
Temporal trends and spatial distribution of meningitis-related mortality in Uganda, 2021–2025
Authors: Kyomugisha Denise Aman1*, Richard Migisha1, Irene Kyamwine1, Benon Kwesiga1 Institutional Affiliations: 1Uganda Public Health Fellowship Program, Ugandan National Institute of Public Health, Kampala, Uganda Correspondence*: Email: akyomugisha@uniph.go.ug; Tel: +256759803507
Summary
Background: Meningitis is an important cause of preventable mortality in Uganda, with deaths linked to epidemic-prone bacterial pathogens and HIV-associated opportunistic infections. Mortality trend data are useful for identifying high-burden populations and guiding prevention and case management priorities. We assessed temporal trends in meningitis-related mortality in Uganda during 2021–2025.
Methods: We analyzed aggregated meningitis mortality surveillance data reported by health facilities through the District Health Information Software during 2021–2025. A meningitis death was an inpatient death recorded under bacterial, viral, cryptococcal or other type of meningitis in the health unit inpatient monthly reporting form. Mortality rates per 100,000 population were calculated using reported meningitis deaths and annual projected population denominators from the Uganda Bureau of Statistics 2024 Census Report (2.9% annual growth). Mortality rates were disaggregated by year, age group, sex, and meningitis type. Temporal trends in mortality rates were assessed using the Mann-Kendall test.
Results: During 2021–2025, national mortality rates were highest in 2021 (1.26/100,000) and lowest in 2023 (1.07/100,000), representing a 15% decline from 2021 to 2023. Over the 5 years, mortality rates were highest among males (1.25–1.58/100,000), those aged ≥5 years (0.88–1.01/100,000), and for cryptococcal (0.36–0.49/100,000) and bacterial (0.43–0.46/100,000) meningitis. No statistically significant monotonic trends in mortality rates were observed by year, age group, sex or meningitis type. Five of 146 districts (3%) had statistically significant declining trends in mortality rates; Sembabule (τ=-0.95, p=0.04), Kasese, Kiboga, Mubende and Gulu City (all τ=-1.0, p=0.03).
Conclusion: During 2021–2025, meningitis mortality rates were highest among males and individuals aged ≥5 years. Declining mortality trends were observed in a few districts. Further clinical and programmatic review could identify opportunities to reduce meningitis-related deaths.
Background
Meningitis is inflammation of the membranes surrounding the brain and spinal cord. It may be caused by bacterial, viral, fungal, or non-infectious conditions and commonly presents with fever, headache, neck stiffness, confusion, photophobia, and vomiting (1). Bacterial meningitis is the most severe form because it can progress rapidly, cause outbreaks and lead to death or long-term complications (1,2).
Uganda lies within the extended African meningitis belt, a region affected by recurrent bacterial meningitis outbreaks (3–5). Although vaccination against major bacterial pathogens has reduced vaccine-preventable meningitis in many settings, meningitis remains a public health concern in Uganda, with a bacterial meningitis cluster reported in Obongi District in 2023 (3). In addition, Uganda’s high HIV burden means that adult meningitis is also shaped by opportunistic infections, particularly cryptococcal meningitis (6–12). Previous Ugandan studies have shown that cryptococcal meningitis is a leading cause of HIV-associated adult meningitis and continues to cause substantial mortality, even with ART expansion (10,11,13–15).
Both epidemic-prone bacterial pathogens and HIV-associated opportunistic infections therefore drive meningitis mortality in Uganda. However, most available studies have focused on clinical cohorts in referral hospitals, and less is known about national and regional mortality patterns using routine surveillance data. We described national, regional, and district trends in meningitis-related mortality in Uganda during 2021 to 2025.
Methods
Study setting: We utilized data generated by healthcare facilities in all districts and regions in Uganda. These healthcare facilities included health centre IIIs, health centre IVs, general hospitals, regional referrals, and national referral hospitals. Meningitis cases are managed as admitted cases in these facilities.
