
Assessment of emergency medical services, Uganda, 2020–2023
Authors: Adams Kamukama1*, Benon Kwesiga1, Richard Migisha1, Alex Riolexus Ario1, Edirisa Junior Nsubuga2, Joshua Kayiwa2, Issa Makumbi2 | Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda; 2National Public Health Emergency Operations Center, Ministry of Health, Kampala, Uganda | *Correspondence: Tel: +256779314504, Email: akamukama@uniph.go.ug
Summary
Background: Emergency Medical Services (EMS) is a spectrum of urgent medical care that spans from initial prehospital critical interventions, transportation, to continued care in emergency care units. EMS play a crucial role in reducing morbidity and mortality associated with time-sensitive emergencies. In 2021, the Uganda Ministry of Health (MoH) launched the EMS policy and strategic plan to improve the quality and accessibility of EMS. It is not clear how EMS has changed since then. We analyzed EMS data from District Health Information System 2 (DHIS2) to assess trends of selected EMS indicators, Uganda, 2020–2023.
Methods: We abstracted national and regional annual and semi-annual data on EMS indicators from DHIS2. Indicators included number of patients involved in emergencies, ambulance use, assessments of consciousness, response time, post-treatment complications, and deaths at emergency units. We determined the incidence of emergencies using mid and end-year population estimates and tested the significance of trends using Mann-Kendall test.
Results: Between 2020–2023, Uganda registered an annual average number of 254,258 patients involved in emergencies, with an average incidence of 290 emergencies/100,000 population. Of these, 150,012(59%) received care at the scene, 22,883(9%) used ambulance services, 109,331(43%) were assessed for consciousness, and 203,406(80%) received care within one hour. A total of 4,831(1.9%) patients involved in emergencies developed complications within 24 hours while 45,766(18%) died. Of the deaths at emergency unit, 12,950 (41%) were attributed to medical emergencies, 7,211(23%) to road traffic injuries, 3,249 (10%) to pediatric emergencies, 3,113 (10%) to surgical emergencies, 9,104 (7%) to burns, 1,912 (6%) to obstetric/gynecological emergencies, and 1,230 (4%) to poisoning. The incidence of emergencies increased from 176/100,000 in January-June 2020 to 385/100,000 in June-December 2023 (p=0.004). There was an improvement in assessment of consciousness (29-50%, p=0.04) and reduction in mortality (27-7.9%, p=0.004) between 2020–2023.
Conclusion: We found a rising incidence of emergencies which underscores Uganda’s growing demand for reliable and functioning EMS system across the country. Despite a decline in mortality rate which could indicate improved emergency care, challenges remain in pre-hospital care and ambulance use. We recommend expanding community-based first responder programs, enhancing EMS personnel training, and improving ambulance availability and coordination.
Background
Emergency Medical Services (EMS) encompass critical life-saving medical care provided at the scene, during transportation, and in emergency units at healthcare facilities. It is characterized by rapid assessment, timely intervention, and efficient transportation to appropriate health facilities. It significantly impacts outcomes for patients with time-sensitive conditions such as communicable infections, non-communicable diseases, obstetric emergencies, and trauma (1–3).
The communicable infections requiring EMS may include sepsis, meningitis, severe pneumonia, severe malaria, and Ebola virus disease among others. Non-communicable diseases needing urgent care may include acute myocardial infarction, stroke, diabetic ketoacidosis, acute asthma attack, and pulmonary embolism. Obstetric emergencies may include conditions such as eclampsia, placental abruption, postpartum hemorrhage, uterine rupture and pre-eclampsia. Additionally, trauma conditions like traumatic brain injury, spinal cord injury, severe burns, major fractures, and penetrating injuries require prompt medical intervention to prevent significant morbidity and mortality.
In Uganda, maternal mortality was estimated at 336 deaths per 100,000 live birth in 2020 while road traffic crushes caused approximately 4,197 on site deaths in 2023(4,5).These conditions contribute significantly to the country’s morbidity, disability and mortality rates. Effective EMS can play a crucial role in reducing some of these avoidable morbidity, disability or mortality.(6,7).
Recognizing the importance of strengthening emergency care, the Ugandan Ministry of Health (MoH) formulated the EMS policy in 2021 to address existing challenges in responding to emergencies, laying the foundation for the development of a comprehensive EMS strategic plan encompassing protocols, guidelines, and standards aimed at improving the quality and accessibility of EMS across the country (8,9).
One of the primary objectives of the EMS strategic plan is to enhance the availability of quality EMS hospital care, particularly in 19 referral hospitals, 180 district hospitals, and 250 selected health center IVs by the year 2025, entailing the establishment of emergency departments/units, the development of a professional EMS workforce, and the creation of crisis centers within emergency departments across all regions of Uganda (10). It was also targeted to increase the proportion of patients involved in emergencies accessing on-scene emergency medical care to at least 50% and those receiving ambulance response within 1 hour to at least 50% by 2025.
