
Evaluation of the Laboratory Pillar Response during the Sudan Virus Disease Outbreak in Uganda, 2025: An After-Action Review
Authors: Caroline Musubika 1,2 *, Joshua kayiwa 3 , Alisen Ayitewala 3 , Isaac Ssewanyana 3 , Samuel Gidudu 1 , Godfrey Ekuka 5 , Andrew Nsawotebba 3 , Valeria Nakintu 3 , Vivian Nakawesa 1 , Martha Nakaye 1, Diana Namaya 4 , Daniel Namanya 6 , Ibrahim Mugerwa 3 , Rebecca Kakudde 7 , Morgan Ottita 8 , Bridget Ainembabazi 1 , Roger Micheal Eilu 8 , Thomas Nsibambi 1 , Jonathan Ntale 3 , and Susan Ndidde Nabadda 3 Institutional affiliations: 1 Uganda National Institute of Public Health, Ministry of Health, Kampala, Uganda, 2 Makerere University Biomedical Research Centre, 3 National Health Laboratory and Diagnostics Services, Ministry of Health, Kampala, Uganda, 4 Uganda Virus Research Institute, Ministry of Health, Entebbe, Uganda, 5 Department of Integrated Epidemiology Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda, 6 Kyegegwa District local government, Kyegegwa, Uganda, 7 Baylor Foundation, Kampala, Uganda, 8 Infectious Diseases Institute, Kampala, Uganda *Correspondence: Email: musubikacarol@uniph.go; +256 784 752853
Summary
Background: Following the containment of the 2025 Sudan Virus Disease (SVD) outbreak in Uganda, the Ministry of Health conducted an After-Action Review (AAR) to document lessons across multiple response pillars as required by the International Health Regulations Monitoring and Evaluation Frame work. This paper evaluates the laboratory pillar and #39s performance in containing the outbreak.
Methods: Using a working group AAR format, we conducted facilitated exercises to evaluate the response. We reviewed pre-existing capacities across four domains: plans, coordination, resources, and preparedness activities to establish a baseline. We reconstructed the response timeline against an epidemiological curve and cross-validated milestones with other pillars. Performance gaps were identified by contrasting planned and actual outcomes, and the five whys technique was applied to determine the root causes of the identified challenges.
Results: Fifteen professionals from national and sub-national levels participated. Pre-response enablers included the existence of the National laboratory guidelines for preparedness and response to public health emergencies, the Uganda National Health Laboratory Hub and sample network, National health laboratory policy, the Ebola 2022 response plan, the national laboratory budget, the national laboratory pillar, the Laboratory Leadership Program, the One Health platform, reference and mobile laboratories. The referral network confirmed the case within 72 hours; however, analysis revealed delays in the deployment of mobile laboratories and incomplete investigation forms. Key strengths included emergency information systems and biosafety protocols, while key constraints were limited funding, low district-level involvement, and conflicting guidance on result dissemination. Root causes were traced to an inactive electronic logistics system and lack of pre-positioned supplies at the district level.
Conclusion: The laboratory pillar demonstrated functional preparedness and response capabilities. To ensure resilience against future high-consequence threats, we recommend standardizing communication protocols and strengthening emergency logistic systems.
Background
On 30 th January 2025, the Uganda Ministry of Health confirmed the eighth Ebola virus disease outbreak caused by Sudan Virus (SDV). The outbreak affected Kampala, Wakiso, and Mbale and prompted mapping of seven additional highrisk 2 districts (1) . It resulted in 14 cases and four deaths (case fatality rate 28.5%) and was declared over on 25 April 2025, 42 days after the last patient was discharged from hospital. Ebola outbreaks require rapid detection, timely laboratory confirmation, effective case management, contact tracing, infection prevention and control, risk communication, and coordinated response across multiple pillars. After such an event, systematically reviewing the response is essential to identify what worked well, what did not work well, and what corrective actions are needed to strengthen preparedness and response for future outbreaks (2) . After Action Review (AAR) is one of the components of the International Health Regulations (IHR) Monitoring and Evaluation Framework, alongside annual reporting on International Health Regulation (IHR) capacities, Joint External Evaluation, and simulation exercises (3) . The AAR is a qualitative assessment of the actions taken in response to a public health event of concern (2) . It enables countries to assess the functionality of public health systems after an emergency, document best practices, identify gaps, and define immediate, medium-term, and long-term actions for strengthening IHR core capacities (3, 4) . Following the 2025 SVD outbreak, the Ministry of Health conducted an AAR in June 2025 to review actions undertaken during the preparedness, detection, and response phases of the outbreak. The review assessed performance across multiple response pillars, documented lessons learned, and identified priority corrective actions to strengthen Uganda’s readiness for future Ebola outbreaks and other public health emergencies. The laboratory pillar is central to Ebola outbreak detection and response because timely and accurate testing guides case confirmation, isolation, contact tracing, clinical management, and declaration of outbreak control milestones. Delays or gaps in laboratory preparedness and response can affect the speed and quality of outbreak control activities (5) . We assessed the laboratory pillar’s preparedness and response to the 2025 Sudan virus disease outbreak in Uganda to identify pre-existing capacities, response performance, root causes of challenges, lessons learned, and priority actions for strengthening future Ebola diagnostic preparedness
and response.