Study design and data source: We conducted a descriptive analysis of aggregated meningitis-related health facility mortality surveillance data in Uganda reported during 2021 to 2025. We abstracted annual meningitis mortality data, including meningitis deaths and cases reported by healthcare facilities through the Ministry of Health District Health Information Software using the Health Unit In-patient Monthly Reporting Form (HMIS108) for 2021 to 2025. Data cleaning, population projections and statistical analyses were conducted using R Statistical Computing software version 4.2.3. The study population included all meningitis deaths and cases reported in HMIS 108 from January 2021 to December 2025. A meningitis death was defined as an inpatient death recorded in HMIS 108 under diagnoses of bacterial, viral, cryptococcal or other types of meningitis. A meningitis case was defined as an inpatient admission recorded in HMIS 108 under diagnoses of bacterial, viral, cryptococcal or other types of meningitis.
Study variables: The outcome was the meningitis mortality rate, expressed per 100,000 population. We defined the meningitis mortality rate as the proportion of meningitis deaths in the total population. Mortality rates were disaggregated by year, region, age group, sex, and meningitis type. Annual meningitis deaths were summarized by year at national, and district levels. National-level deaths were further disaggregated by age group, sex, and meningitis type.
Data analysis and management: Population data were obtained from the 2024 Uganda National Population and Housing Census Report published by the Uganda Bureau of Statistics. Annual population denominators for 2021 to 2025 were estimated using 2.9% exponential annual growth projections (16). Projected population denominators were aligned with the relevant level of analysis, including national, regional, age-specific and sex-specific analyses.
Meningitis mortality rates were calculated as the number of reported meningitis deaths, divided by the projected population for the same year, multiplied by 100,000.
Temporal trends in national, regional, and district mortality rates were assessed using the nonparametric Mann-Kendall test for monotonic trends. District meningitis mortality rates per 100,000 population over the 5 years were visualized using choropleth maps generated in Quantum Geographical Information Software.
Ethical considerations: This descriptive study was conducted under the direction of the Ministry of Health of Uganda. This analysis used aggregated surveillance data reported through DHIS2; no individual identifiers were accessed, and consent was not applicable. The Office of the Associate Director for Science at the US Centres for Disease Control and Prevention (CDC) Uganda determined that this investigation was non-research and that its primary intent was public health practice or disease control.
Results
Trends in meningitis mortality rates per 100,000 by year, sex, age group, meningitis type, region, and district, Uganda, 2021–2025
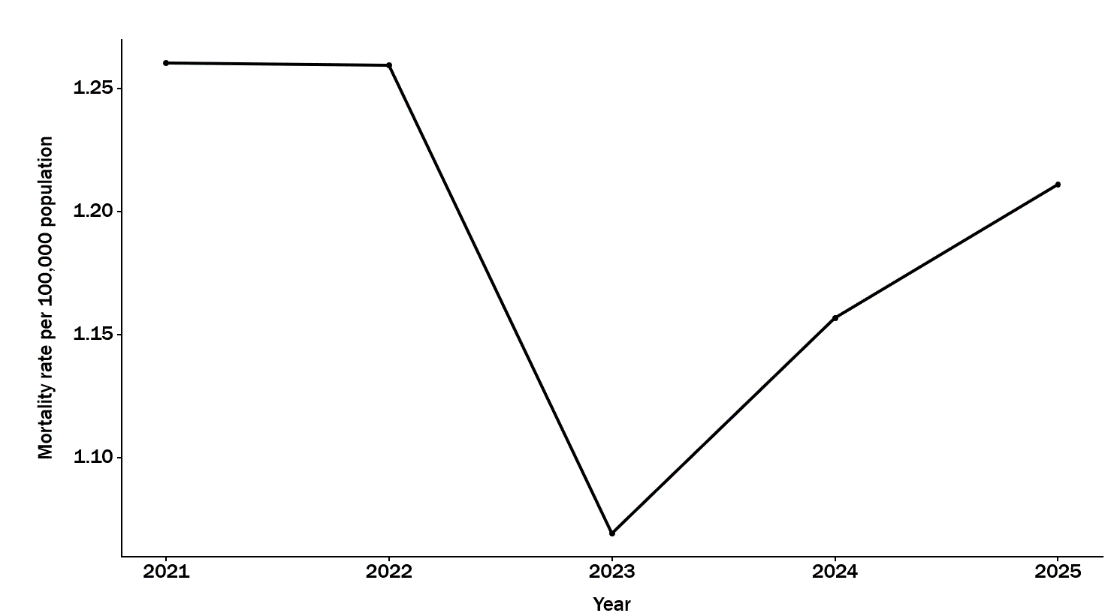
During 2021–2025, 2,657 deaths were reported. The national meningitis mortality rates by year ranged from 1.07−1.26 deaths per 100,000 population. Rates declined from 2021 to 2023, then increased by 2025, but the overall trend was not statistically significant (τ = -0.40, p = 0.46) (Figure 1).
