
Chickenpox outbreak fueled by lack of vaccination and congestion among pupils in school X, Kampala City, Uganda, August 2025
Authors: Michael Mutegeki1*, Justine Wobusobozi1, Amina Namwabira1, Tracy Rutogire1, Esther Nabatta1, Benon Kwesigwa1, Richard Migisha1, and Bernard Lubwama2, Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda 2Department of Integrated Epidemiology, Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda Correspondence*: Tel: +256 787882985, Email: mutegekim@uniph.go.ug
Summary
Background: In July 2025, an unusual febrile rash illness was reported among pupils at a primary school X in the Greater Kampala Metropolitan Area (GKMA). We investigated to determine the cause and magnitude of the outbreak, identify exposures to inform evidence-based prevention and control measures.
Methods: We defined a case as onset of papular, vesicular, or papulovesicular rash in a pupil of school X from 1st July–30th August 2025. We conducted active case search among all pupils at school X and collected data on clinical, demographic and exposure variables using an electronic case investigation form administered to parents or guardians. We conducted an environmental assessment focusing on classroom ventilation, crowding, shared play and resting areas. Laboratory samples from the first nine cases were tested at the Uganda Virus Research Institute using polymerase chain reaction for varicella-zoster virus (VZV), Mpox virus, measles, rubella, and enteroviruses using national standard operating procedures. We conducted descriptive epidemiology (proportions and attack rates by age group, sex and class).
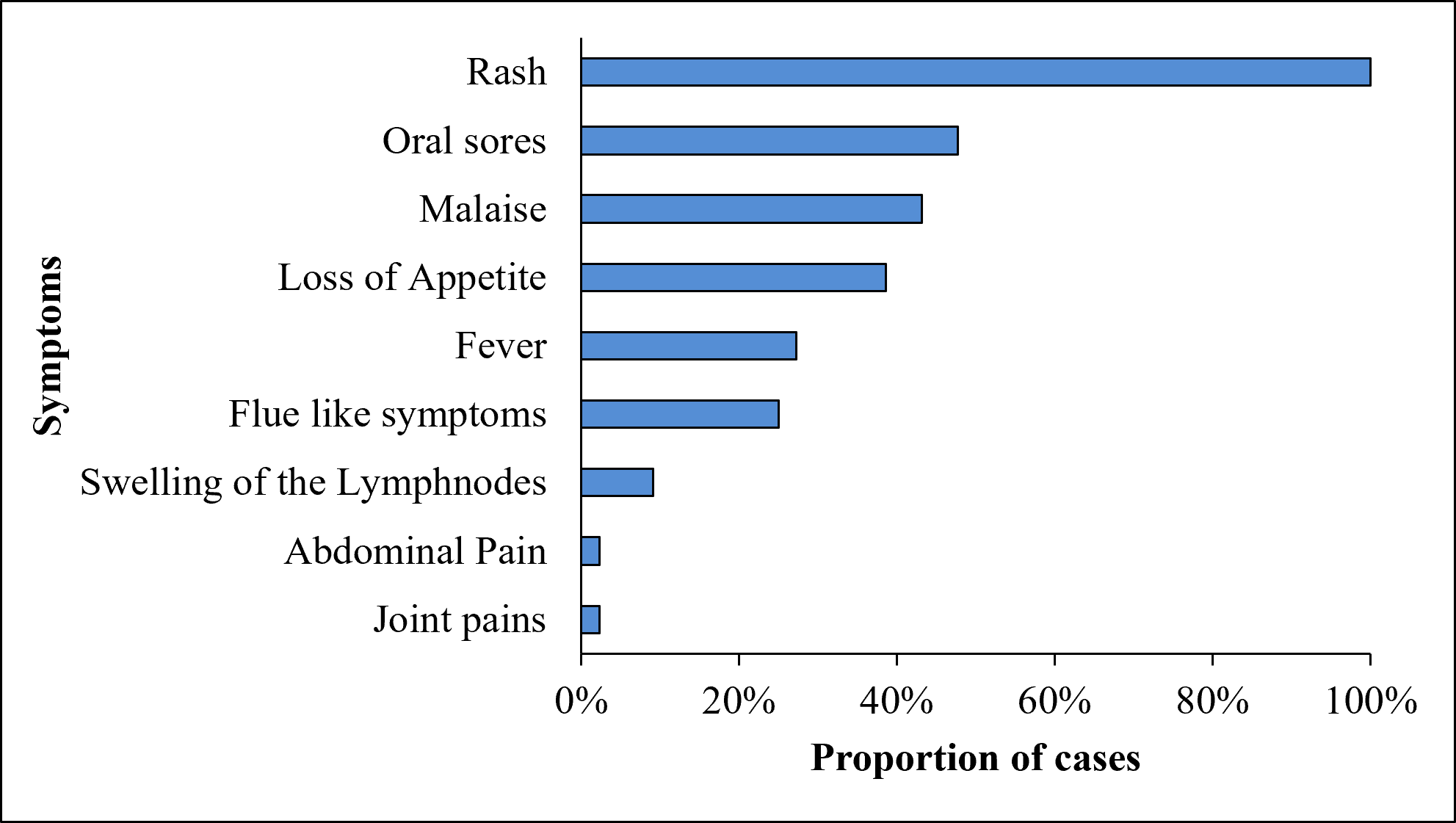
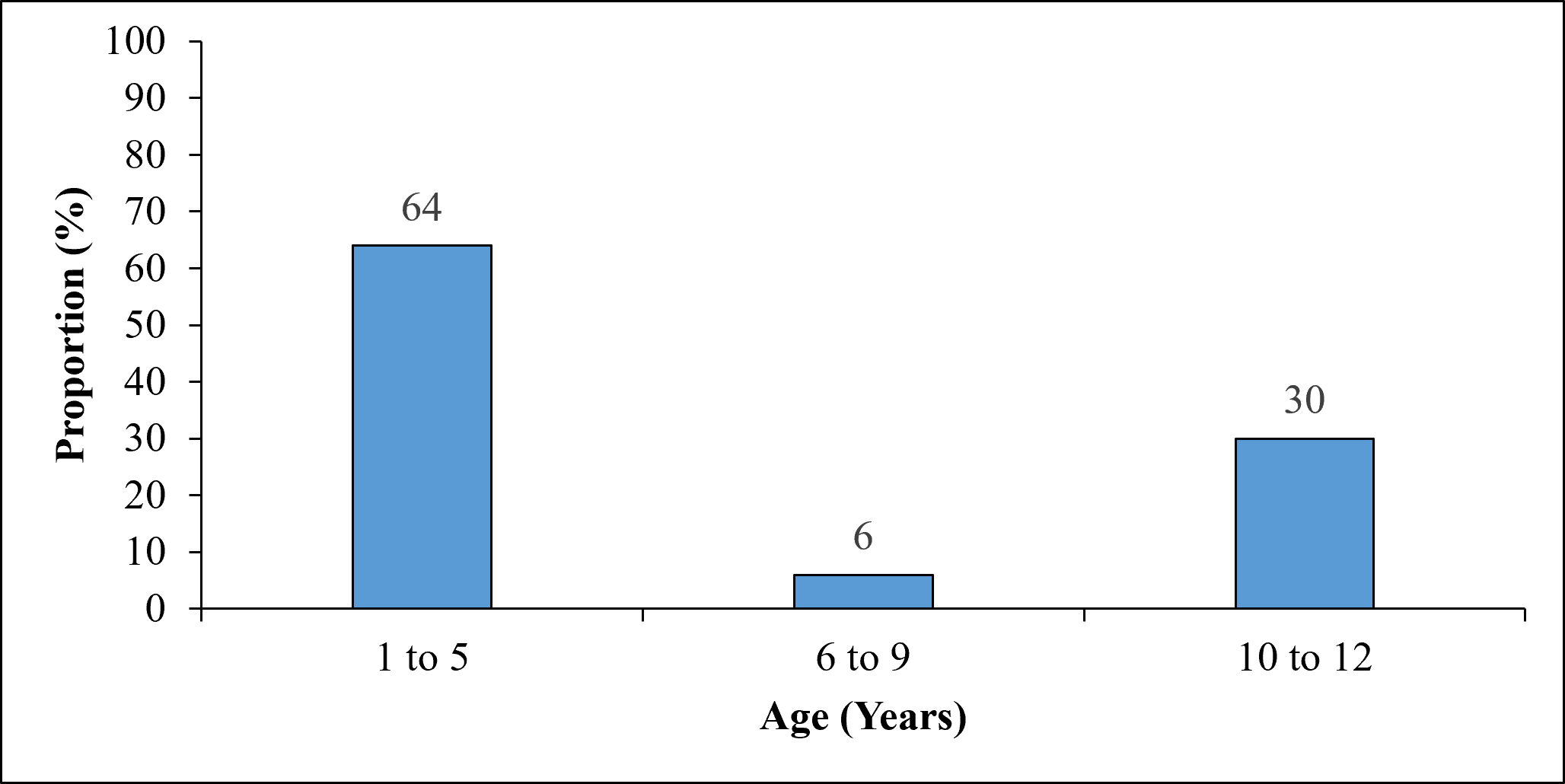
