
Sustained Measles Transmission in Kabulasoke, Uganda: The role of Suboptimal Vaccination, Delayed Detection, and Gender-Based Barriers, March–July 2025.
Authors: Sharon Namasambi1*, Richard Migisha1, Kigongo John Vianney1, Nakabuye Maria1, Benon Kwesiga1, Yasiin Nuwamanya2, Rita Atugonza2, Fred Nsubuga2, Ampaire Immaculate2 Institutions of affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Ministry of Health-Uganda National Expanded Program on Immunisation *Correspondence*: Tel: +256772511067, Email: nabsharon@uniph.go.ug
Summary
Background: Measles is a highly contagious, vaccine-preventable disease with significant morbidity and mortality, particularly in settings with suboptimal immunization coverage. An outbreak was confirmed on May 27, 2025, in Kabulasoke Subcounty, Gomba District, Uganda. We investigated the outbreak, which spanned from March to July 2025, to determine its magnitude, identify risk factors, assess vaccine coverage and effectiveness, and recommend appropriate control measures.
Methods: The investigation used a mixed-methods approach, including medical record reviews, active case finding, and environmental assessments from March to July, 2025. Cases were classified per WHO definitions: a suspected case involved onset of fever, a maculopapular rash, and ≥1 of cough, coryza, or conjunctivitis in a Kabulasoke resident from March 1 to July 30, 2025; confirmed cases were positive for measles-specific IgM. We computed Attack Rates (AR) and conducted a 1:2 matched case–control study (80 cases, 160 controls) to identify risk factors for measles infection. Vaccine Effectiveness and coverage ware estimated from vaccination data, and surveillance timeliness was assessed using the 7-1-7 framework.
Results: We identified 106 case-patients (5 confirmed), with one suspected death. The overall AR was 24/10,000, peaking in children aged 9–17 months (AR: 130/10,000). Males accounted for 60% (n=64/106) of all cases. Cases were geographically concentrated in Lugaaga Parish, with a notable cluster at Sunrise Infant School. Overall Measles-Rubella (MR) coverage was 72%, and VE was estimated at 60% (aOR=0.4, 95% CI 0.3–0.6). Factors associated with infection included: non-vaccination (aOR=2.5, 95% CI 1.7–3.3); school attendance at Sunrise Infant School (aOR=1.7, 95% CI 1.1–2.7); and contact with a symptomatic person while playing away from home (aOR=2.1, 95% CI 1.2–3.7). Surveillance showed a 33-day delay in detection, far exceeding the 7-day target. In-depth interviews revealed that male-dominated household decisions, mistrust in vaccines, reliance on traditional remedies, and limited healthcare access fueled sustained transmission.
Conclusion: This outbreak highlights the persistent challenges of measles control in low-resource settings, where sociocultural factors, gaps in vaccination coverage, and delayed detection can sustain transmission. Strengthening routine and outreach immunization, implementing school-based preventive measures, fostering culturally sensitive community engagement, and enhancing surveillance timeliness are essential to mitigate future outbreaks and build resilient local health systems.
Background
Measles is a highly contagious, vaccine-preventable viral infection. It is caused by a single-stranded RNA virus, with transmission occurring primarily via respiratory droplets or direct contact. Measles is one of the most transmissible infectious diseases, with a basic reproduction number (R0) of 12–18 in unvaccinated populations. The disease is characterized by a prodrome of high-grade fever, cough, coryza, and conjunctivitis, followed by a maculopapular rash (1–3).
Despite the availability of an effective vaccine, outbreaks continue to occur due to suboptimal vaccination coverage (3,4), with both national and global coverage remaining below the 95% herd immunity threshold(5–7). In Uganda, the Measles-Rubella (MR) vaccine is administered at 9 and 18 months of age. By mid-2025, nearly half of Uganda’s districts had reported measles outbreaks. On 27 May 2025, five laboratory-confirmed measles cases were reported from Kabulasoke Subcounty in Gomba District. A National Rapid Response Team (NRRT), supported by the Uganda Public Health Fellowship Program (PHFP), was deployed to investigate and guide control interventions. We determined the magnitude of the outbreak, identified risk factors, assessed vaccine coverage and effectiveness, and recommended evidence-based control measures, March to July, 2025.
