
Effect of Integrated Diseases Surveillance and Response training on notification of epidemic-prone communicable diseases in Uganda
Author: Ben Masiira and Immaculate Nabukenya - ESD, Ministry of Health
Summary
Integrated Disease Surveillance and Response (IDSR) is a comprehensive strategy adopted in African region to improve surveillance. IDSR training is among core functions for strengthening disease surveillance and response. We assessed reporting rates of notifiable diseases before and after districts were trained in IDSR. There was a significant improvement in average weekly reporting rate after IDSR training but only 32% of district achieved the target.
However, monthly reporting rates were above the target in ≥97% of districts before and after the training. This might point to lack of prioritization of weekly reporting by districts. Therefore, strengthening IDSR through trainings might yield limited results if these trainings are not supplemented by other interventions.
Introduction
Communicable diseases remain a significant threat to developing countries and contribute 54% of the disease burden in Uganda (1). Since the beginning of 2015, the country has experienced several disease outbreaks such as typhoid fever, cholera, measles, rubella and malaria. IDSR is a comprehensive strategy proposed by World Health Organization (WHO) to improve public health disease surveillance and response in the African region (2). With support from WHO, the Uganda Ministry of Health has been conducting IDSR trainings in various districts. We assessed the impact of IDSR training, in districts which were trained in 2015, by comparing reporting rates of priority diseases before and after the training.
Methods
We assessed 2015 weekly and monthly reporting rates in the four cohorts of districts that were trained in IDSR for five days. We computed average reporting rates before and after conducting the IDSR training in each of the districts and compared them with a district target of ≥80%. We compared overall weekly average reporting rates before and after the training by using a t-test for comparison of means. We also computed average monthly reporting rates before and after IDSR training.
Results
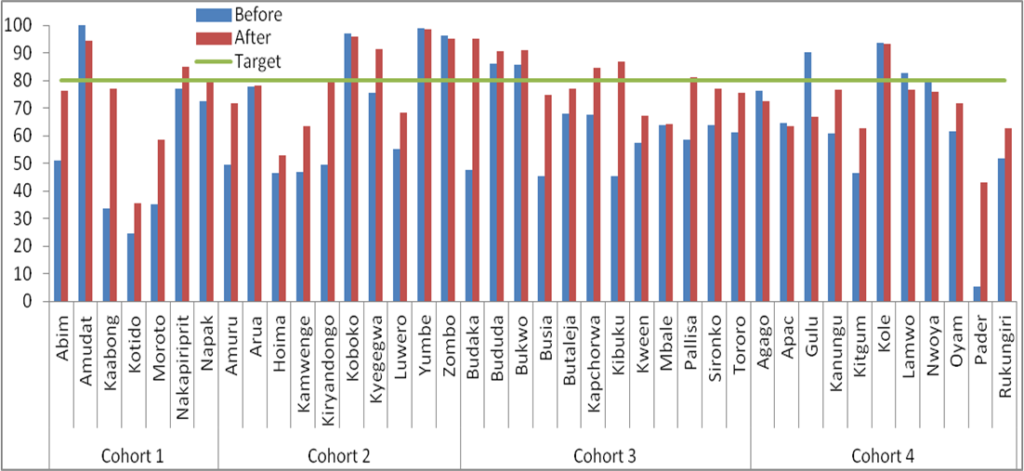
Over all, the reporting rate improved significantly in 73% (29/40) of districts after IDSR training (P<0.001) but only 32% of district achieved the target. The average weekly reporting rate improved in 86% districts trained in cohort 1 but only 14% (n=1) achieved the target (Figure 1). All districts in cohort 1 were above the monthly reporting target before and after the training.
In cohort 2, 60% (n=6) recorded improvement in average weekly reporting rate but 40% (n=4) achieved the target of which only one (Kyegegwa) had reporting rate <80% before the training (Figure 1). All districts in cohort 2 were above the monthly reporting target before and after the training. In cohort 3, 100% (n=12) of districts recorded an improvement in average weekly reporting rate after the training of which 50% (n=6) achieved the target and out of six districts that achieved the target, four had reporting rates below the target before training (Figure 1). Monthly reporting rates before the training were above the target in 92% (n=11) of districts in cohort 3 and 100% (n=12) had reporting rates above the target after IDSR training. There was improvement in average reporting rates in 45% (n=5) of districts trained in cohort 4 but none of these districts achieved the target (Figure 1). Of the districts trained in cohort 4, only 9% (n=1) achieved the. All districts in cohort 4 had monthly reporting rates above the target before and after the training.
Discussion and recommendations
IDSR has been adopted as a national strategy in Uganda since 2000 and much has been achieved regarding its implementation at both national and regional revels in Uganda. IDSR trainings have led to improved reporting in majority of districts but reporting rates are still below the target in 67% of districts.
Despite of low weekly reporting rates, monthly reporting rates were above the performance target before and after IDSR training. Findings of this analysis are similar to an assessment in Tanzania which documented a few districts exceeding performance targets of above 80% after the training on IDSR (3).
It is unclear why districts are unable to achieve weekly reporting targets yet majority can easily achieve monthly targets.
Although several reasons may explain why weekly reporting rates in many districts are low, it is possible that health facilities are not prioritizing weekly reporting. This is due to the fact that most districts were able to achieve monthly targets. Strengthening IDSR through trainings might yield limited results if these trainings are not supplemented by other interventions.
These interventions should target all stakeholders so that they offer full support and commitment to objectives of IDSR. The government investment in recruitment of health workers and HMIS focal persons at health facilities is a useful resource for districts to fulfill their IDSR responsibilities.
Districts need to ensure that all personnel involved in IDSR appreciate the importance of disease surveillance in detection and solving public health threats. Supervision or mentorships to health facilities by districts with support from Ministry of Health is crucial in addressing individual factors such as staff motivation and attitude.
There is need to conduct studies to explore reasons why weekly reporting rates remain low.
Comments are closed.