
Magnitude and drivers of mpox in Mbarara City, October 2024–May 2025
Authors: Vianney John Kigongo1*, Pauline Achom1, Justine Wobusobozi1, Sharon Namasambi1, Nasif Matovu1, Maria Nakabuye1, Winfred Nakaweesi1, Martha D. Nalweyiso1, Anne Loy Alupo1, Deborah Aujo1, Aman D. Kyomugisha1, Michael Mutegeki1, Aminah Namwabira1, Francis Mugabi2, Irene Kyamwine1, Richard Migisha1, Benon Kwesiga1 Institutional affiliations: 1Uganda Public Health Fellowship Program, Kampala, Uganda 2Mbarara Regional Referral Hospital Correspondence*: Tel: +256780109590, Email: kigongojv@uniph.go.ug
Summary
Background: By April 2025, Mbarara City had the highest mpox national attack rate of 142 cases per 100,000 population. We investigated to determine the scope of mpox, estimate proportion of missed cases in medical records and identify drivers of outbreak transmission in Mbarara City October 2024-May 2025.
Methods: We defined a confirmed case as an RT-PCR-positive patient admitted to Mbarara Regional Referral Hospital (MRRH) while a suspected case was defined as acute onset of skin rash or genital lesions with ≥2 of the following: fever ≥38.5°C, headache, weakness, myalgia, back pain, genital discharge, lymphadenopathy, or mucosal lesions, in a resident of Mbarara City between October 2024 and May 2025. We reviewed records at MRRH to find cases and further conducted active case search through house-to-house interviews in Nyamityobora Ward which was the most affected in Mbarara City. We administered a questionnaire to collect data on demographics, clinical symptoms, and risk factors. We line listed all identified cases and described case-patients by person, place, and time.
Results: We identified 317 records of confirmed mpox cases from Mbarara City admitted at MRRH, of which 175 (55%) were male, and 292 (92%) were aged 15-44 years. The overall attack rate was 12 cases per 10,000 population. Males had a higher attack rate (14/10,000) than females (10/10,000). The active case search in Nyamityobora Ward identified a total of 106 mpox cases which included 91(86%) new cases that were not previously recorded in hospital data. Of these, 96 adult cases (excluding 7 children) reported on exposure history. Sexual contact 63% (60/96) was more common. Fifty-one percent (49/96) of the cases initially sought care at private clinics. Cases appeared to cluster geographically around specific business types, including brothels, bars, guest houses, and betting companies.
Conclusion: The true burden of mpox was underestimated by a factor of at least 2, with private facilities most often the first point of care. Sexual contact was the main driver of the outbreak. We recommend educating private providers on suspect case identification and referral and promoting community-wide awareness on mpox.
Background
Mpox, previously known as monkeypox, is a viral illness caused by the monkeypox virus, a species of the genus Orthopoxvirus [1]. It primarily spreads from person to person mainly through close contact with someone who has mpox. It can also be transmitted via contaminated objects, from mother to child during pregnancy or child birth, and from infected animals [1]. Symptoms include fever, rash, swollen lymph nodes, and body pain. Severe illness can occur, especially in immunocompromised individuals [2].
On July 24, 2024, Uganda confirmed its first cases of mpox reported in Kasese District [3]. Mpox spread rapidly to over 115 districts, with transmission in Mbarara confirmed on November 4, 2024.
According to the national situation report of 6th April 2025, Mbarara was ranked third in the number of reported mpox cases (420) outside the Kampala Metropolitan Area (KMA), followed closely by Masaka. Furthermore, the 16th April 2025 situation report indicated that Mbarara had the highest attack rate nationally at 142 cases per 100,000 population, surpassing even Kampala. While multiple investigations have been conducted extensively in the KMA, key epidemiological questions remain unanswered in Mbarara and surrounding areas. Additionally, whereas epi curves in other districts were starting to flatten, that of Mbarara continued to peak, signaling ongoing transmission and potential gaps in outbreak control efforts. We investigated to estimate the mpox magnitude, describe transmission dynamics, and develop actionable recommendations for outbreak control in Mbarara City, October 2024-May 2025.
Methods
Mbarara City is a major urban center in southwestern Uganda and serves as the administrative and commercial hub of the region. It is supported by a network of public and private health facilities, with Mbarara Regional Referral Hospital (MRRH) functioning as the main referral facility and designated isolation center for suspected and confirmed mpox cases. MRRH played a central role in case management and coordination of the regional outbreak response.
We defined mpox cases as suspected or confirmed cases. A suspected case was defined as acute onset of skin rash or genital lesions with ≥2 of the following: fever ≥38.5°C, headache, general body weakness, myalgia, back pain, genital discharge, lymphadenopathy, mucosal lesions in a resident of Mbarara City from Oct 2024 to May 2025; a confirmed case was defined as RT-PCR-confirmed mpox infection in a resident of Mbarara City from October 2024 to May 2025.
We reviewed records of confirmed cases managed at the MRRH isolation unit between October 3, 2024, and May 9, 2025. We captured data on socio-demographic characteristics, exposure history, clinical symptoms, past medical history, laboratory results, and case outcomes. Using this information, we generated a line list.