To monitor progress and performance, the EMS strategic plan integrated key performance indicators into the District Health Information System 2 (DHIS2), a web based comprehensive Health Information Management System (HMIS) widely utilized by the MoH. These indicators provide insights into various aspects of EMS, including response times, patient outcomes, and resource utilization (10). We analyzed EMS data from District Health Information System 2 (DHIS2) to assess trends of selected EMS indicators, Uganda, 2020–2023.
Methods
Study design, data source, and study variables
We conducted a descriptive analysis of EMS surveillance data collected from the entire country using the DHIS2. These data are reported by all emergency units/departments managing patients involved in emergencies in Uganda. We abstracted six-monthly (2020 ̶ 2023) data on key EMS indicators from DHIS2. These indicators included number of patients involved in emergencies at facilities, number of patients involved in emergencies that received care at the scene of the emergency, those that arrived at the health facility in an ambulance, those assessed for level of consciousness, those accessing emergency services within one hour in an emergency unit, and those who developed complications within 24 hours after management/care. We also abstracted data on deaths at emergency units and the different causes of deaths that included medical causes, surgical causes, obstetric and gynecological causes, road traffic injuries, burns, and poisoning. We abstracted data at national and regional levels and downloaded it into Microsoft excel and cleaned it.
Data analysis
We determined the incidence of emergencies per 100,000 population using the national and regional mid and end year population estimates from 2020 ̶ 2023 from Uganda Bureau of Statistics (UBOS)(11). We determined the proportions of patients involved in emergencies assessed for level of consciousness, accessing emergency services with one hour in an emergency unit, who developed complications within 24 hours after management/care and who died at the emergency unit. We determined the proportion of the total deaths at emergency units cause by different conditions. We determined the significance of the semi-annual trends by conducting Mann-Kendall test using Stata version 14. We demonstrated the regional performance using Quantum Geographic Information System (QGIS) maps.
Ethical considerations
This study used EMS surveillance data reported by health facilities in the DHIS2 which were also aggregated with no individual patient identifiers. However, we obtained administrative clearance to use the data from the Uganda MoH. The US Centers for Disease Control and Prevention (CDC) also determined that this activity was not human subject research and its primary intent was for public health practice or disease control. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. §§See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.
Results
Annual incidence of patients involved in emergencies at health facilities, Uganda, 2020–2023
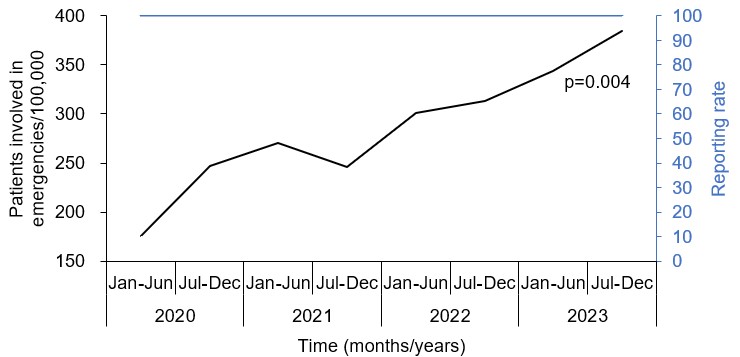
The incidence of patients involved in emergencies as reported by healthcare facilities increased from 176 patients/100,000 in January-June 2020 to 385 patients/100,000 in July-December 2023 (Table 1).
Table 1: Annual total number and incidence of patients involved in emergencies at health facilities, Uganda, 2020–2023
| Total number of patients involved in
emergencies |
Population | Incidence of patients involved in emergencies/100,000 | |
| Jan-Jun 2020 | 73,053 | 41,583,600 | 176 |
| Jul-Dec 2020 | 104,510 | 42,368,800 | 247 |
| Jan-Jun 2021 | 116,170 | 42,885,900 | 271 |
| Jul-Dec 2021 | 107,632 | 43,716,700 | 246 |
| Jan-Jun 2022 | 133,131 | 44,212,800 | 301 |
| Jul-Dec 2022 | 141,344 | 45,097,400 | 313 |
| Jan-Jun 2023 | 156,551 | 45,562,000 | 344 |
| Jul-Dec 2023 | 179,037 | 46,508,200 | 385 |
National trend of incidence of patients involved in emergencies, Uganda, 2020–2023
The incidence of patients involved in emergencies increased significantly from 176 patients /100,000 population in January–June 2020 to 385 patients/100,000 in July–December 2023 (p-value = 0.004). During this period, the reporting rate was 100% (Figure 1).