Methods
To investigate the Kabulasoke measles outbreak (March 1–July 30, 2025), a comprehensive approach was used combining descriptive epidemiology and analytic studies. A suspected case was defined as onset of fever, maculopapular rash, plus ≥of cough, coryza, or conjunctivitis, while a confirmed case required measles-specific IgM positivity. Initial methods included reviewing medical records, performing active case finding (line-listing cases and verifying them through facility reviews and community searches), and computing Attack Rates (AR) by age, sex, and parish. To assess risk factors for measles infection, we conducted a 1:2 matched case–control study involving 80 cases and 160 controls in Lugaaga Parish. Data were analysed using conditional logistic regression, and vaccine effectiveness (VE) was calculated as VE= (1 − aOR) × 100%. Vaccination Coverage (VC) was determined from eligible controls’ status, verified via cards, registers, or recall. Finally, environmental and qualitative assessments (observations and key informant interviews) were performed to understand community perceptions and barriers; while surveillance timeliness was evaluated using the WHO 7–1–7 framework.
The investigation was conducted as part of the Ministry of Health’s response to a public health emergency under the National Rapid Response Team (NRRT). Administrative clearance to conduct the investigation was obtained from the Ministry of Health, and a non-research determination was granted by the U.S. Centers for Disease Control and Prevention (CDC) in compliance with applicable U.S. federal laws. Administrative clearance was additionally obtained from Gomba District Health Authorities. Given the minimal risk involved, verbal informed consent and assent were obtained from all participants prior to interviews. Privacy was ensured during data collection, and all information was treated with strict confidentiality throughout the investigation.
Results
Descriptive epidemiology
We identified a total of 106 case-patients. The highest burden was among children aged 9–17 months (AR 130/10,000). Lugaaga Parish recorded the highest AR (120 per 10,000), followed by Mawuuki (54 per 10,000).
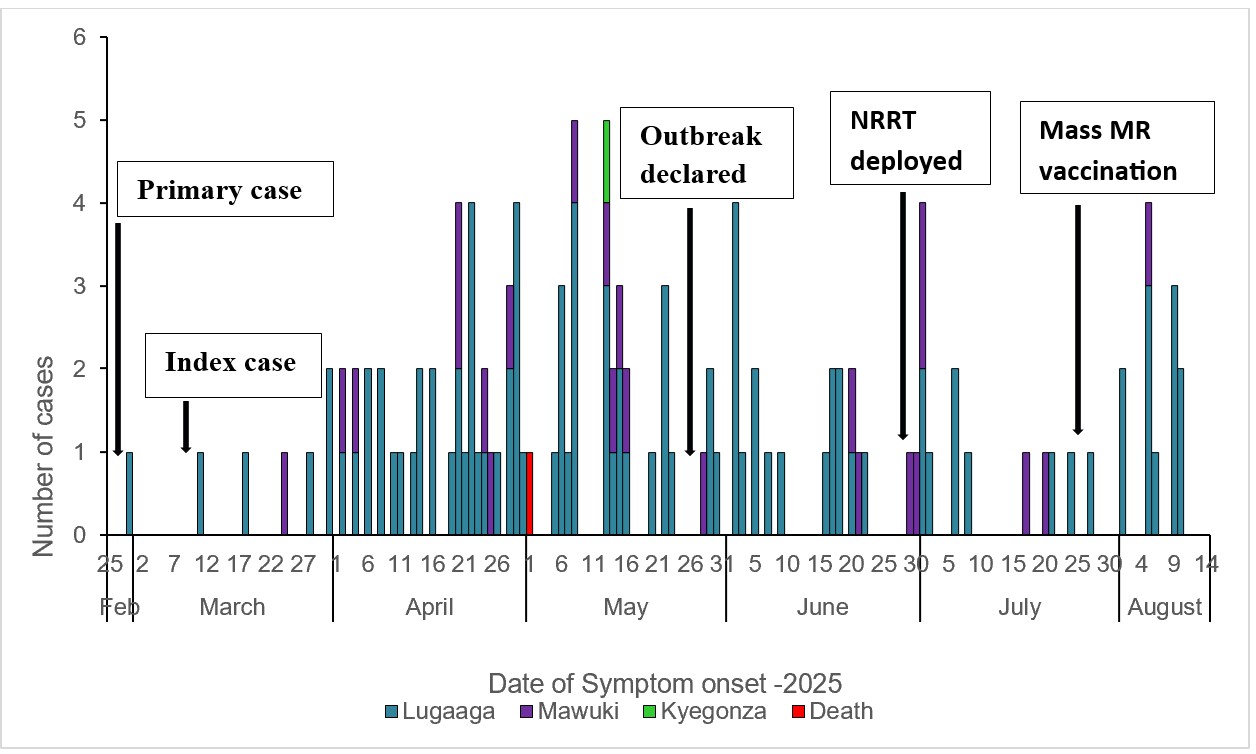
