
Uptake of the second dose of measles-rubella vaccine among children aged 18–23 months in Uganda, August, 2024
Sharon Namasambi¹*, Richard Migisha¹, Yasiini Nuwamanya¹, Benon Kwesiga¹, Collins Ankunda3, Pauline Achom1, Nasif Matovu¹, Annet Mary Namusisi¹, Emmanuel Okiror¹ Institutional Affiliation: ¹Uganda Public Health Fellowship Program, Ministry of Health, Kampala, Uganda; 2Department of Community Health and Behavioural Sciences, School of Public Health, Makerere University, Kampala, Uganda; 3Department of Pharmacology, Makerere University, Kampala, Uganda Correspondence*: Email: nabsharon@uniph.go.ug +256772511067
Summary
Background: Uganda introduced the second dose of measles-rubella vaccine (MR2) in 2022 to strengthen protection in the second year of life, but routine coverage has remained low. A national survey was conducted to estimate MR2 coverage and identify factors associated with uptake among children aged 18–23 months in Uganda.
Methods: We conducted a nationally representative, two-stage stratified cluster household survey in Uganda’s four regions. Caregivers of eligible children were interviewed using a structured electronic questionnaire, and MR2 status was verified from vaccination cards. Weighted estimates were calculated, and modified Poisson regression was used to assess factors associated with uptake.
Results: Among 750 children, national MR2 coverage was 32.0% (95% CI: 25.5–38.7), with marked regional differences. Coverage was highest in the Northern region (41.4%) and lowest in the Eastern region (22.0%), while the Western and Central regions recorded 34.5% and 27.6%, respectively. Several factors were associated with MR2 uptake. First-born children were more likely to be vaccinated than children of higher birth order (aPR=1.7; 95% CI: 1.1–2.6; p=0.02), and children in households with two or more eligible children had higher uptake than those in households with only one eligible child (aPR=2.4; 95% CI: 1.4–4.1; p=0.002). In contrast, caregiver-reported adverse events following immunization (aPR=0.4; 95% CI: 0.2–0.7), and dissatisfaction with vaccination services (aPR=0.2; 95% CI: 0.06–0.5) were associated with lower MR2 uptake.
Conclusions: MR2 coverage in Uganda remains far below the level (>95%) needed for measles and rubella elimination. Improving uptake will require stronger second-year-of-life vaccination strategies, better follow-up of eligible children, improved caregiver communication on vaccine safety, and better client experience at vaccination sites.
Background
Although one dose of measles-rubella (MR) vaccine prevents most infections, up to 15% of children may remain susceptible, particularly in high-transmission settings(1,2). To support measles elimination, WHO recommends two MR doses, with MR1 at 9 months and MR2 at 15–18 months, and global targets call for at least 95% coverage with two measles-containing vaccine doses in every district by 2030(3,4). However, despite improvements in MR1 coverage in Uganda, MR2 uptake remains low. Uganda introduced MR2 into the routine immunization schedule in 2022 for children aged 18 months, but HMIS data showed a decline in MR2 coverage from 49% in 2022 to 21% in 2023, while MR1 coverage increased from 83% in 2013 to 93% in 2023(5–7). This widening gap highlights persistent weaknesses in second-year-of-life immunization delivery, including reduced caregiver engagement after infancy, weak defaulter tracking, limited reminders, concerns about adverse events following immunization, socio-cultural influences, regional inequities, inconsistent outreach, and low caregiver awareness of 2YL immunization schedules(8–11). Because determinants of MR2 uptake remain poorly characterized, particularly using behavioural frameworks such as the Behavioural and Social Drivers model, we conducted a cross-sectional household survey among children aged 18–23 months in Uganda during August–September 2024 to estimate MR2 coverage and identify factors associated with uptake.
Methods
We conducted a cross-sectional household survey in August–September 2024 across 15 districts in Uganda’s four regions informed by selected enumeration areas to generate nationally representative estimates and assess regional variation in MR2 uptake. The study included children aged 18–23 months and their primary caregivers who had lived in the selected areas for at least six months; only children with vaccination cards were enrolled to allow objective verification of MR2 status.