Trends of ambulance use and receiving care at the emergency scene among patients involved in emergencies, Uganda, 2020–2023
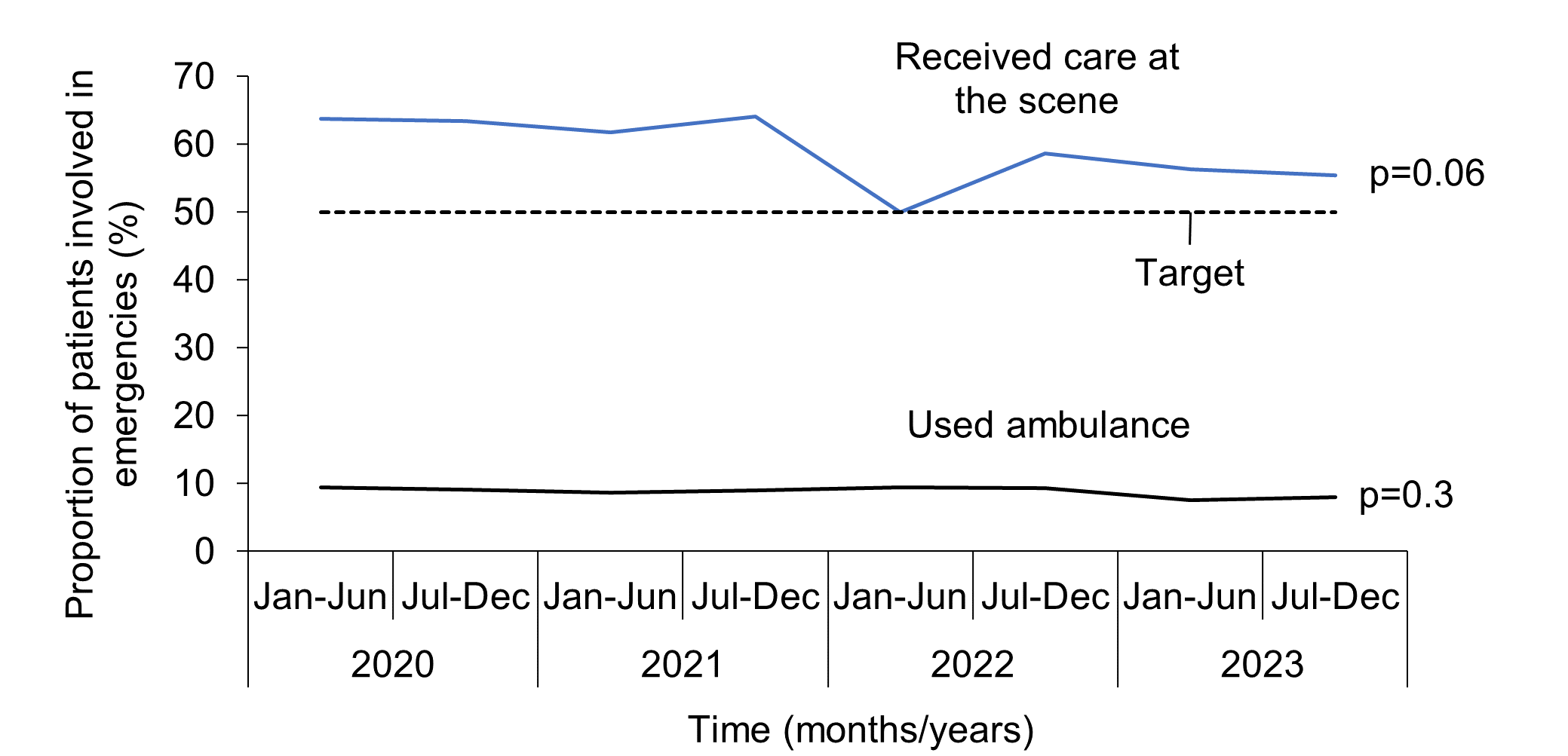
The proportion of patients involved in emergencies who arrived at the health facility in an ambulance stagnated at around 9% (p-value = 0.3) and was below the 50% target throughout the study period. The proportion of patients involved in emergencies who received care at the scene of emergency stagnated between 64-55% (p-value = 0.06) throughout the study period, but was generally above the 50% target (Figure 2).
