
Burden of Injuries due to Gender Based Violence in Uganda, 2011 – 2016
Authors: Biribawa Claire1, Alex Riolexus Ario1; Affiliation: 1Public Health Fellowship Program
Summary
Injuries are a major public health concern ac- counting for an enormous share of global morbidity. Gender- based violence (GBV) refers to any act that is perpetrated against a person’s will based on gender and unequal power relationships and is a significant contributor to the burden of injuries in Uganda. There is paucity of information on the bur- den of injuries due to GBV in Uganda. We therefore carried out analysis of secondary data reported through the routine Uganda Health Management Information System (HMIS) from 2011 – 2016 on injuries due to GBV. Logistic regression was used to assess trends of injuries due to GBV over the years. The highest cumulative incidence of injuries due to GBV was re- ported in 2013 at 15.3 per 100,000. The incidence of GBV has been increasing by 14% per year from 2011 – 2016 (Odds Ratio: 1.14, P-value <0.0001).
Introduction
Injuries have become a major public health concern accounting for an enormous share of global morbidity. Leading causes of injuries include road traffic crashes, violence, homicide, drowning, falls, fires and poisoning. GBV refers to any act that is perpetrated against a person’s will based on gender and unequal power relationships.
All are affected by GBV although women, girls and children are most at risk because of their vulnerability. Globally, one in four children has been physically abused and one in seventeen older people have been abused in the past month (1). GBV negatively affects one’s physical, mental, sexual and reproductive health and often leads to injuries, disability and death. Injuries resulting from GBV translate into massive medical costs with other economic losses involved due to loss of productivity (1).
In Uganda, more females report physical injuries due to GBV than males (2). The 2012 UBOS report indicted that 59.6% of the women in Uganda have ever experienced physical violence since the age of 15 years (2). Possible drivers for GBV may be weak policies, poor law enforcement, low education status, cultural beliefs, poverty, attitudes and harmful use of alcohol (3; 4; 5) and usually happens in the framework of family, community, work and institutions, places where they should be safe and protected (6; 3; 7).
There is paucity of information on the burden of injuries due to GBV in Uganda yet that data is captured in the HMIS but not analysed over the years. We therefore carried out an analysis of injuries due to GBV from 2011 to 2016 to determine the burden according to person, place and time, stimulate a deeper research on risk factors for GBV and to enhance planning and inform policies to curb GBV in Uganda.
Methods
We carried out a cross-sectional analysis of secondary data reported through the routine HMIS from 2011 – 2016 on injuries due to GBV. HMIS is a standard data collection tool used by the Ministry of Health in Uganda to collect information from patients seeking medical care from all public and private health facilities.
We extracted regional based data on injuries due to GBV and calculated cumulative incidences using 2014 Population Estimates from Uganda Bureau of Statistics. Logistic regression was used to test trends of injuries due to GBV over the years. Results were presented in tables and graphs to indicate trends of injuries due to GBV in Uganda.
Results
Burden and trends of injuries due to GBV in Uganda
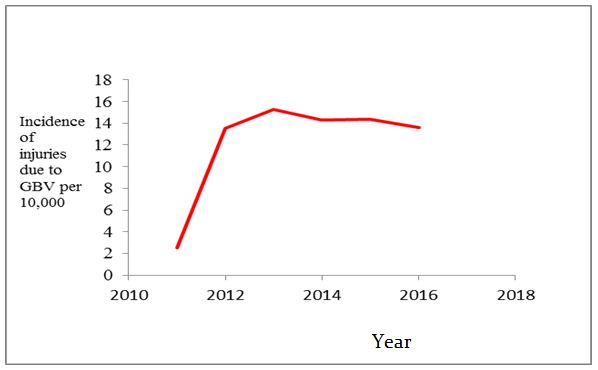
From 2011 to 2016, a total of 254,795 patients with injuries due to GBV reported in health facilities. The highest cumulative incidence was report- ed in 2013 at 15.3 per 100,000 as shown in table 1. However important to note are the very low cumulative incidence registered in 2011 at 2.5 per 10,000.
Table 1: Showing cumulative incidence over the 5 year period
| Period | Number of injuries due to GBV | Population | Rate per 10,000 |
| 2011 | 8,002 | 32,086,509 | 2.5 |
| 2012 | 44,491 | 32,935,889 | 13.5 |
| 2013 | 51,576 | 33,785,270 | 15.3 |
| 2014 | 49,542 | 34,634,650 | 14.3 |
| 2015 | 51,343 | 35,673,690 | 14.4 |
| 2016 | 49,841 | 36,593,000 | 13.6 |
The incidence of injuries due to GBV steeply increased from the year 2011, and has remained stable over the preceding years as seen in figure 1. Testing trends for injuries due to GBV using logistic regression from 2012 to 2016 showed that the trend remained constant (Odds Ratio: 1.0, P-value<0.0001). This illustrates that the incidence of injuries due to GBV has not changed from the year 2012 – 2016 and this is statistically significant.
Figure 1: Cumulative incidence of injuries due to GBV in Uganda between 2011 and 2016
Distribution of injuries due to GBV by sex
Based on the rates of 2016 and 2015, females were more affected than males although there was no significant difference between them. This is an indication that there is a significant proportion of males who are also affected by GBV as seen in table 2.
