
Voluntary Male Medical Circumcision Service Uptake among Men over 20 Years of Age during Flexi and Regular Hours, Central Uganda, 2018-2019
Authors: Sarah Elayeete1*, Atuhaire Immaculate1, Gerald Pande2, Benon Kwesiga1, Steven Kabwama1, Alex R. Ario1,2 Institutional affiliations 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Ministry of Health, Kampala, Uganda Correspondence*: Email: selayeete@musph.ac.ug, Tel:+256-782-948-872
Summary
Background: Voluntary male medical circumcision (VMMC) in Uganda was only offered during regular hours (8:00am to 5:00pm and only week days) from 2010-2017. However, VMMC uptake among men aged 20+ years was low. To scale uptake VMMC among men 20+ years, ‘flexi-hour clinics’ were rolled out in Kampala and Wakiso districts in 2018. Flexi-hour clinics expanded the hours during which VMMC was offered to after 5:00pm on weekdays, including weekends, and holidays. However, no study has compared VMMC service use in flexi and regular hour clinics. We described and compared patients’ profiles who received VMMC during flexi and regular hours in four facilities. We also assessed trends in VMMC service use to determine ways to improve targeted uptake of VMMC.
Methods: Demographic data were retrieved from the electronic medical records for clients aged 20+ years in both flexi (n=1,984) and regular hour (n=5,077) clinics during 2018 to 2019. Where individual level information was missing from the electronic database, we reviewed medical registers to complete the data. We described men who received VMMC during flexi or regular hours using frequencies and percentages. We compared demographic characteristics of men receiving VMMC during flexi or regular hours as a proportion of all men who received VMMC service from 2018-2019 using a two-sample t-test. To assess trends in VMMC use over time, we assessed overall and quarterly changes in VMMC use at each clinic as a proportion of all clients accessing VMMC service over time and in each quarter.
Results: A total of 7,061 men received VMMC services during flexi and regular hour clinics. Among all men who received VMMC, 1,984 (28%) used flexi-hours. Of the 1,984 men who got VMMC service during flexi hours, 940 (47%) were married or cohabiting, 1,267 (64%) were aged between 20-29 years, and 1,785 (90%) were employed. A higher proportion that used VMMC during flexi hour verses regular hour were married/cohabiting (47% vs 44%; p=0.003), had no education (26% vs 22%; p=0.0004), and came from Eastern region (17% vs 13%; p=<0.0001). Men receiving VMMC during flexi hours were non-significantly older than men receiving VMMC service during regular hours (median age 27 vs 26 years, p=0.37). Overall, there was an overall decline in VMMC uptake by 6% during regular hours and 30% decline during flexi hours.
Conclusion: More than a quarter of men aged 20+ received VMMC services during flexi-hours. There were modest demographic differences between men using flexi-hours versus regular hours. Expanding flexi-hour VMMC clinics to other parts of the country may be beneficial in improving uptake.
Introduction
Voluntary medical male circumcision (VMMC) is the complete surgical removal of the foreskin as a one-time primary prevention intervention that reduces the risk of heterosexual transmission of HIV from a female partner to the male by approximately 60 percent (1-4). It offers men substantial lifelong partial protection against the acquisition of HIV and a number of other sexually transmitted diseases (1-4). As a result, the World Health Organization (WHO) and Joint United Nations Programme on HIV/AIDS (UNAIDS) recommended VMMC as a new HIV prevention intervention among men in regions with high HIV prevalence and low rates of male circumcision (5).
Based on WHO recommendations, the Uganda Ministry of Health adopted VMMC policy in 2010 as part of HIV prevention package (6) with a goal of achieving 80% circumcision coverage among men aged 15 to 49 years by 2020 (7). Initially, VMMC was only offered during regular business hours (9 am to 5 pm Monday through Friday). However, in 2015, the circumcision prevalence rate among men aged 30 years or older remained generally low (26%), compared to 69% among men under 20 years of age.