Trends of assessment of level of consciousness and receiving care within one hour at the emergency unit among patients involved in emergencies, Uganda, 2020–2023
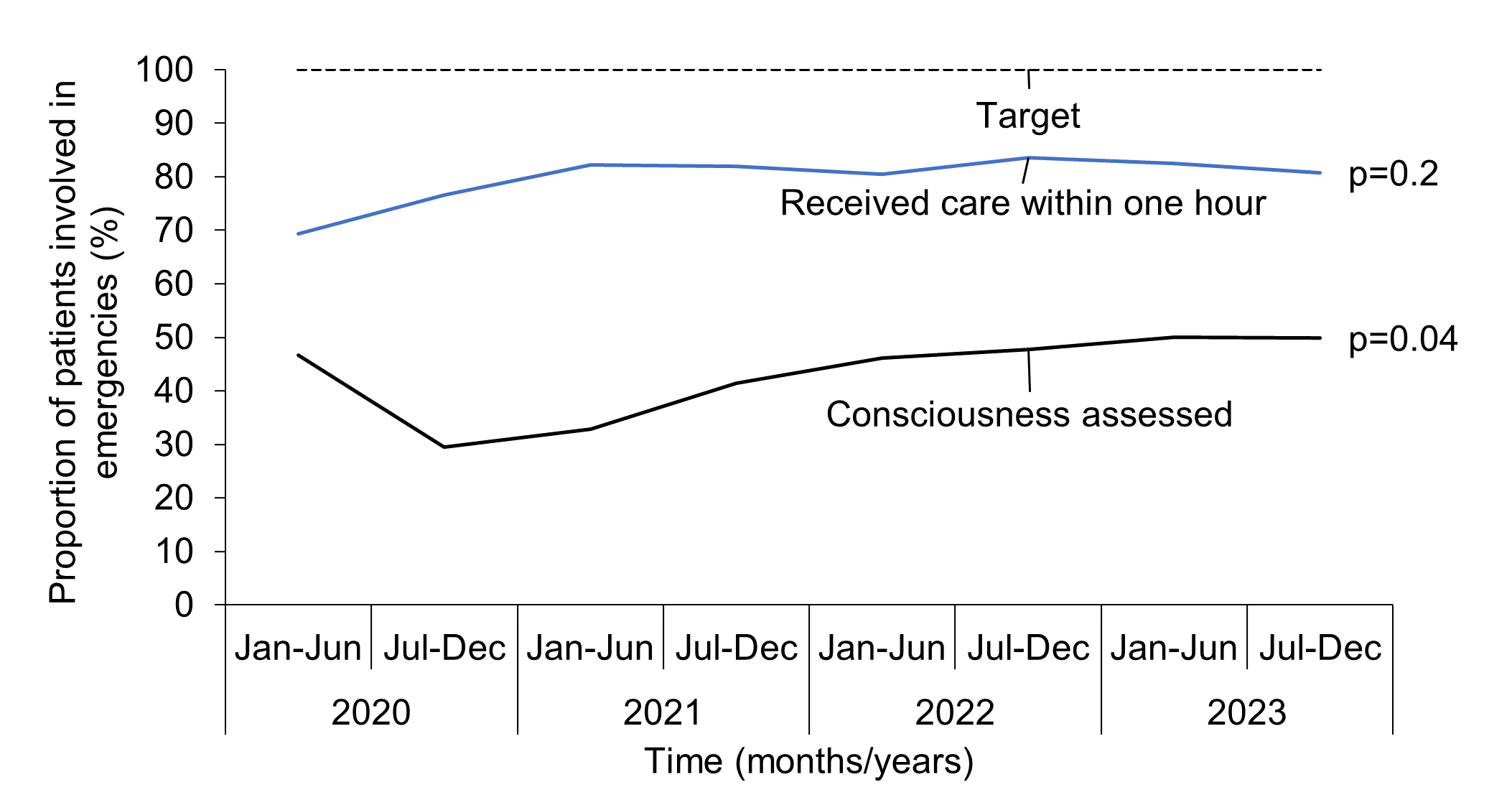
The proportion of patients involved in emergencies assessed for level of consciousness reduced from 47% in January-June 2020 to 29% in July-December 2020 and then increased significantly to 50% in June-December 2023 (p-value = 0.04). However, this was way below the 100% target. The proportion of total emergency patient who received emergency care within one hour in an emergency unit increased slightly from 69% in January-June 2020 to 81% in June-December 2023. However, this increase was nonsignificant (p-value = 0.2) (Figure 3).