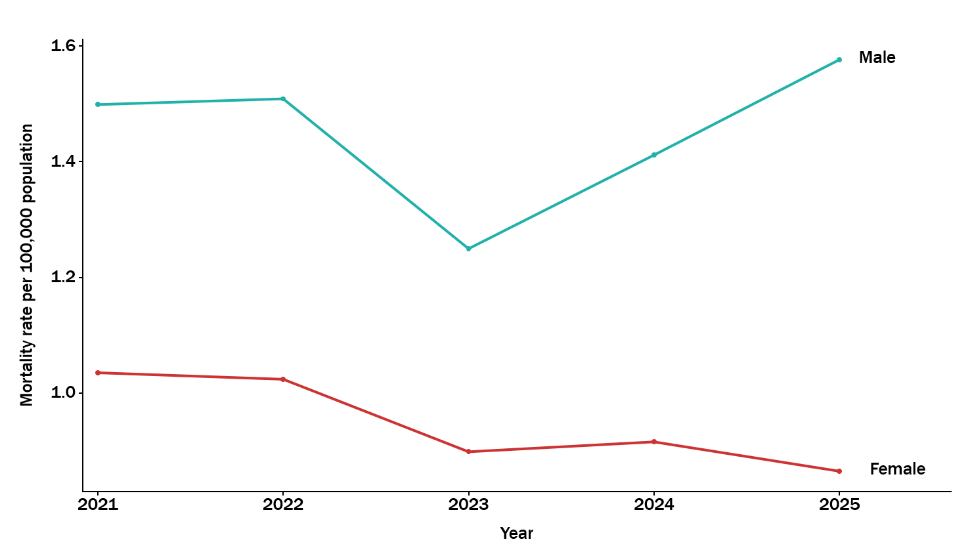
Males accounted for 1,573/2,657 (59%) deaths compared with 1,084/2,657 (41%) among females. Meningitis mortality rate by sex ranged from 1.25−1.58 deaths/100,000 for males and from 0.87-1.03 deaths/100,000 for females for the
5-year period; with no statistically detectable trend in among males (τ = 0.20, p = 0.81) or females (τ = -0.80, p = 0.09) (Figure 2).
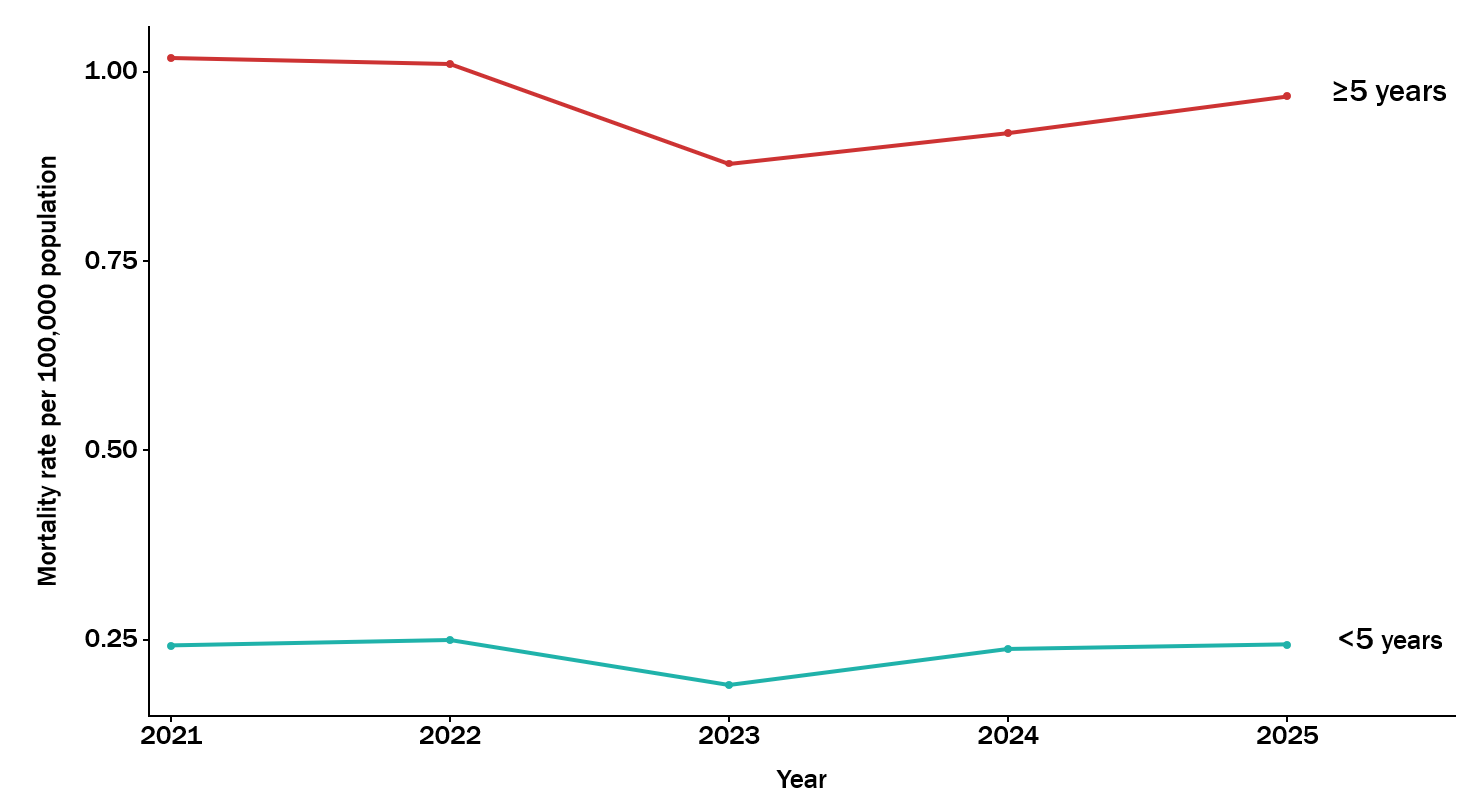
Among those aged ≥5 years, 2,138/2,657 (80%) deaths occurred compared to 519/2,657 (20%) deaths among