Methods
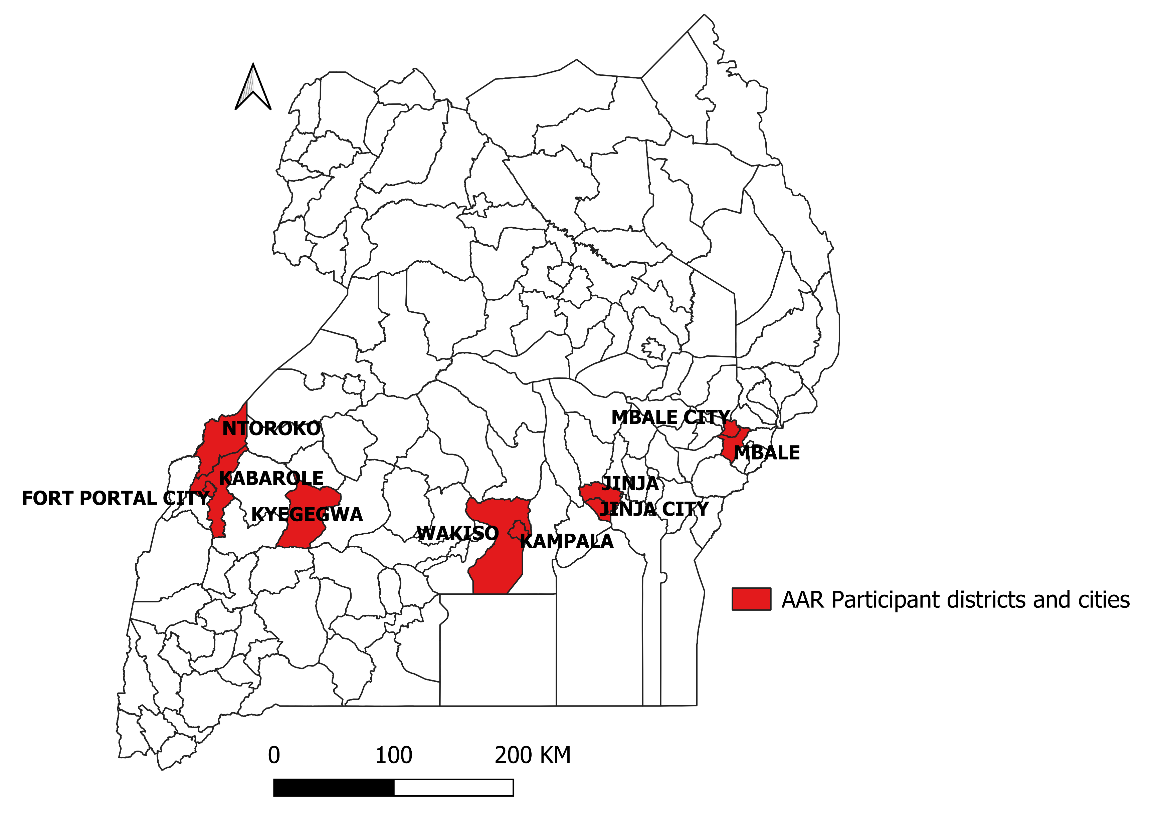
A three-day After-Action Review meeting was convened at Imperial Royale Hotel, Kampala, Uganda. Using a working group AAR format, facilitated exercises and plenary sessions were conducted to evaluate the response (2) . The discussions were led by a facilitator and documented by a note-taker proficient in laboratory functions. The group discussion comprised fifteen laboratory professionals from national and sub-national levels in the seven high-risk districts and three cities, including Mbale District and Mbale City, Kabarole District and Fort Portal City, Kyegegwa, Ntoroko, Jinja District and Jinja City, Wakiso, and Kampala City (Figure 1).
Preparedness assessment to Sudan Virus Disease outbreak
We reviewed per-existing capacities across four domains: plans, coordination, resources, and preparedness activities to establish a baseline. We used Post-it sticky notes and compiled the notes in a table on a flip-chart. We then reviewed the notes and discussed the findings during the plenary session.