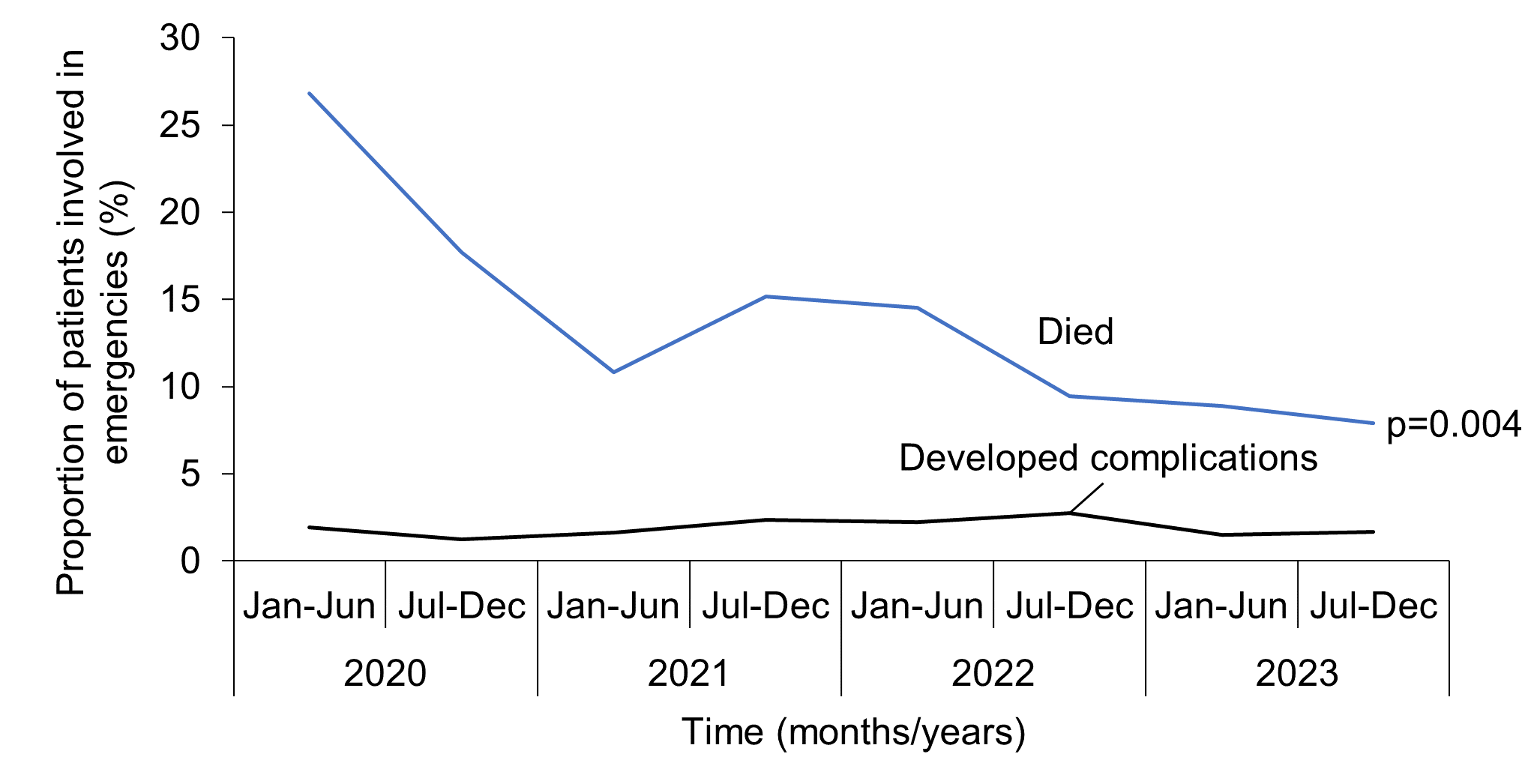
The proportion of patients involved in emergencies who developed complications within 24 hours after management stagnated between 1.9 -1.7% throughout the study period (p-value = 0.7). However, the proportion of patients involved in emergencies who died at the emergency unit decreased significantly from 27% in January-June 2020 to 8% in June-December 2023) (p-value = 0.004) (Figure 4).
Causes of death among patients involved in emergencies Uganda, 2020–2023
From 2020–2023, medical emergencies were increasingly the leading cause of death at emergency units (37-48% deaths), followed by road traffic injuries (25-20% deaths) (Table 2).
Table 2: Different causes of death at emergency departments, Uganda, 2020–2023
| Cause of death | 2020 | (%) | 2021 | (%) | 2022 | (%) | 2023 | (%) |
| Medical emergencies | 14,031 | (37) | 11,061 | (38) | 13,171 | (40) | 13,535 | (48) |
| Road traffic Injuries | 9,397 | (25) | 7,199 | (25) | 6,564 | (20) | 5,682 | (20) |
| Paediatric emergencies | 3,432 | (9) | 2,570 | (9) | 4,624 | (14) | 2,368 | (8) |