A two-stage stratified cluster sampling design was used: 165 enumeration areas were selected proportional to population size from the Uganda Bureau of Statistics sampling frame, after which households were systematically sampled, and one eligible child was randomly selected per household using a lottery method. The minimum sample size was 750 children, based on an assumed MR2 coverage of 30%, 5% margin of error, 95% confidence level, design effect of 2.25, and 10% non-response allowance.
Data were collected using a structured electronic questionnaire in KoboCollect adapted from the WHO vaccination cluster survey manual (12) and informed by the BeSD framework(13). The tool captured socio-demographic, household, health service, and behavioural factors, and was translated into Local languages, back-translated, and pilot-tested before use. Uptake of MR2was the outcome variable. Associations with potential determinants were assessed in Stata version 17 using weighted modified Poisson regression with robust standard errors, accounting for clustering and non-response. Sampling weights were derived as the inverse of the selection probabilities at EA and household levels and were adjusted for non-response.
This study was a secondary analysis of data collected through a national vaccination coverage survey conducted by the Uganda Ministry of Health and partners. The parent survey was administratively cleared by the Ministry of Health, and the U.S. Centers for Disease Control and Prevention determined the activity to be non-research public health practice. Participation was voluntary, written informed consent was obtained from all caregivers before participation, interviews were conducted in private settings, and all data were de-identified and securely stored to protect participant confidentiality.
Results
Characteristics of study participants
A total of 750 children aged 18–23 months and their primary caregivers were included in the study. The median age of children was 20 months (interquartile range [IQR] 19-22 months). Most children (70%; 544) were born in health facilities, and 566 (79%) received vaccinations at static health facility sessions. Public health facilities administered 86% of the vaccinations. Caregivers were predominantly female (93%; 702) and had a median age of 28 years (IQR 24-34). Nearly all (93%; 684) were the parents of the child
National and Regional Measles Rubella 2 vaccine Uptake, Uganda, August 2024
The overall MR2 vaccine coverage was 32.0% (95% CI: 25.5–38.7). Coverage varied by region: Northern (41.4%, 95% CI: 29.6–54.2), Central (27.6%, 95% CI: 19.3–37.7), Western (34.5%, 95% CI: 23.3–47.8), and Eastern Uganda (22.0%, 95% CI: 14.6–31.8).
Factors associated with Measles Rubella 2 Vaccine uptake, Uganda, August 2024
In the adjusted multivariable analysis (Table 1), children whose caregivers were female had a lower prevalence of MR2 uptake compared with male caregivers (aPR=0.4; 95% CI: 0.4–0.9; p=0.01). Uptake was higher among first-born children (aPR=1.7; 95% CI: 1.1–2.6; p=0.02) and second-born children (aPR=1.5; 95% CI: 1.0–2.2; p=0.04), than children of fourth or higher birth order. Children from households with two or more eligible children had higher MR2 uptake than those from households with one eligible child (aPR=2.4; 95% CI: 1.4–4.1; p=0.002). Increasing age modestly increased MR2 uptake (aPR=1.1; 95% CI: 1.0–1.2; p=0.04). A history of adverse events following immunization (AEFIs) was significantly associated with lower MR2 uptake (aPR=0.4; 95% CI: 0.2–0.7; p=0.002), as was caregiver dissatisfaction with vaccination services (aPR=0.2; 95% CI: 0.06–0.5; p=0.001).
