
Malaria Outbreak Facilitated by Increased Vector Breeding Sites sustained by Intermittent Rainfall: Mbale District, Uganda, June 2019
Author: Gloria Bahizi1, Daniel Kadobera1, Fred Monje1, Benon Kwesiga1, Alex Riolexus Ario1 Author: Affiliations: 1Uganda Public Health Fellowship Program, Ministry of Health, Kampala, Uganda
Summary
In June 2019, the Ministry of Health’s National Malaria Control Program received notification of an increase in malaria cases in Mbale District, Uganda which exceeded the action thresholds. The most affected sub-counties were Bumbobi and Nyondo located in the midlands. We investigated to assess the out break’s magnitude, identify transmission risk factors, and recommend evidence-based control measures. We defined a confirmed case as a positive malaria result using mRDT or microscopy from 1 January 2019 to 30 June 2019 in a resident or visitor of Bumbobi or Nyondo sub-county in Mbale District, Uganda. Cases were found by reviewing out patient registers in health facilities and a matched case control study was conducted. We identified 8,827 case-persons (overall attack rate [AR]=33%). Females (AR=36%) were more affected than males (AR=27%). The 5-18-year age-group (AR=26%) was the most affected. The area had intermittent rainfall patterns from January with short spells of no rainfall; the propagated outbreak began in epidemiologic week 10 in March 2019. In the case-control study, 52% (74/143) case-patients and 5.5% (4/73) controls had artificial soil erosion control pits near their homes which held stagnant water for several days following rainfall (AOR=16, 95%CI=4.0-61); 23% (11/47) of case-patients and 67% (72/108) of controls wore long-sleeve clothes during evening hours (AOR=0.19, 95%CI=0.076-0.45); 6.7% (7/104) of case-patients and 30% (41/138) of controls slept under a bed-net (AOR=0.16, 95%CI=0.016-1.7. Entomological assessment indicated active breeding sites; Anopheles gambiae species were the predominant vector. We recommend draining of erosion pits immediately after the rain and educating communities on malaria prevention measures.
Introduction
Malaria is one of the leading causes of disease and death in the world. Globally, it is estimated that 3.4 billion people are at risk of being infect- ed with malaria and developing disease. According to the World Health Organization report of 2018, malaria caused nearly 219 million cases and 445,000 deaths with an estimated 90% deaths in 2016 being in the WHO African Region 1.
Malaria occurs mostly in tropical and subtropical areas of the world. Africa is the most affected due to a combination of factors such as the presence of the Anopheles mosquito which is responsible for the high transmission and the spread of the Plasmodium falciparum which causes malaria. Malaria transmission in Uganda exhibits seasonality which follows the rainfall pattern.2
The weather conditions allow the vector to thrive hence transmission occurs all year round with the presence of breeding sites and favorable temperatures. In Uganda, Malaria is endemic in approximately 95% of the country, affecting over 90% of the population and is listed as the sixth leading cause of death 3. We investigated to assess the outbreak’s magnitude, identify transmission risk factors, and recommend evidence-based control measures.
Methods
We defined a confirmed case as a positive malaria result using mRDT or microscopy from 1 January 2019 to 30 June 2019 in a resident or visitor of Bumbobi or Nyondo sub-county in Mbale District, Uganda. We re- viewed outpatient registers in health facilities of the two most affected sub counties. We described the case-persons by person, place, and time. Environmental and entomological assessments of the most affected villages in the sub counties were done. We generated hypotheses and conducted a case control study to compare exposures among cases and controls, frequency matched by age and village with a ratio of 1:1.