Response assessment to Sudan Virus Disease outbreak
We assessed the laboratory response timeline, and outcomes by reconstructing the response timeline against an epidemiological curve and compared milestones with other pillars. Performance gaps were identified by contrasting planned against actual outcomes, bottlenecks and enablers of timely performance were identified and the five whys technique was applied to determine root causes of identified challenges, improvement actions were proposed to address bottlenecks and improve future laboratory performance.
Results
Preparedness assessment findings
Fifteen professionals from national and sub-national participated. Pr-response enablers included the existence of the National laboratory guidelines for preparedness and response to public health emergencies, Uganda national health laboratory hub and sample network, National health laboratory policy, Ebola 2022 response plan, National laboratory budget, National laboratory pillar, Laboratory leadership program, One health platform, and the existence of Reference and mobile laboratories.
Response assessment findings
The referral network confirmed the case within 72 hours. However, analysis revealed delays in deployment of mobile laboratories and incomplete investigation forms. Key strengths included availability of emergency information systems and biosafety protocols, while key constraints included limited funding, low district-level involvement, and conflicting result-dissemination guidance. Root causes were traced to an inactive electronic logistics system and lack of pre-positioned supplies at the district level.
Discussion
The preparedness and response strategies for laboratory Ebola response was informed by the availability and reference to pre-existing preparedness frameworks including national preparedness plans, policies and response structures such as reference and mobile laboratories and laboratory hub and sample network. Well defined frameworks such as sample collection protocols and sample referral networks ensured rapid turnaround time of 72 hours. Despite the progress, we learnt that weaknesses in electronic logistic system can disrupt supply chain performance (6) while a lack of pre-positioned supplies at the district level, limited funding, delays in mobile laboratory deployment, low district-level involvement, conflicting result-dissemination guidance can greatly disrupt emergency response operations. By embracing lessons learned and addressing challenges, we can strengthen our national laboratory defenses and work across boundaries to protect public health against any emerging infectious disease.
Limitations: The information collected was based on self-reports, this could have been biased among the laboratory workers who may have been expected to take “best practice” actions but did not. However, this bias was minimized during the debrief sessions, during which laboratory workers were assured of confidentiality in participation. Additionally, the bias was reduced by triangulating information from other staff and other reports as much as possible.
Conclusion: The laboratory pillar demonstrated functional preparedness and response capabilities. Its response depended on the availability of pre-existing preparedness frameworks to support staff, sample referral networks, and coordination mechanisms. However, limited funding and lack of pre-positioned supplies disrupted critical laboratory functions, undermining the speed and efficiency of the response. The conflicting result-dissemination guidance disrupted data flow which limited the ability of the responders to make timely decisions and public trust in the outbreak response process was undermined.
Recommendation: To ensure resilience against future high-consequence threats, we recommend standardizing communication protocols and strengthening emergency logistic systems.
Conflict of Interest: The authors declare no conflict of interest
Author contribution: CM led the study conceptualization, data collection, analysis, and article drafting. VN, MN, DN, DN, IM, RK, MO, BA, RMO, TN, JN contributed to data collection and writing. SG provided supervision, validation, and article review. All authors read and approved the final bulletin.
Acknowledgements: The authors appreciate the Ministry of Health for funding the After- Action Review meeting that contributed to the data collection process.
Copyrighting and licensing: All material in the Uganda Public Health Bulletin is in the public domain and may be used and printed without permission. However, citation as to source is appreciated. Any article can be reprinted or republished. If cited as a reprint, it should be referenced in the original form.
References
- GLANCE A. Ebola Outbreak Caused by Sudan virus in Uganda. 2025.
- Organization WH. Guidance for after action review (AAR). World Health Organization; 2019.
- Organization WH. Technical Framework in Support to IHR (2005) Monitoring and Evaluation. Joint External Evaluation Tool. 2018.
- Njuguna C, Vandi M, Liyosi E, Githuku J, Squire JS, Njeru I, et al. After action review of the response to an outbreak of Lassa fever in Sierra Leone, 2019: Best practices and lessons learnt. PLOS Neglected Tropical Diseases. 2022;16(10):e0010755.
- Schuh AJ, Kyondo J, Graziano J, Balinandi S, Kainulainen MH, Tumusiime A, et al. Rapid establishment of a frontline field laboratory in response to an imported outbreak of Ebola virus disease in western Uganda, June 2019. PLoS Neglected Tropical Diseases. 2021;15(12):e0009967.
- Wasswa JH, Oundo H, Oteba MO, Komakech H, Ochola I, Mwebaze S, et al. Leveraging electronic logistics management information systems to enhance and optimize supply chain response during public health emergencies: lessons from COVID-19 response in Uganda. Journal of Pharmaceutical Policy and Practice. 2023;16(1):6.