Table 1: Factors associated with uptake of the second
dose of measles–rubella vaccine among children
aged 18–23 months, Uganda, August 2024
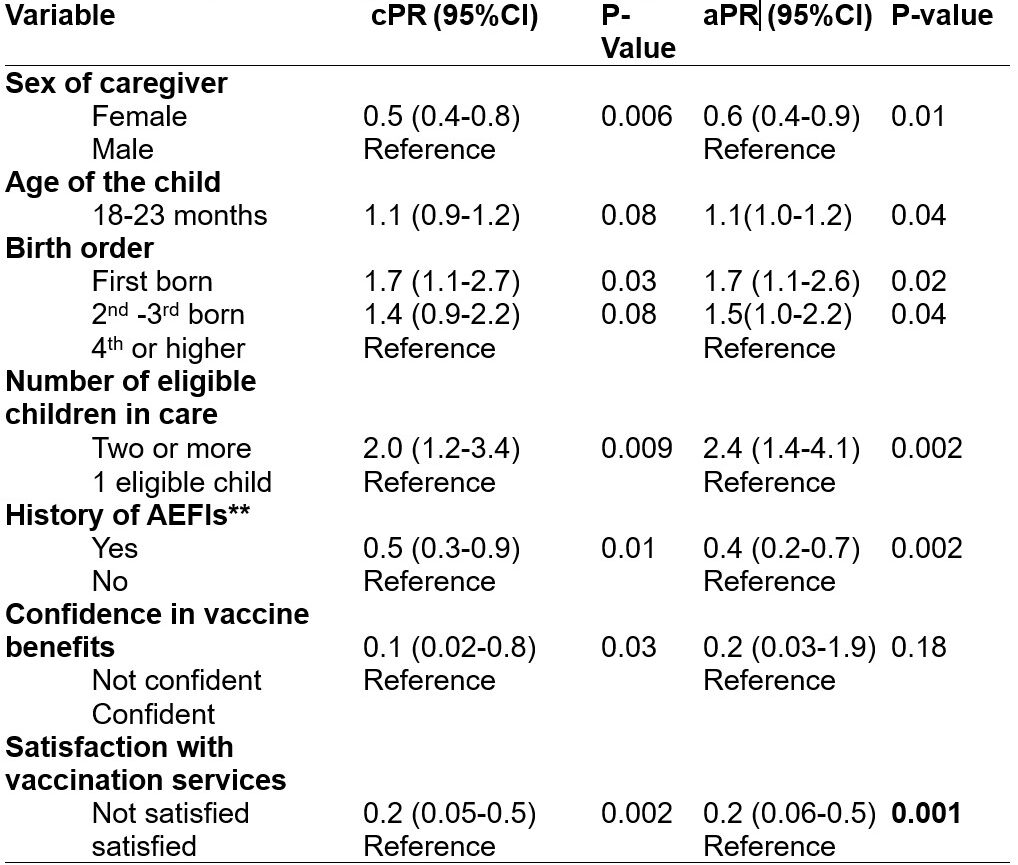
PR = prevalence ratio; CI = confidence interval
aPRs were estimated using modified Poisson regression with robust standard errors
All models accounted for survey weights and clustering at enumeration area level
Discussion
Uptake of the second dose of MR vaccine among children aged 18–23 months in Uganda remains critically low, with coverage far below the level needed to interrupt measles transmission. The large gap between MR1 coverage and MR2 uptake suggests that the health system is able to deliver infant vaccines but is less effective in sustaining vaccination into the second year of life. Regional disparities with lower uptake in the Eastern region and higher uptake in the Northern region, point to persistent inequities in access, outreach, and service delivery. This pattern is consistent with evidence from Uganda and other sub-Saharan African settings showing that missed opportunities, weak follow-up, and limited caregiver awareness continue to undermine completion of later-dose vaccine (7,14,15). Birth order influenced MR2 uptake, with first-born children 70% more likely to receive MR2 than children of fourth and higher birth order. This aligns with global literature showing that later-born children often experience “resource dilution,” in which increased family responsibilities and logistical constraints reduce caregivers’ ability to complete multi-dose schedules (16–18). Additionally, parents may perceive firstborns as more vulnerable, prompting stricter adherence to recommended health behaviours, including immunization. Such challenges are especially pronounced for MR2, which requires a deliberate return visit during the 2YL. Conversely, children from households with multiple eligible children at survey time were more likely to receive MR2, possibly due to more frequent health system contact and synchronized care-seeking during child health days, outreach sessions, or under-five clinics (18–21). Children whose caregivers reported previous AEFIs were 59% less likely to receive MR2, highlighting the powerful influence of real, perceived, or rumor-driven safety concerns on vaccination behaviour. Evidence consistently shows that fear of side effects is one of the strongest predictors of missed or delayed immunization, particularly for second or subsequent doses (18,22–24). Similarly, caregiver dissatisfaction with vaccination services was strongly associated with lower MR2 uptake, reflecting the critical importance of service quality, long waiting times, vaccine stock-outs, poor interpersonal interactions, and inadequate communication, all of which undermine trust and reduce the likelihood of returning for 2YL vaccines(9,11).