In order to scale up uptake of VMMC services among men 20+ years, ‘flexi-hour clinics’ were rolled out in Kampala and Wakiso districts in 2018. Flexi-hour clinics occur at the same sites as regular hour clinics. However, they are generally operating from 5 pm to 10:00 pm on weekdays and weekends. On the other hand, regular-hour clinics typically operate from 8:00am to 5:00pm and only weekdays. As a result, flexi-hour clinics typically operate 42 hours per week while regular clinics generally operate 50 hours per week.
Although flexi-hour clinics had been implemented since 2018, no evaluation had assessed VMMC service uptake and how men getting circumcised during flexi-hours compared to those who get circumcised during regular hours across demographic characteristics such as age, marital status, religion, occupation, place of residence, tribe, and education level. We described and compared’ profiles of men who received VMMC during flexi and regular hours at four clinics in Kampala and Wakiso districts. We also assessed trends in VMMC service use to determine ways to improve targeted uptake of VMMC.
Methods
Study setting and design
We conducted a secondary data analysis of individual level data collected from only health facilities offering VMMC services during both flexi and regular hours for the period 2018 to 2019. The facilities included: Kisenyi, Kajjansi, Kiira and Wakiso Health Center four (HC IVs). We considered all the data generated during 2018-2019.
Study variables, data source, and data collection
Data on demographic characteristic (Age, marital status, employment status, education level, religion and region of origin), site type (flexi or regular), time of circumcision, and underlying health conditions were retrieved from the electronic database (electronic medical records) for men attending clinics during both flexi and regular hours.
Where individual level information was missing from the electronic database, health facilities were visited and VMMC medical registers were reviewed and individual data on demographic characteristics, VMMC modality, time of circumcision, and underlying health conditions were abstracted.
We defined VMMC service use as the number of eligible men who voluntarily underwent VMMC during flexi or regular-hours in the study period. We defined flexi hours as 5:00pm on wards, weekends, holidays, and through mobile services exclusively at the convenience of the clients. While regular hours were 8:00am to 5:00pm and from Monday to Friday.
Data management and analysis
We analysed data using Stata version 14. We described men who underwent VMMC during flexi and regular hours by their demographic characteristics using frequencies and percentages. Demographic characteristics of men who received VMMC during flexi were compared to the demographics of men who received during regular hours as a proportion of all men who received VMMC from 2018-2019 using a two-sample t-test. To assess for trends in VMMC use, changes in overall, and quarterly VMMC use at each clinic was assessed as a proportion of all clients accessing VMMC service over time and during each quarter.
Ethical considerations
We utilized VMMC surveillance data with no identifying information. We abstracted individual clients VMMC data with permission from facility administrators. In addition, the Office of the Associate Director for Science, U.S. Centres for Disease Control and Prevention, determined this project as a non-human subject’s research that will be in response to a public health problem with the primary intent of public health practice (epidemic disease control).
Results
Socio–demographic characteristics of men aged <20 who received Voluntary medical male circumcision during flexi and regular hours, Uganda, 2018-2019
A total of 7,061 men under went VMMC during both flexi and regular hours. Of those, 1,984 (28%) of the men used VMMC during flexi hours and 5,077 (72%) of the men used VMMC service during regular hours (Table 1).