We then conducted house-to-house active case finding in Nyamityobora Ward, the most affected in Mbarara City with the help of Village Health Teams (VHTs). We screened residents for symptoms consistent with mpox and interviewed consenting case-patients to obtain additional epidemiological and clinical information. We compared the active case search data with the medical records to determine the proportion of missed cases at MRRH from Nyamityobora Ward, Mbarara City.
We performed descriptive epidemiology on the line-listed case-patients by time, place, person characteristics.
Results
We identified records of 317 confirmed cases from Mbarara City at the isolation unit of MRRH. Of these, 175 (55%) were male, and 292 (92%) were aged 15–44 years. The overall attack rate was 12 cases per 10,000 population. Males were more affected (AR=14 per 10,000) compared to females (AR=10 per 10,000).
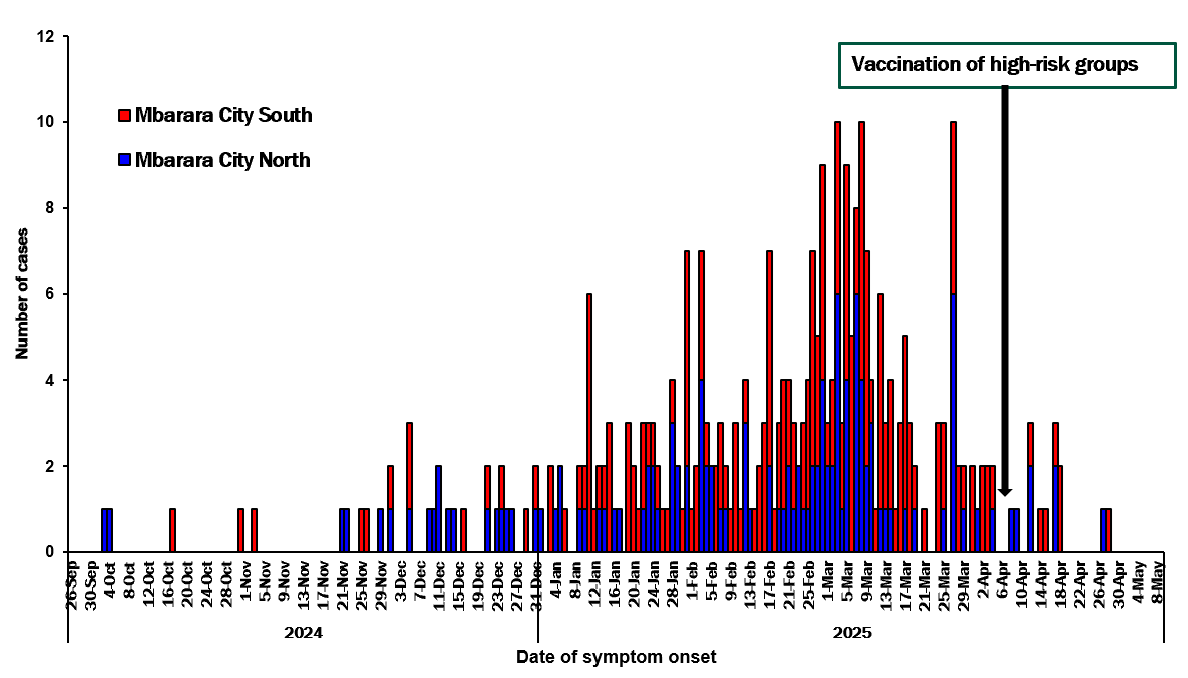
The outbreak began in Mbarara City North and later spread to Mbarara City South. This graph suggests a propagated outbreak. Both administrative units had continued reporting of cases with Mbarara City South reporting more cases over time. The outbreak peaked in March 2025 and vaccination of high-risk groups commenced on 4th April, 2025 (Figure 1).
We identified and interviewed a total of 106 cases from Nyamityobora ward, which was the most affected in Mbarara City South. Half of these were confirmed cases. Of these, 54% (57/106) were female. The majority (85%) of the cases were aged 15-44 years.
Fifty-one percent (49/96) of the cases that sought care reported private clinics as the most common first point of care.
The active case search in Nyamityobora Ward identified a total of 106 mpox cases which included 91(86%) new cases that were not previously recorded in hospital data.
Of the 106 cases, 96 adults (7 children excluded) reported exposure history. Among these, sexual contact 63% (60/96) was more common than non-sexual contact.