Study strength and limitations
This study’s main strength was verification of MR2 status using child health cards, which improved accuracy and reduced recall bias. However, excluding children without cards may have introduced selection bias and limited generalizability. Other limitations included possible recall and social desirability bias in caregiver-reported AEFIs and service satisfaction, the inability of the cross-sectional design to establish causality and the absence of qualitative data to explain caregiver’s experiences and decisions in greater depth.
Conclusion
Uptake of the second dose of measles-rubella vaccine in Uganda remains critically low, with substantial regional variations, highlighting persistent gaps in second-year-of-life immunization despite high MR1 coverage. Key determinants, including caregiver gender, birth order, household composition, prior AEFIs, and service dissatisfaction highlight the multifaceted barriers to timely completion of the second dose. Strengthening 2YL programming may require context-specific, household- and gender-responsive interventions, including enhanced caregiver education and engagement, improved service quality, strengthened AEFI surveillance and risk communication. Addressing these determinants could contribute to reducing immunity gaps, improving completion of the immunization schedule, and supporting progress toward national and global measles and rubella elimination targets.
Conflict of interest
The authors declare no competing interests.
Acknowledgements
We acknowledge the Ministry of Health through the Uganda Expanded Program on Immunization (UNEPI), the Global Alliance for Vaccines and Immunization (GAVI), and the Uganda Public Health Fellowship Program for their technical guidance and funding support. We also thank the Uganda Bureau of Statistics (UBOS) for their commitment and support during this investigation, particularly for providing the master sampling lists of enumeration areas, which were essential for the sampling design and participant selection process.
Authors’ contributions
SN conceptualized the study, led data collection and analysis, and drafted the article. YN, AMN, NM supported data analysis and technical review of the draft article .PA, NM, AMN, CA, and EOO supported revision of the first article draft. RM, YN, NM, and AMN contributed to tool development, field coordination, and data quality assurance. RM, BK, CA and YN provided technical input during the study design and data interpretation. YN, BK and RM supervised the study and reviewed the article for critical intellectual content. All authors read and approved the final article.
Copyright
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Orenstein WA, Cairns L, Hinman A, Nkowane B, Olivé JM, Reingold AL. Measles and Rubella Global Strategic Plan 2012–2020 midterm review report: Background and summary. Vaccine. 2018 Jan 11;36: A35–42. doi: 10.1016/j.vaccine.2017.10.065
- Minta AA, Ferrari M, Antoni S, Lambert B, Sayi TS, Hsu CH, et al. Progress Toward Measles Elimination — Worldwide, 2000–2023. Vol. 73. 2024;73(45).
- World Health Organisation. Immunization agenda 2030: A global strategy to leave no one behind. Vaccine. 2024 Apr 8;42: S5–14. doi: 10.1016/j.vaccine.2022.11.042
- WHO. WHO. Reaching every child in the second year of life: a global priority. 2022. WHO; 2022.
- Ministry of Health. NIPR Comprehensive Report v1.2 Revised 30Jun2021-EPI COV. Ministry of Health; 2021.
- Ministry of Health. Annual Health Sector Performance Report FY 2023_24. Ministry of Health; 2023.
- Uganda Bureau of Statistics. Uganda Demographic and Health Survey 2022. 2022. UDHS-2022-Report. Ministry of Health; 2022.
- Favin M, Steinglass R, Fields R, Banerjee K, Sawhney M. Why children are not vaccinated: a review of the grey literature. International Health. 2012 Dec 1;4(4):229–38. doi: 10.1016/j.inhe.2012.07.004
- Rainey JJ, Watkins M, Ryman TK, Sandhu P, Bo A, Banerjee K. Reasons related to non-vaccination and under-vaccination of children in low- and middle-income countries: Findings from a systematic review of the published literature, 1999–2009. Vaccine. 2011 Oct 26;29(46):8215–21. doi: 10.1016/j.vaccine.2011.08.096
- Mbengue MAS, Sarr M, Faye A, Badiane O, Camara FBN, Mboup S, et al. Determinants of complete immunization among senegalese children aged 12–23 months: evidence from the demographic and health survey. BMC Public Health. 2017 Jul 6;17(1):630. doi:10.1186/s12889-017-4493-3
- Topher B, Margaret KM, Eliphas G. Perceptions of caregivers on immunization in Ntungamo district, Uganda. Int J Community Med Public Health. 2021 Nov 24;8(12):5729. doi:10.18203/2394-6040.ijcmph20214559
- World Health Organization. World Health Organization Vaccination Coverage Cluster Surveys: Reference Manual [Internet]. 2022 [cited 2025 Oct 1]. Available from: https://www.who.int/publications/i/item/WHO-IVB-18.09
- World Health Organisation. Behavioural and Social Drivers of Vaccination: Tools and Practical Guidance for Achieving High Uptake. 1st ed. Geneva: World Health Organization; 2022. 1 p.