Among 1,984 men who received VMMC service during flexi hours, 940 (47%) were married or cohabiting, 1,259 (63%) had attained secondary education, and 1,785 (90%) were employed. The median age of men who underwent VMMC during flexi hours was 27 years. Among 5,077 men who received VMMC during regular hours, 2,235 (44%) were married, 3,374 (66%) had attained secondary education and 4,531 (89%) were employed. The median age of men who received VMMC during regular hours was 26 years (Table 1)
Table 1: Socio-demographic characteristics of men who received voluntary medical male circumcision service during flexi or regular hours Central Uganda, 2018-2019
| Characteristics | Reported VMMC Clinic | ||||
| Total | Flexi-hour | Regular hour | |||
| N | n (col%) | n (col%) | |||
| Overall | 7061 | 1984 | 5077 | ||
| Age (Median age) | 27 | 26 | |||
| Age in complete years | |||||
| 20-29 | 4556 | 1267 | (64) | 3289 | (65) |
| 30-39 | 1862 | 543 | (27) | 1319 | (26) |
| 40-49 | 515 | 138 | (7) | 377 | (7) |
| 50 + | 128 | 36 | (2) | 92 | (2) |
| Marital status | |||||
| Divorced/separated | 40 | 18 | (1) | 22 | (0) |
| Married/cohabiting | 3175 | 940 | (47) | 2235 | (44) |
| Single | 3846 | 1026 | (52) | 2820 | (56) |
| Level of education | |||||
| None/pre-primary | 1633 | 511 | (26) | 1122 | (22) |
| Secondary | 4633 | 1259 | (63) | 3374 | (66) |
| Tertiary | 795 | 214 | (11) | 581 | (11) |
| Employment status | |||||
| Unemployed | 745 | 199 | (10) | 546 | (11) |
| Employed | 6316 | 1785 | (90) | 4531 | (89) |
| Religion | |||||
| Muslim | 193 | 60 | (3) | 133 | (3) |
| Anglican | 2518 | 722 | (36) | 1796 | (35) |
| Catholic | 3208 | 856 | (43) | 2352 | (46) |
| Pentecostal/others | 1142 | 346 | (17) | 796 | (16) |
| Region | |||||
| Northern | 412 | 154 | (8) | 258 | (5) |
| Central | 3928 | 995 | (50) | 2933 | (58) |
| Eastern | 973 | 334 | (17) | 639 | (13) |
| Western | 1748 | 501 | (25) | 1247 | (25) |
Comparison of demographic characteristics of men who received VMMC service during flexi and regular hours, Central Uganda, 2018-2019
Among all men who received VMMC services, a higher proportion that used them during flexi hours vs regular hours were married or cohabiting (47% vs. 44%, p=0.003), had no education (26% vs 22%, p=0.0004), and came from Eastern region (17% vs 13%, p=<0.0001)
(Table 2).
A lower proportion of men who received VMMC services during flexi hours vs regular hours came from Central Region (50% vs 58%, p=<0.0001).
In addition, men who underwent VMMC during flexi hours were non-significantly older than men who underwent VMMC during regular hours (median age 27 years vs 26 years, p=0.37) (Table 2)
Table 2: Comparison of demographic characteristics of men who received VMMC during flexi and regular hours, Central Uganda, 2018-2019
| Characteristics | Reported VMMC Clinic | |||||
| Total | Flexi-hour | Regular hour | P-Value | |||
| N | n (col%) | n (col%) | ||||
| Overall | 7061 | 1984 | 5077 | |||
| Age (Median age) | 27 | 26 | 0.37 | |||
| Age in complete years | ||||||