| Surgical emergencies | 3,369 | (9) | 2,933 | (10) | 3,489 | (11) | 2,662 | (9) |
| Burns | 3,237 | (8) | 2,297 | (8) | 1,958 | (6) | 1,612 | (6) |
| Obstetrics/gynaecology emergencies | 2,705 | (7) | 1,688 | (6) | 1,822 | (6) | 1,433 | (5) |
| Poisoning | 1,915 | (5) | 1,158 | (4) | 1,082 | (3) | 763 | (3) |
| Total | 38,086 | (100) | 28,906 | (100) | 32,710 | (100) | 28,055 | (100) |
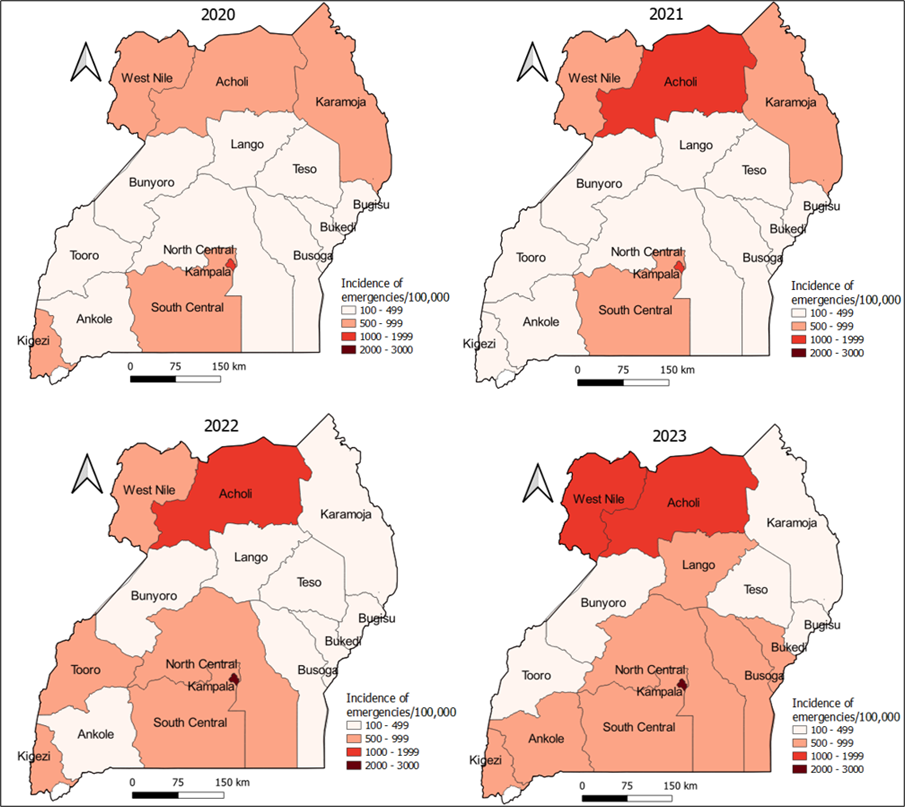
Spatial trends and distribution of emergencies, Uganda, 2020–2023
The incidence of patients involved in emergencies generally increased in all regions throughout the study period, with the highest incidence noted in Kampala Region (2,000-3,000/100,000) followed Acholi and West Nile regions (1,000-1,999/100,000) (Figure 5).
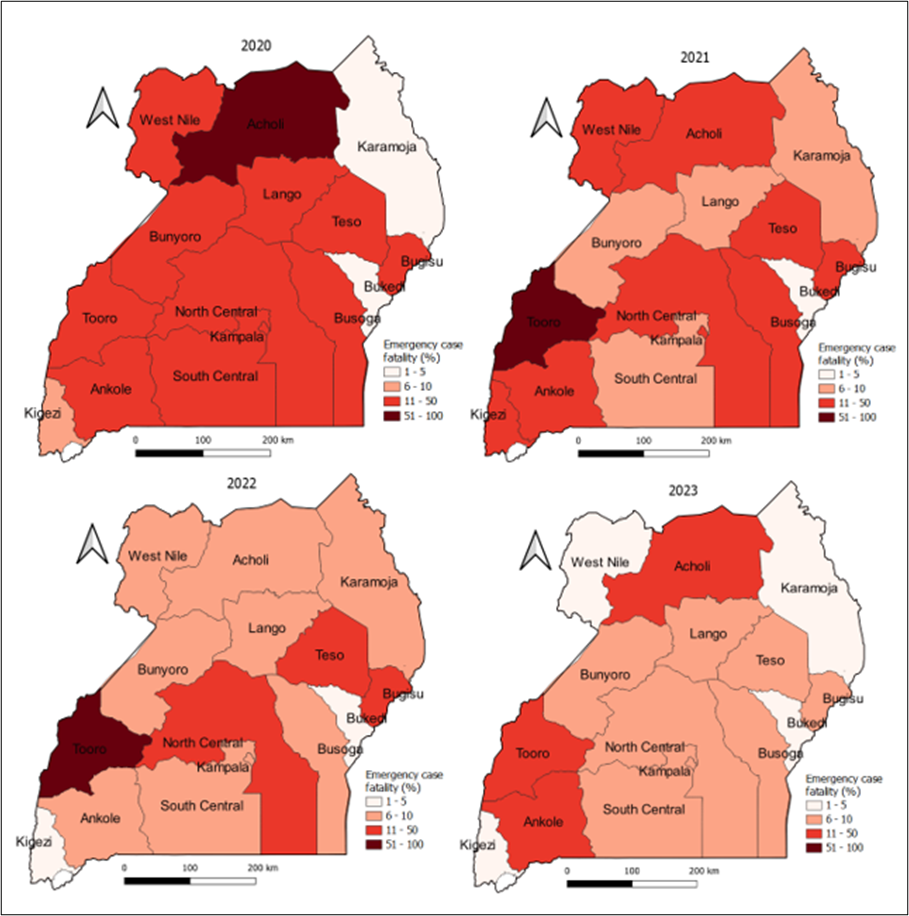
Spatial trends and distribution of mortality among patients involved in emergencies at emergency departments, Uganda, 2020–2023
The mortality among patients involved in emergencies generally reduced in all regions throughout the study period (Figure 6).