Results
We identified 11,598 confirmed case-persons in the two most affected sub-counties. Overall attack rate was 33%. Bumbobi sub-county was more affected (AR = 38/100) than Nyondo sub-county (AR = 24/100). Females (AR= 36%) were more affected compared to the males (AR= 27%). The 5-18-year age group was most affected AR: 26, followed by children under 5 years (AR: 23)
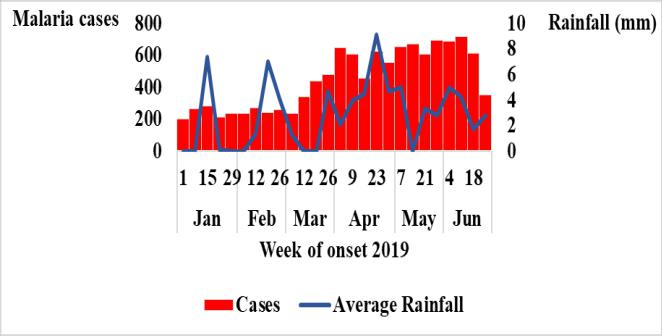
The epidemic curve showed a continuous increase in malaria cases from Mar 2019. The rainfall pattern plotted against the epi-curve shows erratic seasonality coupled with no rain. This was a propagated outbreak sustained by the intermittent rain- fall.
Hypothesis generation interviews
Hypothesis generating interviews found 95% of households had mosquito nets but 71% reported them being torn and had had a sick household member two weeks before onset, 89% had erosion control pits. We hypothesized that the malaria outbreak was associated with erosion control pits which held stagnant water for periods after rainfall.
Environmental assessment and entomological findings
Erosion control pits, ditches near the homes, stagnant water, and improper use of drainage system were observed. There were larvae of anopheles mosquitoes in observed stagnant water. All households had at least one LLINs in their house. Ninety four percent of the cases had LLINs however, among those who used and those who did not use LLINs, most of them re-ported mosquito nets as sources of bedbugs. The pyrethrum spray catch (PSC) yielded 37 Anopheles gambiae of which 65% were fed, 8 Anopheles funestus with all fed, and 362 culex mosquitoes.
Case-control findings
Fifty two percent of case-patients(74/173) and 5.5% (4/73) of controls had erosion control pits near the homes and gardens (AOR=16, 95%CI=4.0-61) two weeks before symptom onset; 69%(94/102) of case-patients had a sick household member compared 38%(5/13) of the controls AOR=15, 95%CI=5.6-40.9) two weeks before symptom onset. Sixty three percent (49/79) case-patients compared to 40% (20/50) controls had bed bugs on mosquito nets (AOR=2.6 95% CI=1.07-6.4). Sleeping under an insecticide treated mosquito net (AOR=0.16, 95%CI=0.016-1.7) and wearing long clothes in the evenings (AOR=0.19, 95% CI=0.076-0.45); 6.7% (7/104) reduced the odds of malaria infection.
Discussion
This malaria outbreak was facilitated by increased vector-breeding sites sustained by intermittent rainfall. The time of the malaria transmission coincided with the rainfall season in Mbale District which has a bimodal pattern for March to June and September to November 4. Mbale has a topographical make-up of mountainous (highlands) with steep terrain combined with high rainfall and unstable soils, midlands, and the lowlands which make it vulnerable to impact of climate change. Our study highlighted presence of erosion control pits filled with stagnant water in the affected areas that increased breeding sites. The intermittent rainfall also sustained a conducive environment for mosquitos and was associated with this outbreak as documented elsewhere7. Our study found that people found close to these pits were 16 times more affected than those who lived far from them. This finding is also supported by a report from Afar, Ethiopia8. The affected villages are situated in the midlands characterized with fertile soils and farming. As main source of livelihood. Whilst beneficial for crops and domestic water use, rainfall in the wet seasons can be expected to increase erosion, especially on steep slopes, as well as flooding in valleys and siltation of streams and rivers. In order to preserve their soil and prevent soil erosion, erosion control pits are dug in the midlands to reduce the speed of runoff. Other modifications included ditches that also preserved water for farming.
Age group of 5–18 years and females were most affected. Similar studies done in India5, Ethiopia, 6and Zimbabwe 8 showed children and females were more attacked by malaria. This may be explained by children having lower immunity and adult women carrying out activities such as cooking late in kitchens detached from the house and taking care of animals that exposed them more to mosquito breeding sites.