| 20-29 | 4556 | 1267 | (64) | 3289 | (65) | 0.44 |
| 30-39 | 1862 | 543 | (27) | 1319 | (26) | 0.39 |
| 40-49 | 515 | 138 | (7) | 377 | (7) | 1.00 |
| 50 + | 128 | 36 | (2) | 92 | (2) | 1.00 |
| Marital status | ||||||
| Divorced/separated | 40 | 18 | (1) | 22 | (0) | <0.0001 |
| Married/cohabiting | 3175 | 940 | (47) | 2235 | (44) | 0.003 |
| Single | 3846 | 1026 | (52) | 2820 | (56) | <0.0001 |
| Level of education | ||||||
| None/pre-primary | 1633 | 511 | (26) | 1122 | (22) | 0.0004 |
| Secondary | 4633 | 1259 | (63) | 3374 | (66) | 0.02 |
| Tertiary | 795 | 214 | (11) | 581 | (11) | 1.00 |
| Employment status | ||||||
| Unemployed | 745 | 199 | (10) | 546 | (11) | 0.22 |
| Employed | 6316 | 1785 | (90) | 4531 | (89) | 0.22 |
| Religion | ||||||
| Muslim | 193 | 60 | (3) | 133 | (3) | 1.00 |
| Anglican | 2518 | 722 | (36) | 1796 | (35) | 0.42 |
| Catholic | 3208 | 856 | (43) | 2352 | (46) | 0.02 |
| Pentecostal/others | 1142 | 346 | (17) | 796 | (16) | 0.31 |
| Region | ||||||
| Northern | 412 | 154 | (8) | 258 | (5) | <0.0001 |
| Central | 3928 | 995 | (50) | 2933 | (58) | <0.0001 |
| Eastern | 973 | 334 | (17) | 639 | (13) | <0.0001 |
| Western | 1748 | 501 | (25) | 1247 | (25) | 1.00 |
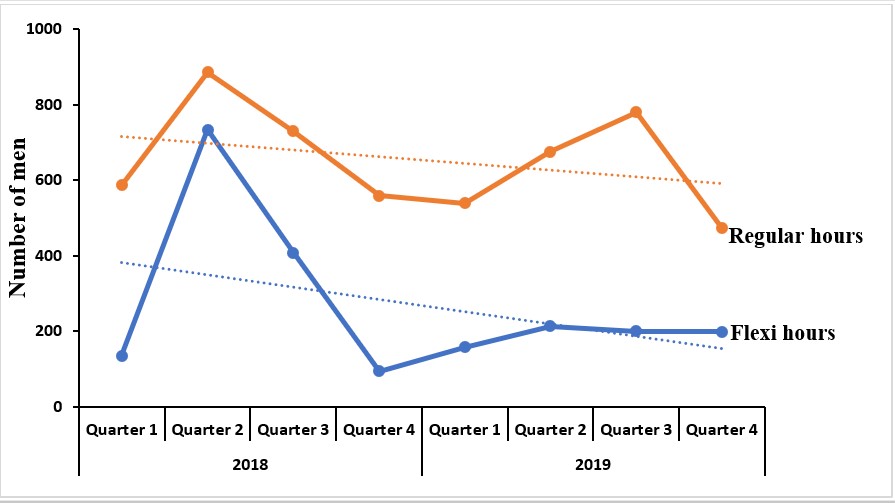
Trends in voluntary male medical circumcision uptake among men aged 20 and above during flexi and regular hours, Uganda, 2018-2019
Overall, from 2018-2019, VMMC uptake during regular hours decreased by 6% while VMMC uptake during flexi-hours decreased by 30%. We observed an increase in the number of men who received VMMC service from the first quarter through the second quarter of 2018 during both regular and during flexi hours.
There was a 30% increase in VMMC service uptake during flexi hours and a 50% increase in regular hours between the first and second quarter of 2018 (Figure 1). This was followed by a general decline during the following quarters for both clinics.
Table 3: Overall trends in VMMC service uptake during flexi and regular hours, Central Uganda, 2018-2019
| Service hours | Total | 2018 | 2019 | Reduction rate (%) | P-Value |
| Flexi hours | 1984 | 1290 | 694 | 30 | <0.0001 |
| Static hours | 5077 | 2692 | 2385 | 6 | <0.0001 |
Figure 1: Trends in VMMC service uptake during flexi and regular hour clinics, Central Uganda, 2018-2019
Discussion
Understanding the use of VMMC during flexi- hours and the types of clients who use flexi- vs regular hours for VMMC is important in ensuring that needs are being met for VMMC for the public. We found that men mostly use VMMC service during regular hours than flexi hours.
There was no significant age difference between men who received VMMC during flexi hours compared to men who received VMMC during regular hours. The men who received VMMC during flexi hours were more likely to be married/cohabiting than men who received VMMC during regular hours. In addition, men who received VMMC during flexi hours were more likely from Eastern regions than men who received VMMC during regular hours.
