
Improving completeness of requests at a selected government veterinary laboratory X in Kampala Metropolitan area using a quality improvement approach, December 2024
Nabatta Esther1,2*, Samuel Gidudu1, Gladys Nakanjjako2, Olympia Mugarura2, and Abumelech Byamukama2 Institutional affiliations:1Uganda Public Health Fellowship Program, Laboratory Leadership Program, Uganda National Institute of Public Health, Kampala, Uganda, 2National Animal Disease Diagnostics and Epidemiology Center, Ministry of Agriculture Animal IF, Entebbe, Uganda *Correspondence: Tel: +256 782539910, Email: enabatta@uniph.go.ug
Summary
Background: Although the World Organization for Animal Health (OIE) provide requirements for sample collection and documentation, anecdotal evidence from a government veterinary laboratory X indicated that samples were often submitted with incomplete request forms. Using a continuous quality improvement (CQI) approach, we aimed at improving the form completeness to 70% by December 2024 at the veterinary laboratory X.
Methods: Applying a CQI approach, conducted a baseline assessment, identified two main issues: lack of staff orientation and a non-user-friendly form design as the root causes of form incompleteness. We redesigned the request form and mentored staff on the use of the revised form. A subsequent decline prompted assigning a dedicated staff member to follow up on completion of the request forms.
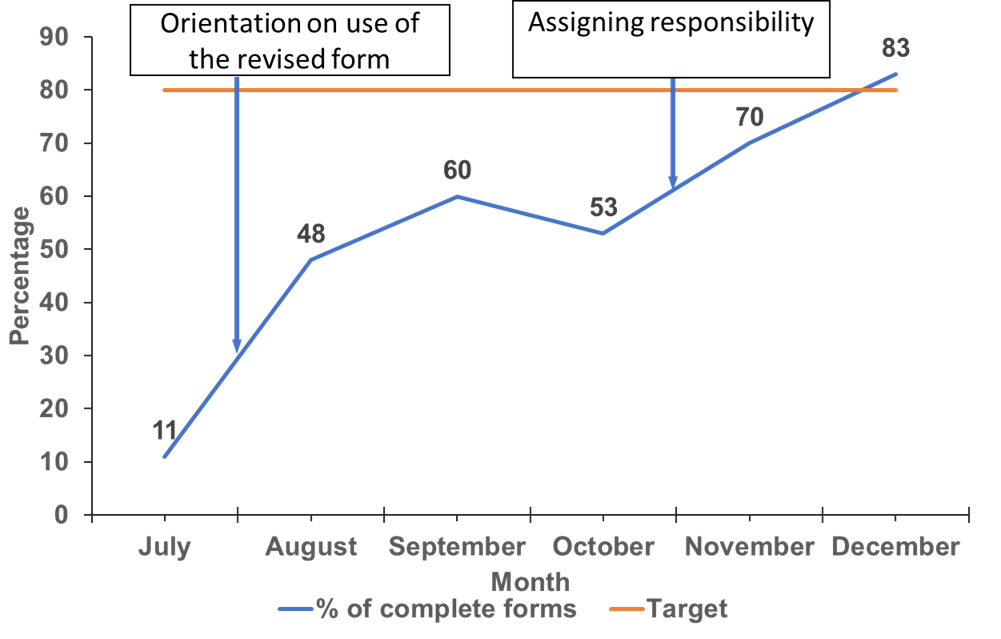
Results: At baseline, only 11.3% of the samples had complete request forms. Following form redesign and staff mentorship, a 60% raise in form completeness was realized within the first three months. Addition of a follow up component further improved the completeness to 83%, exceeding the 70% target.
Conclusion: The multi-layered CQI intervention significantly improved form completion. To sustain the gains, we recommend integrating the revised form and follow-up mechanisms into the laboratory standard operating procedures and quality systems, supported by regular monitoring and refresher trainings.
Introduction
The reliability of diagnostic testing is a cornerstone of effective animal disease surveillance, control, and public health protection. Veterinary laboratory X is key in diagnosing diseases such as African Swine Fever, Foot and Mouth Disease, tick borne diseases and zoonotic threats like Rift Valley Fever, Brucellosis, Rabies, and Crimean Congo Hemorrhagic Fever. The analytical precision of diagnostic platforms is fundamentally dependent on the quality of the pre-analytical phase, which includes the submission of accurate and complete sample information on the laboratory request forms (1). Laboratory request forms provide essential epidemiological, clinical, and demographic information as emphasized in the by international standards such as the Animal Health (OIE) guidelines on sample collection (3). Although the OIE provide requirements for sample collection and documentation, anecdotal evidence from a government veterinary laboratory X indicated that samples were often submitted with incomplete request forms or sometimes with no forms at all. Using a continuous quality improvement (CQI) approach, we aimed at improving form completeness to 70% by December 2024 at the veterinary laboratory X.
Methods
We conducted the project at a government veterinary laboratory X, located in the greater Kampala metropolitan area serving the outskirts of Kampala and several districts through providing confirmatory testing of several animal diseases. The project was conducted by the veterinary laboratory X’s existing quality improvement committee led by the quality officer. The committee conducted a retrospective review of forms accompanying samples received over a four-month period (January to April 2024). Additionally, a questionnaire was subjected to all veterinary laboratory X staff involved in sample reception to understand the possible causes of submission of samples without or with incomplete forms. Using root cause analysis techniques, we identified lack of orientation for staff on request form filling was the most modifiable root cause for form incompleteness. The form not being user friendly was a secondary contributing factor. To address the root cause, we redesigned the form and mentored the staff on its use. A subsequent decline in completeness prompted assigning a laboratory staff to follow upon request form completion.