those aged <5 years. Meningitis mortality rate by age group ranged from 0.88-1.02 deaths/100,000 for those aged ≥5 years and from 0.19−0.25 deaths/100,000 for those aged <5 years for the 5 years. Similarly, trends were not significant for the≥5 years age group (τ = −0.4, p = 0.46) or the <5 years age group (τ = 0.0, p = 1.0) (Figure 3).
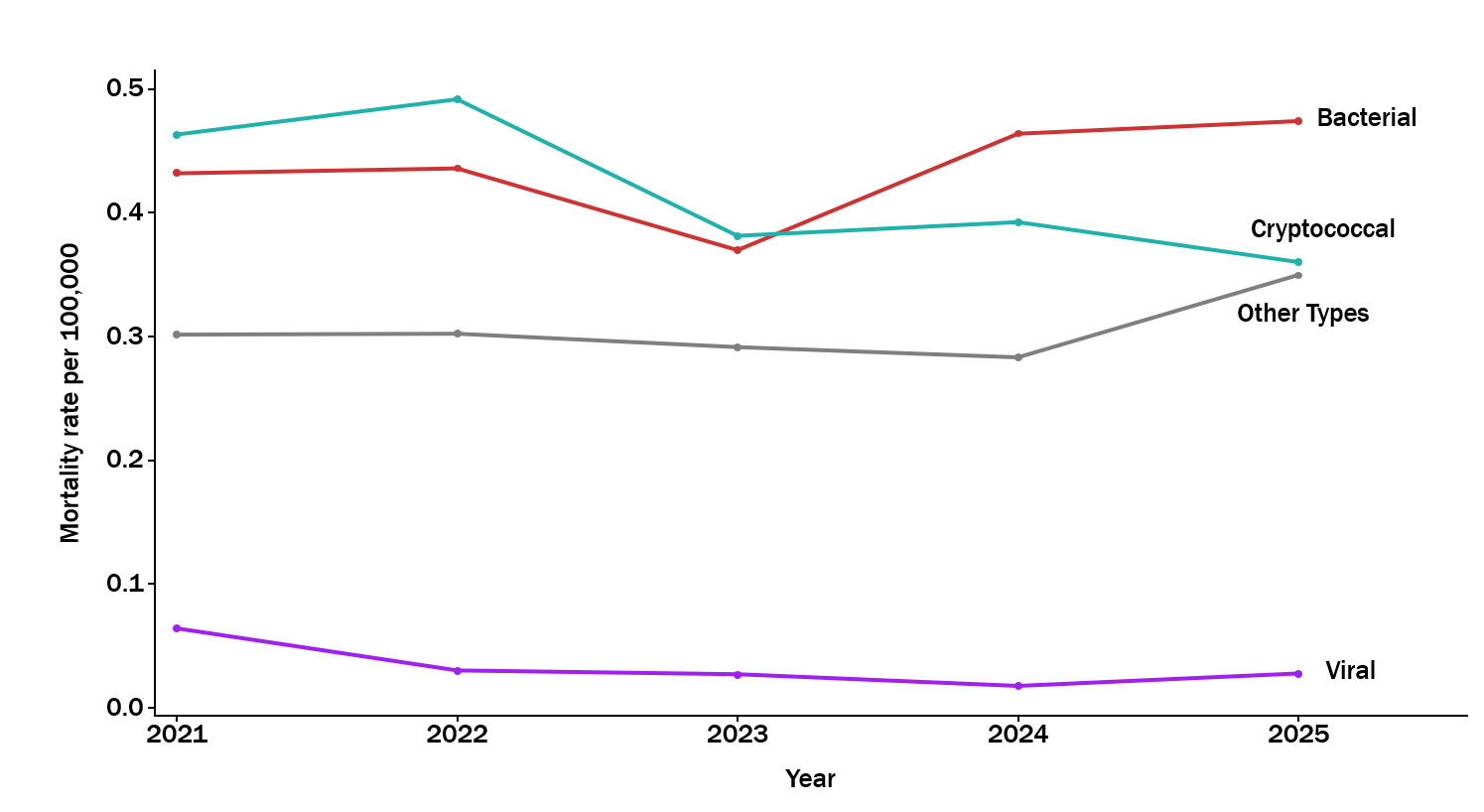
Bacterial meningitis accounted for 973/2,657 (37%) deaths, cryptococcal meningitis for 928/2,657 (35%) deaths, other types of meningitis for 683/2,657 (26%) deaths and viral meningitis for 73/2,657 (3%) deaths. Meningitis mortality rate by meningitis type ranged from 0.37−0.47 deaths/100,000 for bacterial meningitis, from 0.36-0.49 deaths/100,000 for cryptococcal meningitis, from 0.28−0.35 deaths/100,000 for other types of meningitis, and from 0.02-0.06 deaths/100,000 for viral meningitis for the 5 years. There was no statistically significant trend by meningitis type (bacterial: τ = 0.60, p = 0.22, cryptococcal: τ = -0.60, p = 0.22, other types: τ = 0.00, p = 1.00, viral: τ = -0.60, p = 0.22) (Figure 4).
