
Distribution of attempted suicide in Uganda, 2016-2017
Authors: Vivian Ntono1, Steven Kabwama1, Daniel Kadobera1, Hafsa Lukwata1; Affiliation: 1Uganda Public Health Fellowship Program
Summary
Uganda has a high suicide rate of 18.67. We described prevalence of attempted suicide in Uganda, 2016-2017, using data from the Health Management Information System. Males (7.1/100,000) were more affected than females (6.7/100,000). The prevalence of attempted suicide during the study period was highest in the Northern region of Uganda (15/100,000). The proportion of deaths among attempted suicide cases was higher among males (38/1000) than females. Suicide attempts are prevalent in our setting with the Northern region having the highest prevalence. Males were more affected than females. We recommend designing of interventions targeting the most affected groups.
Background
Globally, suicide is one of the 3 leading causes of death among those in the most economically productive age group (15-44 years), and the second leading cause of death in the 15-19 years age group. Uganda has a high suicide rate of 18.67% and it ranks number 17 worldwide and number 4 in Africa[3]. Suicidal behaviors have been conceptualized as a complex process that can range from suicidal ideation, to planning of suicide, attempting suicide, and suicide[2]. Suicide attempts result in a significant social and economic burden for communities due to the utilization of health services to treat the injury, the psychological and social impact of the behavior on the individual and his/her associates and, long-term disability due to the injury. More importantly, a prior suicide attempt is the single most important predictor of death by suicide in the general population[4]. We described prevalence of attempted suicide in Uganda, 2016-2017, using data from the Health Management Information System.
Methods
We extracted data on mental and neurological disorders from the District Health Information System (DHIS2), 2016-2017. DHIS2 is an online master dataset of data submitted by each district using the Health Management Information System data collection tools. The District Health Information System (DHIS) is a community and facility based data aggregation system that was established to facilitate public health related decision-making.
We extracted data on attempted suicide which is defined as a non-fatal, self-directed, potentially injurious behavior with an intent to die as a result of the behavior; might not result in injury. We also extracted data on case type, region, age-group, and sex. We specifically abstracted data from the monthly reports data of attempted suicide, HMIS form 108.
We calculated the overall prevalence of attempted suicide during the study area, prevalence by sex, region, and case type using population data from the national population and housing census report [6]
Results
Prevalence of attempted suicide, Uganda, 2016-2017
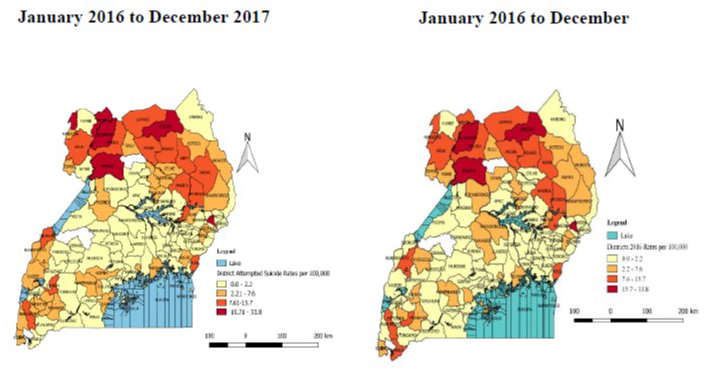
The overall prevalence of attempted suicide during the study period was 6.9/100,000. Males (7.1/100,000) were more affected than females (6.7/100,000). Persons aged ≥ 5years were the only affected (8.3/100,000). Northern region (15/100,000) had the highest prevalence of attempted suicide compared to other region (Table 1 and Figure 1). The overall case fatality rate (CFR) was 28% (72/2589). The CFR was higher among males (50/1302=3.8%) compared to females (22/1287=17%).
Table 1: Prevalence of attempted suicide by sex, age-group, and region, Uganda, 2016-2017
![]()
Discussion
Suicide attempts are prevalent in our setting. The prevalence was highest in the Northern region of Uganda. Another study conducted in the Northern region also found that suicidal ideation and attempt were 12.1 % and 6.2 % respectively [7]. The reported higher suicide prevalence could be due to the region having experienced a long period of active conflict which could have resulted into the communities going through acute distress [8].
The prevalence of attempted suicide was higher for males compared to females. This finding is consistent with other studies that established that attempted suicide was higher among males than females [7]. This is likely because the women have more social support than men therefore less likely to engage in suicide attempt behavior. Women also more often have family support, social networks, good social skills, and are more likely to use telephone help lines, visit family doc-tors, discuss their problems with others, and have better opportunities to access social and health services (11).
The deaths following suicide attempts were higher among males than females. This is consistent with a study done in Singapore that established that men were more likely to die due to suicide attempts than females [9]. This is because the suicide methods used by men are more aggressive than the methods used by females. Furthermore, men have generally been found to be more impulsive than women because they are over-represented in aggressive behavior, accidents, violence-related injuries, drug use, extreme sports, and criminal behavior , risk-taking, all of which have been linked to impulsivity higher suicide rates in men, given that suicidal behavior is associated with impulsivity[10].
Limitations
We were unable to expressively analyze age as it relates to attempted suicide because of the way it was aggregated in the DHIS2.
Conclusions and recommendations
Suicide attempts are prevalent in our setting with the Northern region having the highest prevalence. Males were more affected than females. We recommend designing of interventions targeting the most affected groups.
References
1. WHO. Suicide. 2018 [cited 2018 23/04/2018]; Available from: http://www.who.int/mediacentre/factsheets/fs398/en/.
2. WHO, Public health action for the prevention of suicide: A framework. 2012.
3. WHO. Age Standardized Estimate: World Life Expectancy 6458 [cited 6458 67/48/6458]; Available from: http://www.worldlifeexpectancy.com/cause-of-death/suicide/by-country/.
4. WHO. Preventing Suicide: A global Imperative. 2014 [cited 2018 23/04/2018]; Available from: http://apps.who.int/iris/bitstream/handle/10665/131056/9789241564878_eng.pdf;jsessionid=4ED87BFAD9A0FCBE9CD0FB7A6B6BAA18?sequence=8.
5. Rudatsikira, E., et al., Suicidal ideation and associated factors among school-going adolescents in rural Uganda. BMC psychiatry, 2007. 7(1): p. 67.
6. Statistics, U.B.o., The National Population and Housing Census 2014 – Main Report, Kampala, Uganda. 2016.
7. Mugisha, J., et al., Prevalence of suicidal ideation and attempt: associations with psychiatric disorders and HIV/AIDS in post-conflict Northern Uganda. African health sciences, 2016. 16(4): p. 1027-1035.
8. Ovuga, E., J. Boardman, and D. Wassermann, Prevalence of Suicide Ideation in Two Districts of Uganda. Archives of Suicide Research, 2005. 9(4): p. 321-332.
9. Wong, S.S., R.P. Ang, and V.S. Huan, Externalizing problems, internalizing problems, and suicidal ideation in Singaporean adolescents: Sex differences. Current Psychology: Developmental• Learning• Personality• Social, 2007. 25(4): p. 231.
10. Cross, C.P., L.T. Copping, and A. Campbell, Sex differences in impulsivity: a meta-analysis. Psychological bulletin, 2011. 137(1): p. 97.
11 Hawton K. Sex and suicide: Gender differences in suicidal behaviour. The British Journal of Psychiatry. 2000;177(6):484–485.
Comments are closed.