In Uganda, compared to regular hour clinics, flexi hour clinics were rolled out barely two years from the evaluation period. The 28% reported usage of VMMC service among men aged 20+0 years during flexi hour clinics indicates that, once community-based services are closer or to the convenience of the consumers, they are easily used (8), and may also reflect the time it takes men exposed to the service to decide to pursue VMMC service and use it.
A qualitative study of behaviour change pathways to VMMC in Zimbabwe highlighted the dynamic nature of demand for VMMC, which involves a man’s progression through multiple stages of change over time (9). In addition, a scale up program of VMMC service uptake reached more clients three years post-intervention period compared to the proportion of clients reached the year immediately following program implementation (10).
A study conducted in Tanzania showed that, periodic mobile VMMC service delivery and interpersonal motivational advisors/mentors were promising strategies for promoting VMMC uptake among older clients aged 20 years or older, compared with routine services (11). In addition, a study on the influence of service delivery on age found that the proportions of males within the age group 20–24 years accessing VMMC services during mobile service were significantly higher than those accessing routine services (12).
In contrast, we found no significant age difference between men who received VMMC during flexi hours and men who received VMMC during regular hours, with more men within age group 20-29 years receiving VMMC service during both regular and flexi hours. The big turn up for VMMC among men aged 20-29 years during both regular and flexi hour clinics could be attributed to the fact that youth are very adventurous in trying out new things (13). Although our study did not explore older males concerns in regard to undergoing VMMC during flexi hours, it could also be that the VMMC messages are more appealing to the youth than the older men Married men were more likely to undergo VMMC during flexi hours.
Although this study did not explore men’s perspectives on the choice of sites, one possible explanation for this, is that married men often perceive themselves to be at higher risk of getting infected with HIV due to exposure to frequent unprotected sex with their spouses; hence, wanting circumcision as an HIV prevention strategy (14).
Another possible explanation is that women always influence their male partners decisions of the method and where to undergo circumcision (15, 16). In addition, married men believed that VMMC protects their sexual partners from the risk of Human Papilloma Virus (HPV) associated with cancer of the cervix (16, 17) and this could be a driver to undergoing VMMC during flexi hours.
While it has been suggested earlier that men’s perception of risk of getting infected with HIV may play a role in men’s willingness to undergo VMMC, it is not clear whether the same explanation may apply for the willingness of men from some regions undergoing VMMC
during flexi hours. We found that men from Eastern region were more likely to undergo VMMC during flexi hours than during regular hours. It is possible that the demand to undergo VMMC during flexi hours for men from this region could be associated to the role of social and cultural identity (21) on their knowledge and decisions on whether or not they would adopt the intervention. Men from regions with knowledge of the practice of both traditional and medical circumcision tended to perceive circumcision positively and not stigmatized (22).
Study limitations
We acknowledge the following limitations in line with the study. Firstly, the quantitative nature of the study while using only demographic variables without individual perspectives and environmental factors didn’t allow in depth exploration of knowledge and perceptions as well as attitudes of men towards undergoing VMMC during flexi or regular hours.
Conclusion
We found that the demographic profile of men who received VMMC during flexi hours differed from men who received VMMC during regular hours. Flexi hours are convenient for particular groups of people and should therefore be encouraged. We recommend an in-depth-qualitative study to understand the declining trends of VMMC service use in both flexi and regular hour clinics.
Ethical Considerations
We utilized VMMC surveillance data with no identifying information. We abstracted individual clients VMMC data with permission from facility administrators. In addition, the Office of the Associate Director for Science, U.S. Centres for Disease Control and Prevention, determined this project as a non-human subject’s research that will be in response to a public health problem with the primary intent of public health practice (epidemic disease control)
Conflict of Interest
The authors declare that they had no competing interests.