The analysis of EMS performance using Uganda’s DHIS2 from 2020–2023 revealed both encouraging progress and persistent challenges. We found a significant increase in the total number and overall incidence of emergencies across all regions, with Kampala Region exhibiting the highest incidence. The observed increase in the overall incidence of emergencies aligns with global trends reflecting growing healthcare needs and changing disease patterns (12,13). This trend is consistent with studies in low and middle-income countries where rapid urbanization and demographic shifts contribute to rising emergency healthcare demands (6). Furthermore, the regional disparities in emergency incidence, with urban centers like Kampala experiencing higher rates, resonate with previous research indicating higher healthcare utilization in densely populated areas (14).
There was a significant decrease in the proportion of patients who died at the emergency unit. This notable reduction in mortality among patients involved in emergencies across all regions suggests improvements in the quality of emergency care delivery. This finding is in line with studies emphasizing the importance of timely interventions, standardized protocols, and enhanced healthcare infrastructure in reducing mortality rates (15,16). The decline in mortality despite increasing emergency incidence underscores the effectiveness of interventions aimed at enhancing emergency care accessibility and quality nationwide.
While mortality rates decreased, certain EMS performance indicators exhibited mixed results. Despite the proportion of patients involved in emergencies accessing on-scene emergency medical care being above the 2025 target of 50%, the declining trend from 64% to 55% highlight persistent challenges in pre-hospital care. Additionally, the proportion of patients requiring emergency services who used ambulance services was way below the 2025 target of 50%. Similar findings have been reported in studies from resource-constrained settings, emphasizing the need for targeted interventions to improve pre-hospital care infrastructure and raise public awareness regarding EMS utilization (7,17).The modest improvement in the proportion of patients accessing emergency services within one-hour underscores ongoing challenges in ensuring timely care delivery. Studies have emphasized the critical importance of prompt access to care in improving patient outcomes, particularly in time-sensitive conditions such as trauma and acute illnesses (7). Addressing infrastructural limitations and strengthening referral systems could potentially mitigate delays in accessing emergency services, thereby improving patient outcomes.
Medical emergencies were consistently and increasingly the leading cause of death among patients involved in emergencies. These medical emergencies mainly include non-communicable diseases like acute myocardial infarction, stroke, diabetic emergencies, acute asthma attack, and pulmonary embolism among others. The shift towards medical emergencies as the leading cause of death underscores the evolving disease burden and the need for comprehensive emergency care beyond trauma-related conditions. This finding aligns with global epidemiological shifts towards non-communicable diseases and chronic conditions, highlighting the importance of adapting EMS systems to address diverse healthcare needs (18).
The significant increase in the total number and incidence of emergencies underscores the growing healthcare needs and changing disease patterns within the country, emphasizing the importance of adapting EMS systems to meet evolving healthcare demands. The remarkable reduction in mortality rates among patients involved in emergencies across all regions reflects improvements in the quality of emergency care delivery, highlighting the effectiveness of interventions aimed at enhancing accessibility and standardizing care protocols. However, challenges persist in certain EMS performance indicators, such as the decline in patients receiving care at the scene and the stagnation in ambulance utilization. Additionally, the shift towards medical emergencies as the leading cause of death underscores the need for comprehensive emergency care beyond trauma-related conditions.
While our study provides valuable insights into the performance of EMS in Uganda, several limitations should be considered when interpreting the results.
Firstly, analysis relied on data abstracted from the DHIS2 where the accuracy and completeness of the data depend on the quality of reporting by healthcare facilities. Variability in reporting practices, missing data points, incomplete records and data entry errors could bias our analysis and limit the comprehensiveness and reliability of our findings.
Secondly, we were not able to comprehensively assess the in-hospital emergency care because some key indicators like number of patients with hypoxia who received oxygen and number of patients with hemorrhage controlled lacked denominators.
Additionally, the study focused on key EMS indicators available in DHIS2, but other important independent variables, such as pre-hospital care practices, ambulance fleet capacity, and healthcare provider training levels, were not assessed. The absence of these variables may limit the comprehensiveness of the assessment of EMS performance.
Based on the findings and limitations of our study, the following recommendations are proposed to enhance the effectiveness and efficiency of EMS in Uganda.
The MoH needs to improve the EMS data quality and completeness of reporting through regular training, capacity building, and monitoring.
The MoH needs to address the challenge of ambulance inaccessibility. This could involve expanding ambulance fleets, optimizing ambulance deployment strategies, and raising public awareness about the availability of ambulance services.