We designed an action plan with suggested changes that we monitored over a period of three months for action implementation and an additional three months for action (intervention) effectiveness.
To monitor the tested change, we collected data every month on the number of samples received at the veterinary laboratory X with complete request forms (as the numerator) and the number of samples received at the veterinary laboratory X (as the denominator). The proportion of samples received at veterinary laboratory X with complete request forms was then plotted using a line graph.
This study was determined to be a non-research activity by the US Centers for Disease Control and Prevention. Administrative clearance to conduct the study was sought from the laboratory leadership. Verbal informed consent was obtained from the staff before obtaining information regarding the possible root causes for incomplete request forms.
Results
At baseline, of the 106 forms accompanying samples received between the months of January and April 2024, only 12 (11.3%) were complete. Out of the 94 incomplete forms, 33 (35.1%) were ad hoc (improvised pieces of paper with scribbles of information), 35(37.2%) were district-developed forms, and 26 (27.7%) were incomplete standard laboratory test request forms. Following intervention implementation, there was an improvement from 11% to 60% in the first three months (July-September 2024). Subsequently assigning a laboratory staff to follow up on form completeness-related issues led to an increase to 83% surpassing the set target of 70% (Figure 1).
Discussion
The CQI approach successfully increased the completeness of laboratory request forms from 11% to 83%, exceeding the 70% target. The baseline reflected a systemic lack of standardization and awareness of the request form, with over one-third of forms being improvised documents. Improvement required a multilayered approach that involved redesigning the form, staff orientation, and assigning a laboratory staff to follow up on form completion. This made the form more user-friendly, reduced complexity and the likelihood of errors. Concurrently, the mentorship sessions were crucial for educating staff on how to complete the new form and, more importantly, why its completeness is critical for diagnostic accuracy and national disease surveillance. Although these were effective, a decline in performance midway into the project could have occurred due to behavioral changes where by staff are bound to revert back to previous habits and practices (9). For accountability and making compliance a routine part of the workflow, a second intervention was instituted which proved to be effective leading to the final improvement of 83%.
Study limitations
We conducted the study at a single veterinary laboratory. This restricts the generalizability of the findings, as the specific root causes identified and the effectiveness of the interventions may be unique to the local context, workflows, and staff dynamics of this particular site.
Conclusions
A multi-layered CQI approach (form redesign, staff mentorship, and accountability) significantly improved form completeness. To sustain gains, we recommend integrating the revised form and follow-up into standard operating procedures, supported by regular monitoring and refresher training.
Conflict of interest: The authors declare that they had no conflict of interest.
Authors’ contributions: EN did the conceptualization of the study idea, data analysis, writing, and editing of the manuscript, SG, GNK, OM, and AB provided guidance in the writing and reviewing of the bulletin. All authors read and approved the final manuscript
Acknowledgements: We acknowledge the US Centers for Disease Control and Prevention Uganda through Makerere University School of Public Health, and Baylor Uganda for technical and implementation support. We extend our heartfelt gratitude all the stake holders and partners for their vital roles in implementing the quality improvement project. Their collaboration, expertise, and dedication were key in effectively improving completeness of the request forms at a selected veterinary laboratory.
Copy right and licensure: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be re printed or published. If cited as a reprint, it should be referenced in the original form.
References
- Lippi, G., Blanckaert, N., Bonini, P., Green, S., Kitchen, S., Palicka, V., … & Plebani, M. (2011). Causes, consequences, detection, and prevention of identification errors in laboratory diagnostics. Clinical Chemistry and Laboratory Medicine, *49*(5), 743-752
- International Organization for Standardization (ISO). (2017). *ISO/IEC 17025:2017 General requirements for the competence of testing and calibration laboratories*.
- World Organization for Animal Health (OIE). (2021) Part 1: General Information on collection and shipment of diagnostic specimens.
- Nutt L, Zemlin AE, Erasmus RT. Incomplete laboratory request forms: The extent and impact on critical results at a tertiary hospital in South Africa. Ann Clin Biochem. 2008 Sep;45(5):463–6.
- Callen J, Georgiou A, Li J, Westbrook JI. The safety implications of missed test results for hospitalised patients: A systematic review. Vol. 20, BMJ Quality and Safety. 2011. p. 194–9.
- Plebani, M. (2019). The detection and prevention of errors in laboratory medicine. Annals of Clinical Biochemistry, 57(2), 118–13019952034.
- Hajalamin M, Awadalla A, Mukhtar M. Assessing, Advising, and Advancing the Filling Practices of the Radiology Request Form in Africa: A Systematic Review. Vol. 14, Diagnostics. Multidisciplinary Digital Publishing Institute (MDPI); 2024.
- Al Muallem Y, Al Dogether M, Househ M, Saddik B. Auditing The Completeness and Legibility of Computerized Radiological Request Forms. J Med Syst. 2017 Dec 1;41(12).
- Korrakuti A. Shaping Leaders, Shaping Habits: Leadership Styles and Their Effect On Habit Formation In Employees. IOSR Journal of Business and Management. 2024 Sep;26(9):18–25.
Comments are closed.