Table 2: Showing injuries due to GBV by sex
| Sex | Period | No. of injuries due to GBV | Population | Incidence per 1,000 |
| Male | 2015 | 20,777 | 17,572,657 | 1.18 |
| 2016 | 20,576 | 18,084,482 | 1.14 | |
| Female | 2015 | 30,566 | 18,101,033 | 1.69 |
| 2016 | 29,265 | 18,628,247 | 1.57 |
Trends of GBV for each region over the 5 years to 2016 for each region in Uganda
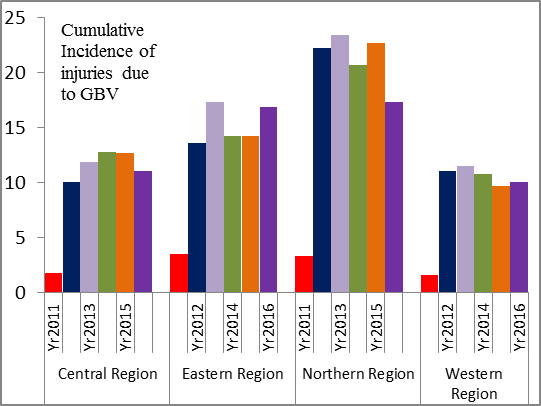
Generally over the years, the Northern and Eastern region have experienced higher rates of GBV compared to other regions. There was a sharp increase of cases from 2011 in all the regions and the rates have relatively stabilized over the preceding years as seen in figure 2.
In 2011, very low numbers of injuries due to GBV were record- ed; this could be attributed to under-reporting. The reporting rates for HMIS 105:1 was 10.6% for the indicator on injuries due to GBV for the year 2011 which is below the recommended of 90% .
The trend of injuries due to GBV has remained stable from the year 2012 to 2016, and therefore calls for a need to strategize priorities and interventions in this sector of injury prevention. There are no specific laws on GBV, although there are provisions that address it in the 1995 Constitution of Uganda, the Penal Code Act CAP 120, the Children Act CAP 59, among others, however, these have not seen much success (8).
This can be attributed to power imbalances between women and men and how GBV is deeply entrenched in some cultural practices and intimate relationships (8). The highest incidence of injuries due to GBV was reported in 2015 at 15.3 per 10,000 however, this incidence is underestimated because only a small proportion of GBV is reported to hospitals and captured in the HMIS.
Incidence of injuries due to GBV was predominant in the Northern region compared to other regions. This is similar to what was reported in the Uganda Demographic and Health Survey (UDHS) report of 2011 where the Northern and Eastern regions had higher incidences of GBV compared to other regions (9).
In the Northern region, this could be attributed to a number of factors which include; post-traumatic stress disorder due to previous rebel insecurity, insecurity in this region due to civil unrest in South Sudan leading to a number of refugees in the Northern region (UPF, 2014, UNICEF, 2014). Previous experience of violence has been documented to be a risk factor for triggering violence (3). High incidences of injuries due to GBV were also noticed in the Eastern region and this was similar to what was reported in the UDHS 2011, report.
Reasons for high incidence of GBV in the Eastern region could be attributed to the heightened level of acceptability of wife battering in this region (9). A significant proportion of males have also been affected by GBV in Uganda and so prevention and control measures should therefore be targeted towards all people and not just women and children as it is with most interventions
Conclusion
The trend of injuries due to GBV has remained stable from the year 2012 to 2016, and therefore calls for a need to strategize priorities and interventions in this sector of injury prevention. The Northern and Eastern region shared disproportionate amounts of injuries due to GBV.
Recommendations
- Prevention and control measures GBV should be targeted towards all people and not just women and children as it is with most interventions. There is thus a need to engage men and boys in GBV prevention and response.
- There is need to carry out evaluations of GBV prevention efforts and interventions in place so as to assess the existent gaps.
- There is need for continuous assessment, monitoring, and documentation of injuries due to GBV in Uganda
References
- Global status report on violence prevention 2014 . Geneva : World Health Organisation, 2014.
- The Uganda Demographic and Health Survey 2011;. Kampala, Uganda : Uganda Bureau of Statistics (UBOS) and ICF International Inc. 2012., 2012.
- Violence against women- FACT SHEET. 2016.
- Gender-based violence, alcohol use, and sexual risk among female patrons of drinking venues in Cape Town. Pitpitan, E, et , et al. 2013, Journal Behavioral Medicine, Vol. 36.
- A Situational Analysis of the State of Sexual and Gender Based Violence in IPPF Uganda With Special Focus on Health Services. Uganda: School of Women and Gender Studies, Makerere Manyire, H. 2013.
- Gender inequity in the lives of women involved in sex work in Kampala, Mbonye, M, et al., et al. s.l. : Journal of the international AIDS society, 2012, Vol. 15.
- Strengthening Health System Responses to Genderbased Violence in Eastern Europe and Central Asia: A Resource Package. 2014.
- Action for Development. Sexual And Gender Based Violence in Uganda. [Online] December 2009. [Cited: June 12, 2011.] http://menengage.org/wp-content/ uploads/2014/06/ pdf.
Comments are closed.