Acknowledgments
We acknowledge the Public Health Fellowship Program and the Ministry of Health, Uganda, for implementation support, Makerere University School of Public Health and CDC Uganda for support and oversight. We also thank Kisenyi, Kiira, Kajjansi and Wakiso health Centre IVs for allowing us access VMMC dataset.
References
- Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS Med. 2005;2(11):e298.
- Bailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger JN, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet. 2007;369(9562):643-56.
- Bailey RC EO RS. Male circumcision for HIV prevention: a prospective study of complications in clinical and traditional settings in Bungoma, Kenya. Bull World Health Organ 86: 669–677. 2006. 2006.
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, Nalugoda F, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet. 2007;369(9562):657-66.
- Mwandi Z MA RJ, Chesang K, Njeuhmeli E, et al. Voluntary medical male circumcision: translating research into the rapid expansion of services in Kenya, 2008–2011. PLoS Med 8 (11) e1001130. . 2011.
- Uganda Launches National Policy for Safe Male Circumcision [press release]. 2010.
- Kripke K VA, Kirungi W, Musinguzi J, Opio A, Ssempebwa R, Nakawunde S, Kyobutungi S, Akao JN, Magala F, Mwidu G, Castor D. and Njeuhmeli E. “Modeling the impact of Uganda’s safe male circumcision program: Implications for age and regional targeting.”. PLoS One. 2016;11 (7).
- Kaitlyn Atkins PTY, Caitlin E. Kennedy, Virginia A. Fonner, Michael D. Sweat, Kevin R. O’Reilly2, Rachel Baggaley3, George W. Rutherford, Julia Samuelson: . Service delivery interventions to increase uptake of voluntary medical male circumcision for HIV prevention: A systematic review. 2020.
- Price JE PL, Mulenga D, Hewett PC, Topp SM, Shiliya N, et al. Behavior change pathways to voluntary medical male circumcision: narrative interviews with circumcision clients in Zambia. PLoS One. 2014;9(11).
- . Mahler H SS, Plotkin M, Kulindwa Y, Greenberg S, Mlanga E, et al. Covering the last kilometer: using GIS to scale-up voluntary medical male circumcision services in Iringa and Njombe regions, Tanzania. Glob Health Sci Pract. 2015;3(3):503–15.
- Hellar AM BD, Mahler H, Plotkin M, Ng’wanakilala T, Curran K, et al. Mobile VMMC teams in Tanzania see older clients and have higher followup rates. op Antivir Med 2015; 23(e-1):502.
- Ashengo TA HK, Mahler H, Rock A, Kanagat N, Magalona S, et al. Voluntary medical male circumcision- (VMMC) in Tanzania and Zimbabwe: service delivery intensity and modality and their influence on the age of clients. PLoS One. 2014;9(5):e83642.
- .Plotkin M CD, Mziray H, Ku¨ver J, Mpuya E, Luvanda PJ, et al. . “Man, what took you so long?” Social and individual factors affecting adult attendance at voluntary medical male circumcision services in Tanzania. 2013.
- Ezzati M, Lopez, Alan D, Rodgers, Anthony A & Murray, Christopher J. L. Comparative quantification of health risks : global and regional burden of disease attributable to selected major risk factors. 2004.
- FHI360. Corridors of Hope. Zambia Behavioral Surveillance Survey. Adolescent and Mobile Populations. 2007.
- Kibira SP, Daniel M, Atuyambe LM, Makumbi FE, Sandoy IF. Exploring drivers for safe male circumcision: Experiences with health education and understanding of partial HIV protection among newly circumcised men in Wakiso, Uganda. PLoS One. 2017;12(3):e0175228.
- Wawer MJ, Tobian AA, Kigozi G, Kong X, Gravitt PE, Serwadda D, et al. Effect of circumcision of HIV-negative men on transmission of human papillomavirus to HIV-negative women: a randomised trial in Rakai, Uganda. Lancet. 2011;377(9761):209-18.
DOWNLOAD THIS ARTICLE![]()
![]()
![]()
Comments are closed.