Spatial distribution of mortality rates by district in Uganda, 2021–2025
At the district level, higher mortality rates were observed in several small urban districts (cities) which have regional referral hospitals, and this pattern of higher mortality persisted for the 5 years. These cities include: Kampala City, Gulu City, Lira City, Soroti City, Mbale City, Hoima City, Fort Portal City, Masaka City, Mbarara City and Kabale District (Figure 5)
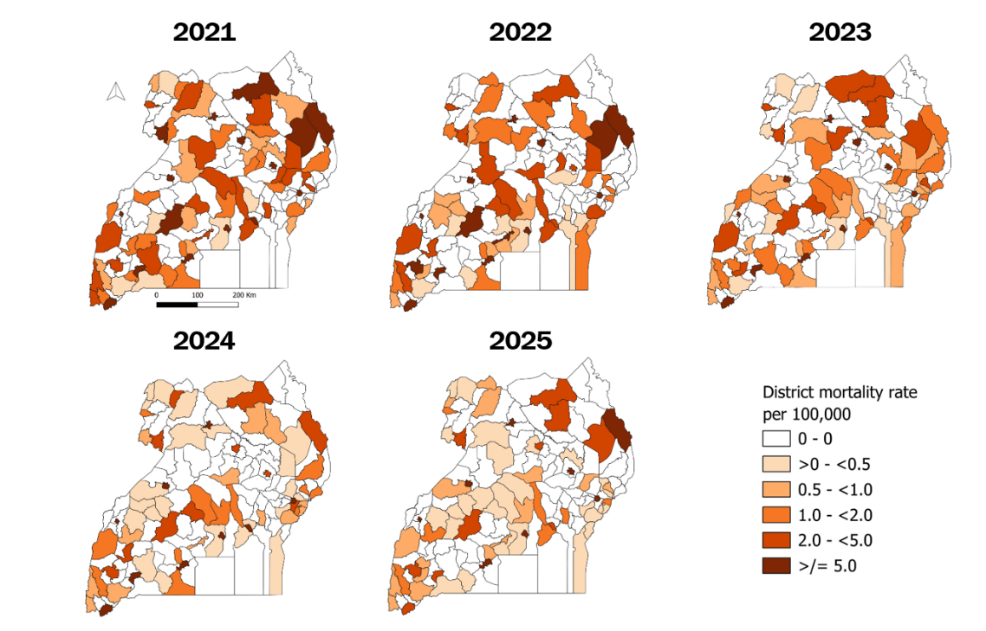
Figure 5: Spatial distribution of annual meningitis mortality rates by district in Uganda, 2021-2025
Discussion
This analysis of national routine mortality surveillance data showed that meningitis-related mortality in Uganda fluctuated during 2021–2025, declining from 1.26 deaths per 100,000 population in 2021 to 1.07 in 2023, then increasing to 1.21 in 2025. No statistically detectable monotonic trend in overall mortality or within demographic or clinical subgroups were identified. This indicates that the observed year-to-year changes did not follow a consistent pattern during the study period.
Mortality was consistently higher among individuals aged ≥5 years than among children aged <5 years, with this age group accounting for 4 in 5 reported meningitis deaths. This may partly reflect the contribution of HIV-associated opportunistic infections (1,2), including cryptococcal meningitis, among older age groups (17,18).
Males also had consistently higher mortality rates than females. This pattern is consistent with evidence of poorer health-seeking behaviour and delayed engagement in care among men in sub-Saharan Africa (19). Some studies have reported higher mortality among women, particularly where anaemia is present (17,20).
By meningitis type, bacterial and cryptococcal meningitis had the highest mortality rates, while viral meningitis had the lowest. This finding suggests that meningitis mortality in Uganda is shaped by both epidemic-prone bacterial meningitis and HIV-associated opportunistic infections. This differs from settings where meningitis burden is dominated mainly by epidemic-prone bacterial disease. This is also consistent with Ugandan and regional evidence showing that cryptococcal meningitis remains an important cause of death among people living with HIV (4,5,8,9,21).
These findings are relevant to regional meningitis control priorities and the WHO roadmap to defeat meningitis by 2030, which emphasizes reducing meningitis deaths, strengthening surveillance, improving diagnosis and care and preventing long-term complications (22).
At district level, some of the highest mortality rates were observed in small urban districts or cities hosting regional referral hospitals. These areas may appear as hotspots because they receive referred patients from surrounding districts and may have stronger diagnostic and reporting capacity. Routine surveillance data are useful for describing broad national and subnational patterns, detecting outbreaks and estimating disease burden, but they provide less clinical detail than patient-level studies and depend on the quality of case detection, reporting and laboratory confirmation (23). Therefore, these findings should be interpreted as surveillance-based patterns of reported inpatient mortality rather than complete estimates of all meningitis deaths in the population.
Study limitations: Several limitations should be considered. The five-year study period provided only five annual time points, which limited the ability to detect trends, especially non-linear patterns. The analysis used aggregated routine surveillance data which may have masked local variation and may have been affected by incomplete reporting, delayed reporting, data entry errors or misclassification. Because the data were based on inpatient reports from healthcare facilities, meningitis cases and deaths occurring in the community or non-reporting units were not captured. Therefore, mortality rates may underestimate the total burden of meningitis-related deaths in the population. Population denominators were based on projections from the 2024 census and may not fully reflect regional demographic differences. Subgroup analyses also reduced the number of observations available for trend analysis.
