-anthrax-outbreak-investigation-Ibanda-District-Southwestern-Uganda-August-2022-.pdf
- Does environmental replication contribute to Bacillus anthracis spore persistence and infectivity in soil? – ScienceDirect [Internet]. [cited 2023 Jun 14]. Available from: https://www.sciencedirect.com/science/article/abs/pii/S092325082300027X
- Driciru M, Rwego IB, Ndimuligo SA, Travis DA, Mwakapeje ER, Craft M, et al. Environmental determinants influencing anthrax distribution in Queen Elizabeth Protected Area, Western Uganda. PLOS ONE. 2020 Aug 18;15(8):e0237223.
- Islam MdS, Hossain MJ, Mikolon A, Parveen S, Khan MSU, Haider N, et al. Risk practices for animal and human anthrax in Bangladesh: an exploratory study. Infection Ecology & Epidemiology. 2013 Jan 1;3(1):21356.
- Risk factors for human cutaneous anthrax outbreaks in the hotspot districts of Northern Tanzania: an unmatched case–control study | Royal Society Open Science [Internet]. [cited 2023 Sep 16]. Available from: https://royalsocietypublishing.org/doi/full/10.1098/rsos.180479
Comments are closed.