The measles outbreak in Kabulasoke Subcounty in 2025 was imported in late February by a primary case returning from Rakai district. It became a propagated outbreak with amplification among school-aged children and their households. Community awareness triggered detection in April, followed by laboratory confirmation on May 13 and a formal declaration by the Ministry of Health on May 27. The subsequent control measures, including the deployment of the National Rapid Response Team and a supplementary immunization campaign achieving 72% coverage, successfully interrupted transmission by August 30, 2025.
Environmental assessment findings
Environmental assessments revealed limited health infrastructure, poor isolation practices in schools, and weak private sector reporting. Qualitative findings indicated vaccine hesitancy influenced by patriarchal decision-making, fear of side effects, and reliance on traditional remedies such as Citropsis articulata (‘Omutulika’). Children frequently mixed in play without restrictions, fostering continuous transmission.
Surveillance Timeliness (7-1-7 metrics) findings
The 7–1–7 assessment revealed a 33-day delay from symptom onset of the index case to official detection, exceeding the WHO target. Delays stemmed from low community awareness, limited clinical suspicion, and weak surveillance capacity at subcounty level.
Risk factors for measles transmission in Kabulasoke Subcounty, Gomba District, Uganda, March–July 2025
Children aged 6 months to 14 years who were unvaccinated, attended school, and engaged in social activities outside the home were hypothesized to likely develop measles during the outbreak. In a matched case–control analysis, children who had received at least one dose of MR vaccine were significantly protected, (adjusted odds ratio [aOR]=0.4, 95% CI: 0.3–0.6) compared to unvaccinated children. Attending Infant School X was independently associated with higher risk of being a case compared to attending other schools (aOR=1.7, 95% CI: 1.1–2.7); and exposure to symptomatic children during play was strongly associated with illness (aOR=2.1,95% CI: 1.2–3.7). Similarly, primary play interactions occurring away from home were linked to increased odds of being a case (aOR=1.6, 95% CI: 1.0–2.4) (Table 1).