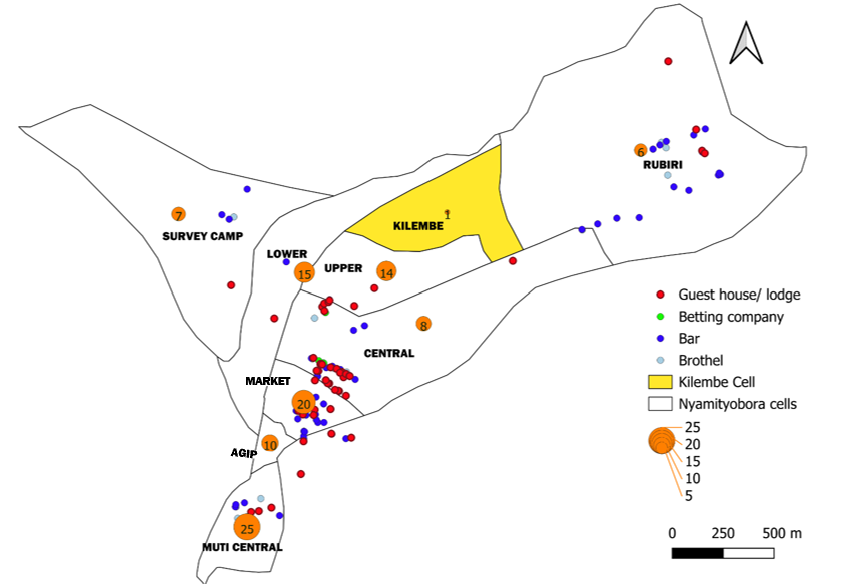
Cases appeared to cluster geographically around brothels, bars, guest houses, and betting companies(Figure 2). The bigger the circle, the higher the number of cases. Notably, Kilembe Cell highlighted in yellow which had none of these businesses, recorded only one case, whereas other cells with these establishments reported at least five cases each.
Discussion
Our investigation highlights a significant mpox outbreak in Mbarara City, with 317 confirmed cases recorded at the referral hospital. The outbreak predominantly affected males and adults aged 30–44 years, consistent with patterns seen in outbreaks where social and sexual networks drive transmission [4-7]. The propagated nature of the outbreak, beginning in Mbarara City North and later spreading to Mbarara City South, suggests ongoing person‑to‑person transmission. Active case finding in one hotspot ward identified many additional cases that were missing from facility records, underscoring the importance of community‑based surveillance to capture the true outbreak magnitude. The clustering of cases around brothels, bars, guest houses, and betting establishments, along with the predominance of sexual contact as a reported exposure, point to high‑risk social and sexual networks as key drivers of transmission patterns that mirror findings in other settings where mpox transmission has been strongly linked to close sexual or intimate contact [8, 9]. Furthermore, the large proportion of cases missed through routine facility records highlights gaps in surveillance and health‑seeking behaviors in high‑risk settings
Study limitations
This investigation depended largely on participants’ self-reported information regarding exposures and behaviors. This methodological approach is susceptible to imperfect recall, which may affect the accuracy of exposure timelines. Furthermore, sensitive issues such as sexual practices may be subject to underreporting due to social desirability bias, and the data could not be independently verified. The active case finding for this study was limited to Nyamityobora Ward. While this area was the most affected in Mbarara City, this geographic restriction means the findings may not be fully representative of or applicable to other parts of the city with different social or epidemiological contexts.
Conclusion
The magnitude of mpox in Mbarara City was underestimated, with most of the cases missed in medical records. Private health facilities were the most common first point of care, and sexual contact emerged as the predominant mode of exposure. We recommend community-based active surveillance, providing health education to private health facilities on suspect case identification and referral, and conducting community awareness campaigns to ensure early detection, timely response, and effective control of mpox outbreaks.
Conflict of interest: The authors declared no conflict of interest.
Authors’ contribution: All authors contributed to the write-up and review of the bulletin article. VJK drafted the initial version of the article. PA, JW, SN, NM, MN, WN, MDN, ALA, DA, ADK, MM, and AN participated in the data collection and case investigations. FM contributed to the acquisition, analysis and interpretation of data. IK, RM and BK supervised the field data collection and reviewed the draft bulletin article for substantial intellectual content. All authors read and approved the final bulletin article.
Acknowledgements: We are so grateful to the management and staff of the mpox isolation unit at MRRH for their support in providing access to facility records and for their indispensable role in facilitating patient-related data collection for this study. We also thank the Ministry of Health and the Uganda Public Health Fellowship Program for their technical support during this study.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- WHO, Mpox. 2025.
- CDC, Signs and Symptoms of Mpox. 2024.
- Abet, T., Uganda confirms two cases of Mpox, in Daily Monitor. 2024.
- Thornhill, J.P., et al., Monkeypox virus infection in humans across 16 countries—April–June 2022. New England Journal of Medicine, 2022. 387(8): p. 679-691.
- Vivancos, R., et al., Community transmission of monkeypox in the United Kingdom, April to May 2022. Eurosurveillance, 2022. 27(22): p. 2200422.
- Riser, A.P., Epidemiologic and clinical features of mpox-associated deaths—United States, May 10, 2022–March 7, 2023. MMWR. Morbidity and Mortality Weekly Report, 2023. 72.
- Sharma, A., et al., Monkeypox epidemiology, clinical presentation, and transmission: a systematic review. International journal of emergency medicine, 2023. 16(1): p. 20.
- Daniel Wenani, A.K., Edith Namulondo, Hannington, et al., Epidemiological characteristics and transmission dynamics of the first 66 confirmed mpox cases, Nakasongola District, Uganda, . 2024.
- Ogoina, D., et al., Mpox Epidemiology and Risk Factors, Nigeria, 2022. Emerg Infect Dis, 2024. 30(9): p. 1799-1808.
Comments are closed.