- Okello G, Izudi J, Ampeire I, Nghania F, Dochez C, Hens N. Two decades of regional trends in vaccination completion and coverage among children aged 12-23 months: an analysis of the Uganda Demographic Health Survey data from 1995 to 2016. BMC Health Serv Res. 2022 Jan 7;22(1):40. doi:10.1186/s12913-021-07443-8
- Uthman OA, Sambala EZ, Adamu AA, Ndwandwe D, Wiyeh AB, Olukade T, et al. Does it really matter where you live? A multilevel analysis of factors associated with missed opportunities for vaccination in sub-Saharan Africa. Human vaccines & immunotherapeutics. 2018;14(10):2397–404.
- Costa FS, Silva LAN, Cata-Preta BO, Santos TM, Ferreira LZ, Mengistu T, et al. Child immunization status according to number of siblings and birth order in 85 low- and middle-income countries: a cross-sectional study. eClinicalMedicine. 2024 May 1;71. doi: 10.1016/j.eclinm.2024.102547 PubMed PMID: 38524919.
- Tugumisirize F, K.Tumwine J, Mworoza EA. Missed opportunities and caretaker constraints to childhood vaccination in rural areas of Uganda. E Af Med Jrnl. 2002 Jul 1;79(7):347–54. doi:10.4314/eamj.v79i7.8837
- Bangura JB, Xiao S, Qiu D, Ouyang F, Chen L. Barriers to childhood immunization in sub-Saharan Africa: A systematic review. BMC Public Health. 2020 Jul 14;20(1):1108. doi:10.1186/s12889-020-09169-4
- Adisu MA. Timeliness of the second dose of measles-containing vaccine uptake and its determinants among children aged 24–36 months in Gondar City, Northwest Ethiopia, 2023: Community-based cross-sectional study design. Journal of Virus Eradication. 2025 Jun 1;11(2):100594. doi: 10.1016/j.jve.2025.100594
- Costa F, Neves Silva L, Cata-Preta B, Santos T, Ferreira L, Mengistu T, et al. Child immunization status according to number of siblings and birth order in 85 low- and middle-income countries: a cross-sectional study. EClinicalMedicine. 2024 Mar 18;71. doi:10.1016/j.eclinm.2024.102547
- Galadima AN, Zulkefli NAM, Said SM, Ahmad N. Factors influencing childhood immunisation uptake in Africa: a systematic review. BMC Public Health. 2021 Jul 28;21(1):1475. doi:10.1186/s12889-021-11466-5
- Nsubuga F, Alfred D, Gyasi SO, Ampeire I, Kabwama SN. Low reporting of adverse events following immunization, during a Measles-Rubella catchup and Polio mass vaccination campaign in Uganda; 2019 [Internet]. In Review; 2022 [cited 2025 Nov 20]. Available from: https://www.researchsquare.com/article/rs-1286703/v1 doi:10.21203/rs.3.rs-1286703/v1
- Gopalan RB, Babu BV, Sarma S K, John RP. Adverse Effects Following Immunisation and Vaccine Hesitancy: A Qualitative Study in a South Indian District. Drug Healthc Patient Saf. 2025 Jun 16;17:145–56. doi:10.2147/DHPS.S515064 PubMed PMID: 40548049; PubMed Central PMCID: PMC12180458.
- Unfried K, Priebe J. Vaccine hesitancy and trust in sub-Saharan Africa. Sci Rep. 2024 May 13;14(1):10860. doi:10.1038/s41598-024-61205-0
Comments are closed.