Conclusion: No statistically detectable monotonic trend in overall mortality, case fatality, age, sex or meningitis type was observed during 2021–2025. Mortality was consistently higher among males and individuals aged ≥5 years, and bacterial and cryptococcal meningitis contributed the greatest mortality burden. The facility-level case fatality rate of 11% indicates substantial mortality among admitted cases. Further clinical and programmatic review could help to identify factors contributing to meningitis-related deaths and opportunities to improve patient outcomes.
Recommendations: The Ministry of Health could conduct focused clinical and programmatic reviews in facilities and districts reporting high meningitis deaths or high case fatality, especially for bacterial and cryptococcal meningitis. These reviews could assess diagnostic practices, referral pathways, treatment practices and outcomes among admitted patients, especially males and persons aged ≥5 years. Findings from these reviews could guide targeted improvements in diagnosis, inpatient care and meningitis surveillance within and outside healthcare facilities.
Conflict of interest: The authors declare that they had no conflict of interest.
Authors’ contribution: KDA and RM conceived, designed, analyzed, interpreted the study and wrote the draft bulletin. IK, and BKreviewed the bulletin to ensure intellectual content.
Acknowledgments: The authors convey their gratitude to the Ministry of Health for approving the utilization of mortality surveillance data on the District Health Information Software – version 2.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission. However, citation as to source is appreciated. Any article can be reprinted or republished. If cited as a reprint, it should be referenced in the original form
References
- Meningitis [Internet]. [cited 2026 Feb 20]. Available from: https://www.who.int/news-room/fact-sheets/detail/meningitis
- Defeating Meningitis by 2030 [Internet]. [cited 2026 Feb 20]. Available from: https://www.who.int/initiatives/defeating-meningitis-by-2030?utm
- Link A, Okwir M, Nabongo B, Okello F, Alal J, Meya D, et al. Meningitis diagnosis, treatment, and outcomes in rural, northern Uganda: 2015–2024. PLOS Global Public Health. 2026 Jan 1;6(1): e0005800. doi: 10.1371/journal.pgph.0005800
- Greenwood B. Manson Lecture: Meningococcal meningitis in Africa. Trans R Soc Trop Med Hyg. 1999 Jul 1;93(4):341–53. doi:10.1016/S0035-9203(99)90106-2 PubMed PMID: 10674069.
- Meningococcal Meningitis – Africa CDC [Internet]. [cited 2026 Mar 24]. Available from: https://africacdc.org/disease/meningococcal-meningitis/
- Investigation of a Bacterial Meningitis Cluster in a Refugee Settlement, Obongi District, Uganda, March, 2023 – UNIPH [Internet]. [cited 2026 Feb 20]. Available from: https://uniph.go.ug/investigation-of-a-bacterial-meningitis-cluster-in-a-refugee-settlement-obongi-district-uganda-march-2023/?utm
- Cresswell F V., Bangdiwala AS, Bahr NC, Trautner E, Nuwagira E, Ellis J, et al. Tuberculous meningitis diagnosis and outcomes during the xpert MTB/Rif era: A 6.5-year cohort study in Uganda [version 2; referees: 3 approved]. Wellcome Open Res. 2018;3. doi:10.12688/wellcomeopenres.14610.2
- Rajasingham R, Rhein J, Klammer K, Musubire A, Nabeta H, Akampurira A, et al. Epidemiology of meningitis in an HIV-infected Ugandan cohort. Am J Trop Med Hyg. 2015 Feb 1;92(2):274–9. doi:10.4269/ajtmh.14-0452 PubMed PMID: 25385864.
- Mugabi T, Namombwe S, Dai B, Nalintya E, Nsangi LJ, Kabahubya M, et al. Etiology and Outcomes of Meningitis among Adults in Three Ugandan Referral Hospitals, 2018–2023: A Prospective Cohort Study in a High-HIV Endemic Setting. Am J Trop Med Hyg. 2025 Jun 4;112(6):1273–9. doi:10.4269/ajtmh.24-0373 PubMed PMID: 40233735.