Table 1: Risk factors for measles transmission in Kabulasoke Subcounty, Gomba District, Uganda, March–July 2025
| Risk factor | Number (%exposed) | cOR
(95% CI) |
aOR
(95% CI) |
|
| Cases n (%) |
Controls n (%) |
|||
| Vaccination status (≥ 1 MR dose)Yes No |
32 (40) 48 (60) |
115 (72) 45 (28) |
0.3 (0.2-0.5) Ref |
0.4 (0.3-0.6) Ref |
| Currently Attending School
Yes No |
50 (63) 30 (37) |
73 (46) 86 (54) |
1.9 (1.1-3.4) Ref |
– |
| School Attended
Infant school X Other schools |
32 (64) 18 (36) |
18 (25) 55 (75) |
5.2 (2.5-11) Ref |
1.7 (1.1-2.7) Ref |
| Participated in any social activities prior to symptom onset
Yes No |
56 (70) 24 (30) |
99 (62) 61 (38) |
1.4 (0.8-2.6) Ref |
– |
| Had contact with symptomatic children during play time
Yes No |
61 (76) 19 (24) |
84 (53) 76 (47) |
2.9 (1.6-5.3) Ref |
2.1 (1.2-3.7) Ref |
| Location of primary play interaction
Away from home At home |
54 (68) 26 (32) |
82 (51) 78 (49) |
1.9 (1.1-3.4) Ref |
1.6 (1.0-2.4) Ref |
Vaccine coverage and effectiveness
Only 22% (32/80) of case-patients had received at least one measles-rubella vaccine dose compared to 72% (115/160) of controls, reflecting suboptimal coverage. Vaccine effectiveness was estimated at 60% (aOR = 0.4; 95% CI: 0.27–0.55), demonstrating substantial protection against measles infection in Kabulasoke Subcounty.
Discussion
The measles outbreak in Kabulasoke Subcounty highlights the vulnerability of rural, low-resource settings with suboptimal measles–rubella (MR) vaccination coverage. The outbreak followed a propagated pattern driven by low vaccine uptake, school-based transmission, household exposure, and delayed detection and response, consistent with findings from Uganda and similar sub-Saharan African settings (4,8–11).Children aged 9–17 months were disproportionately affected, reflecting heightened susceptibility before completion of the two-dose MR schedule, a pattern widely documented in high-transmission contexts(3,10-11).Although vaccination was protective, coverage remained critically low: only 22–35% of case-patients had received at least one MR dose, and estimated population coverage was 72%, far below the ≥95% threshold required for herd immunity(6,12).Transmission was amplified in congregate settings, particularly schools, where dense clustering and prolonged contact has been documented to facilitate spread among susceptible children, as well as frequent community social interactions(4,8–11).Delayed outbreak detection;33 days after symptom onset, exceeded the WHO 7-day benchmark, reflecting low community awareness, limited clinical suspicion, and weak surveillance at the frontline, challenges commonly reported in rural Uganda(2,13-14).Consistent with immunization studies conducted in sub-Saharan Africa, environmental and qualitative assessments identified several structural and sociocultural barriers, including limited access to public health facilities, reliance on private providers not fully integrated into surveillance systems, patriarchal household decision-making, residual mistrust from previous vaccination experiences, and culturally embedded perceptions of measles as a routine childhood illness managed with traditional remedies. These findings indicate that measles transmission in Kabulasoke Subcounty was sustained not only by gaps in service availability but also by deeply rooted social norms and health-seeking behaviors(13,14).
Study limitations
Incomplete vaccination records and reliance on caregiver recall may have introduced information and recall bias, potentially resulting in misclassification of vaccination status and imprecise estimates of vaccine coverage and effectiveness. Consequently, associations between vaccination and measles infection should be interpreted cautiously. Nevertheless, triangulating epidemiological and qualitative data strengthened understanding of the outbreak’s underlying drivers.
Public health actions
The District Health Team was re-oriented on measles case definitions, line-listing, and 7–1–7 response metrics. Active case finding was intensified, and community leaders mobilized for vaccination and health education. A mass measles vaccination campaign conducted in July 2025 targeted all children aged 6–59 months, reaching 72% coverage.
Conclusion
The measles outbreak in Kabulasoke Subcounty, imported from the Rakai district, was driven by low measles-rubella vaccination coverage and amplified by school-based transmission and frequent social interactions. The findings illustrate how limited access to health services and vaccine hesitancy shaped by cultural and gender norms can sustain measles transmission in rural settings. Strengthening routine and community-based immunization through expanded outreach in underserved areas, engaging male household decision-makers alongside religious and cultural leaders, and leveraging schools for screening and periodic vaccination may improve coverage and community trust. Similarly, enhancing surveillance sensitivity through continuous training of health workers and Village Health Teams, integrating private healthcare providers into reporting systems, and implementing culturally responsive risk communication could support earlier detection, increase vaccine uptake, and contribute to measles elimination efforts.