The MoH needs to invest in infrastructure, human resources, and logistical support to reduce response times and ensure timely access to emergency care.
The MoH needs to promote the adoption of standardized clinical assessment protocols, such as the Glasgow Coma Scale (GCS), to ensure consistent and accurate evaluation of patients’ level of consciousness. Provide training and resources to healthcare providers to enhance their proficiency in conducting clinical assessments in emergency settings is essential.
The MoH needs to tailor EMS investments according to regional needs. For example, Kampala region that reported highest incidence of emergencies throughout the study period deserves the highest EMS investment.
The MoH could consider capturing data on number of patients involved in emergencies with hypoxia and number of patients involved in emergencies with hemorrhage so as to provide an appropriate denominator for oxygen use and hemorrhage control.
The authors declare that they have no conflict of interest.
Authors’ contributions
AK participated in the conception, design, analysis, interpretation of the study and wrote the draft bulletin. BK, RM, EJN, JK, IM reviewed the report and the drafts of the bulletin for intellectual content and made multiple edits to the draft bulletin; BK and ARA reviewed the final bulletin to ensure intellectual content and scientific integrity. All authors read and approved the final bulletin.
Acknowledgement
We thank the staff of the Uganda Public Health Fellowship Program and Uganda Public Health Emergency Operation Center for the technical support and guidance offered during this work. We also thank the US-CDC for supporting the activities of the Uganda Public Health Fellowship Program under which this work was done.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source; however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Oc K, Aa H, D B, Er H, C M, M J. Emergency medical systems in low- and middle-income countries: recommendations for action. Bulletin of the World Health Organization [Internet]. 2005 Aug [cited 2024 Mar 18];83(8). Available from: https://pubmed.ncbi.nlm.nih.gov/16184282/
- Emergency care [Internet]. [cited 2024 Mar 6]. Available from: https://www.who.int/health-topics/emergency-care#tab=tab_1
- Razzak JA, Kellermann AL. Emergency medical care in developing countries: is it worthwhile? Bull World Health Organ. 2002;80(11):900–5.
- UNFPA Uganda [Internet]. 2021 [cited 2024 Jul 22]. Promising results in reducing maternal deaths. Available from: https://uganda.unfpa.org/en/news/%C2%A0promising-results-reducing-maternal-deaths
- Kamusiime W. ANNUAL CRIME REPORT 2023 [Internet]. Uganda Police Force. 2024 [cited 2024 Jul 22]. Available from: https://www.upf.go.ug/annual-crime-report-2023/
- Mould-Millman NK, Dixon JM, Sefa N, Yancey A, Hollong BG, Hagahmed M, et al. The State of Emergency Medical Services (EMS) Systems in Africa. Prehospital and Disaster Medicine. 2017 Jun;32(3):273–83.
- Z O, S A, M M, S S, Sr K, La W, et al. Emergency care in 59 low- and middle-income countries: a systematic review. Bulletin of the World Health Organization [Internet]. 2015 Aug 1 [cited 2024 Mar 18];93(8). Available from: https://pubmed.ncbi.nlm.nih.gov/26478615/
- NATIONAL EMERGENCY MEDICAL SERVICES POLICY.pdf.
- MoH Strategic Plan 2020_25.pdf [Internet]. [cited 2024 Mar 18]. Available from: http://library.health.go.ug/sites/default/files/resources/MoH%20Strategic%20Plan%202020_25.pdf
- 16184282.pdf [Internet]. [cited 2024 Mar 18]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2626309/pdf/16184282.pdf
- Explore Statistics [Internet]. Uganda Bureau of Statistics. [cited 2024 Sep 14]. Available from: https://www.ubos.org/explore-statistics/
- World Health Organization. Health emergency and disaster risk management framework [Internet]. Geneva: World Health Organization; 2019 [cited 2024 Mar 29]. Available from: https://iris.who.int/handle/10665/326106
- EMS WHO.pdf.
- The Global Network Maternal Newborn Health Registry: a multi-country, community-based registry of pregnancy outcomes | Reproductive Health | Full Text [Internet]. [cited 2024 Mar 29]. Available from: https://reproductive-health-journal.biomedcentral.com/articles/10.1186/s12978-020-01020-8
- Global Burden of Surgical Conditions – Essential Surgery – NCBI Bookshelf [Internet]. [cited 2024 Mar 29]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK333518/
- Murad MK, Husum H. Trained lay first responders reduce trauma mortality: a controlled study of rural trauma in Iraq. Prehosp Disaster Med. 2010;25(6):533–9.
- Kobusingye OC, Hyder AA, Bishai D, Hicks ER, Mock C, Joshipura M. Emergency medical systems in low- and middle-income countries: recommendations for action. Bull World Health Organ. 2005 Aug;83(8):626–31.
- Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014 Jan 30;123(5):615–24.
Comments are closed.