- Ellis J, Team on behalf of the AC, Bangdiwala AS, Team on behalf of the AC, Cresswell F V, Team on behalf of the AC, et al. The Changing Epidemiology of HIV-Associated Adult Meningitis, Uganda 2015–2017. Open Forum Infect Dis. 2019 Oct 1;6(10). doi:10.1093/ofid/ofz419
- Okwir M, Link A, Opio B, Okello F, Nakato R, Nabongo B, et al. Poor long-term outcomes despite improved hospital survival for patients with cryptococcal meningitis in rural, Northern Uganda. PLoS One. 2024 May 1;19(5): e0303805. doi: 10.1371/journal.pone.0303805 PubMed PMID: 38771769.
- Skipper CP, Hullsiek KH, Cresswell F V., Tadeo KK, Okirwoth M, Blackstad M, et al. Cytomegalovirus viremia as a risk factor for mortality in HIV-associated cryptococcal and tuberculous meningitis. International Journal of Infectious Diseases. 2022 Sep 1; 122:785–92. doi: 10.1016/j.ijid.2022.07.035 PubMed PMID: 35843498.
- Kambugu A, Meya DB, Rhein J, O’Brien M, Janoff EN, Ronald AR, et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clinical Infectious Diseases. 2008 Jun 1;46(11):1694–701. doi:10.1086/587667 PubMed PMID: 18433339.
- Jarvis JN, Meintjes G, Williams A, Brown Y, Crede T, Harrison TS. Adult meningitis in a setting of high HIV and TB prevalence: Findings from 4961 suspected cases. BMC Infect Dis. 2010 Mar 15;10. doi:10.1186/1471-2334-10-67 PubMed PMID: 20230635.
- Walukaga S, Fieberg A, Musubire A, Tugume L, Ssebambulidde K, Kagimu E, et al. The evolution of HIV-associated cryptococcal meningitis in Uganda from 2010 to 2022. Med Mycol. 2024 Dec 27;63(1):115. doi:10.1093/mmy/myae115 PubMed PMID: 39779301.
- NATIONAL POPULATION AND HOUSING CENSUS 2024 FINAL REPORT VOLUME 1 (MAIN) REPUBLIC OF UGANDA.
- Stadelman AM, Ssebambulidde K, Tugume L, Pastick KA, Hullsiek KH, Lofgren S, et al. Impact of biological sex on cryptococcal meningitis mortality in Uganda and South Africa. Med Mycol. 2021; 59:712–9. doi:10.1093/mmy/myaa108
- Akaishi T, Tarasawa K, Fushimi K, Yaegashi N, Aoki M, Fujimori K. Demographic profiles and risk factors for mortality in acute meningitis: A nationwide population‐based observational study. Acute Medicine & Surgery. 2023 Jan;11(1): e920. doi:10.1002/ams2.920 PubMed PMID: 38162167.
- Hsieh DY, Lai YR, Lien CY, Chang WN, Huang CC, Cheng BC, et al. Sex-based differences in bacterial meningitis in adults: Epidemiology, clinical features, and therapeutic outcomes. J Infect Public Health. 2021 Sep 1;14(9):1218–25. doi: 10.1016/j.jiph.2021.08.018 PubMed PMID: 34438332.
- Liechti FD, Van Ettekoven CN, Brouwer MC, Bijlsma M, Van De Beek D. Sex differences in bacterial meningitis and associations with socioeconomic indicators: a systematic review and meta-analysis with metaregression. BMJ Glob Health. 2025 Apr 30;10(4): e016802. doi:10.1136/bmjgh-2024-016802 PubMed PMID: 40306729.
- Guidelines for the diagnosis, prevention and management of cryptococcal disease in HIV-Infected adults, adolescents and children: supplement to the 2016 Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. 2018;51.
- World Health Organization. DEFEATING MENINGITIS BY 2030 A GLOBAL ROAD MAP [Internet]. 2021 Jun [cited 2026 May 24]. Available from: https://www.who.int/publications/i/item/9789240026407
- World Health Organization. Ensuring effective meningitis surveillance [Internet]. [cited 2026 May 24]. Available from: https://www.who.int/activities/ensuring-effective-meningitis-surveillance