Conflict of Interests: The authors declare no conflict of interests
Author Contributions: SN conceptualized and led the investigation. VJK and MN contributed to data collection, while RM supervised the field investigation. SN and VJK conducted data analysis, and SN led the drafting of the bulletin article. VJK, MN, LB and RM contributed to writing and reviewing the bulletin article to ensure scientific rigor and intellectual content. All authors reviewed and approved the final draft for submission.
Acknowledgements: We acknowledge the Gomba District Health Team, Kabulasoke Subcounty leadership, and community members for their support. We thank the Ministry of Health, UNEPI, and Uganda National Institute of Public Health (UNIPH) for technical guidance. We are grateful to the U.S. CDC through the Uganda Public Health Fellowship Program for funding this investigation.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission. However, citation as to source is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, et al. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis. 2017 Dec 1;17(12): e420–8.
- Husada D, Kusdwijono, Puspitasari D, Kartina L, Basuki PS, Ismoedijanto. An evaluation of the clinical features of measles virus infection for diagnosis in children within a limited resources setting. BMC Pediatr. 2020 Jan 6;20(1):5.
- admin. Measles outbreak Investigation in Terego District, Uganda, May- June, 2024. – UNIPH [Internet]. 2024 [cited 2025 Oct 20]. Available from: https://uniph.go.ug/measles-outbreak-investigation-in-terego-district-uganda-may-june-2024/
- Nsubuga EJ, Morukileng J, Namayanja J, Kadobera D, Nsubuga F, Kyamwine IB, et al. Measles outbreak in Semuto Subcounty, Nakaseke District, Uganda, June–August 2021. IJID Reg. 2022 Dec; 5:44–50.
- Plans-Rubió P. Measles Vaccination Coverage and Anti-Measles Herd Immunity Levels in the World and WHO Regions Worsened from 2019 to 2023. Vaccines. 2025 Feb;13(2):157.
- Vaccines and immunization [Internet]. [cited 2025 July 21]. Available from: https://www.who.int/health-topics/vaccines-and-immunization
- Tahir IM, Kumar V, Faisal H, Gill A, Kumari V, Tahir HM, et al. Contagion comeback: unravelling the measles outbreak across the USA. Front Public Health [Internet]. 2024 Dec 18 [cited 2025 July 21];12. Available from: https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2024.1491927/full
- Okiror EO, Ampaire I, Nsubuga F, Kwizera P, Okello PE, Migisha R, et al. Measles outbreak with children below the recommended age for first dose of measles vaccine most affected in Kakumiro District, February–May 2024. 2024;9(3).
- Majwala RK, Nakiire L, Kadobera D, Ario AR, Kusiima J, Atuhairwe JA, et al. Measles outbreak propagated by children congregating at water collection points in Mayuge District, eastern Uganda, July – October, 2016. BMC Infect Dis. 2018 Aug 20;18(1):412.
- Walekhwa AW, Ntaro M, Kawungezi PC, Achangwa C, Muhindo R, Baguma E, et al. Measles outbreak in Western Uganda: a case-control study. BMC Infect Dis. 2021 June 22;21(1):596.
- Qin S, Ding Y, Yan R, He H. Measles in Zhejiang, China, 2004-2017: Population Density and Proportion of Floating Populations Effects on Measles Epidemic. Health Secur. 2019;17(3):193–9.
- CDC. Measles (Rubeola). 2025 [cited 2025 July 21]. Measles Cases and Outbreaks. Available from: https://www.cdc.gov/measles/data-research/index.html
- Solomon K, Aksnes BN, Woyessa AB, Sadi CG, Matanock AM, Shah MP, et al. Qualitative Insights on Barriers to Receiving a Second Dose of Measles-Containing Vaccine (MCV2), Oromia Region of Ethiopia. Vaccines. 2024 June 22;12(7):702.
- Larson HJ, Jarrett C, Eckersberger E, Smith DMD, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine. 2014 Apr 17;32(19):2150–9.
Comments are closed.