Our study revealed mosquito net use being protective against malaria infection but this did not show a significant effect on malaria infection. This is consistent with a study in Haiti which assessed the effectiveness of ITNs after a mass distribution. 12 LLINs are frequently used but those in use were in a poor state with visible holes reported by 49% of the cases, poorly hanged or shared by many members of the household. This was also high-lighted in Somalia where there was no difference in bed net use among the different groups of people in communities 13. It was observed that in some households bed nets were not hung be-cause people believed they brought bedbugs. Mosquito nets impregnated with a long-lasting pyrethroid insecticide were found to be effective in repelling and killing bedbugs14. Bed bugs came out of hiding places and for those that wrapped the mosquito nets around the mattress, they would be seen at the top; in others. The presence of bedbugs on LLINs showed an odds of 2.6 of malaria infection compared to those that did not report having seen bed bugs on their mosquito nets. Other protective measures were wearing long clothes when out late in the evenings and having curtains on doors and windows as these minimize human-vector contact. These are strategies that can be incorporated into behavioral change communication to prevent malaria infection as sup-ported by studies done elsewhere in Kenya15,16.
Conclusions and recommendations
Presence of erosion control pits was significantly associated with the occurrence of malaria outbreak. Lack of awareness on malaria transmission and control highlighted by the belief that mosquito nets brought bedbugs also created laxity on preventive measures. We recommend removal of potential mosquito breeding sites and draining of erosion pits regularly. Community awareness on malaria prevention and control mechanisms should be done. Adequate knowledge about malaria is paramount for the correct application of preventive measures and decreasing the disease exposure.
References
- World Health Organization. World Malaria Report. (2018). Available at: www.who.int/malaria. (Accessed: 22nd July 2019)
- Kilian, A., Langi, P., Talisuna, A. & Kabagambe, G. Rainfall pat-tern, El Niño and malaria in Uganda. Transactions of the Royal Society of Tropical Medicine and Hygiene 93, 22–23 (1999).
- National Malaria Control Programme & Abt Associates. An epidemiological profile of malaria and its control in Uganda. (2013).
- Mbogga, M. S. Climate profiles and climate change vulnerabil-ity assessment for the Mbale region of Uganda. UNDP Consultancy report. Kampala, Uganda (2012).
- Rana: A report on outbreak investigation of malaria… – Google Scholar.
- Workineh, B., Mekonnen, F. A., Sisay, M. & Gonete, K. A. Ma-laria outbreak investigation and contracting factors in Simada District, Northwest Ethiopia: a case–control study. BMC Res Notes 12, 1–6 (2019).
- G. Prevalence and risk factors of malaria… – Google Scholar. Available at: https://scholar.google.com/scholar? oi=gsb95q=Dawit.%20G.%20Prevalence%20and%20risk%20factors% 20of%20malaria%20in%20Ethiopia%3B%202012.&lookup=0&hl=en. (Accessed: 6th September 2019)
- Debela MB, Kahsay AB, Mokonnon TM. Malaria outbreak… – Google Scholar. Available at: https://scholar.google.com/scholar? hl=en&as_sdt=0%2C5&q=Debela+MB%2C+Kahsay+AB% 2C+Mokonnon+TM.+Malaria+outbreak+and+contracting+factors+in+Afar+Region%2C+Ethiopia.+J+
Public+Health+Epidemiol.+2018% 3B10%287%29%3A233%E2%80%9340.&btnG=. (Accessed: 6th September 2019)
- Community perspectives on treating asymptomatic infections for malaria elimination in The Gambia | Malaria Journal | Full Text. Available at: https://malariajournal.biomedcentral.com/ articles/10.1186/s12936-019-2672-7. (Accessed: 6th September 2019)
- Kateera, F. et al. Malaria parasite carriage and risk determinants in a rural population: a malariometric survey in Rwanda. Malaria journal 14, 16 (2015).
Comments are closed.