Results: From a school of 780 pupils, we identified 44 cases with no deaths yielding an overall attack rate (AR) of 56.4 per 1,000 pupils. All (100%) of cases were not vaccinated against VZV. The median age of cases was 4 (IQR: 3-8 years). Males (AR=57.8/1,000) and females (AR=54.8/1,000) were similarly affected. Kindergarten pupils were the most affected (AR=112/1,000). All (100%) cases presented with an itchy rash. The rash appeared on the hands in 41/44 (93%) and on the feet in 27/44 (61%) of cases. Papulo-vesicular type of rash was present in 25/44 (56%) of cases. We found 17/44 (39%) of cases had an affected household member. We observed 25/44 (56%) of cases shared sleeping and play spaces. Laboratory testing identified 2/9 (22%) varicella-positive cases and all 9 samples tested negative for measles, rubella, and Hand Foot and Mouth Disease (HFMD).
Conclusion: This was varicella zoster (chickenpox) with atypical clinical presentation fueled by lack of VZV vaccination and sharing of napping spaces among kindergarten pupils. Implementing daily screening of children and minimizing shared sleeping or napping spaces may support early case identification and help prevent further spread of the illness.
Background
Acute febrile illnesses accompanied by rash are common among children and represent a frequent cause of outbreaks in school settings (1). In low- and middle-income countries, including Uganda, such presentations pose diagnostic and public health challenges because several viral and non-viral conditions share overlapping clinical features. Common childhood illnesses characterized by fever and rash include measles, rubella, varicella (chickenpox), hand, foot and mouth disease (HFMD), parvovirus infection, adenoviral infections, and allergic or bacterial skin conditions (2).
Varicella Zoster Virus (VZV) is one of the frequent causes of exenthematous outbreaks among school children (1). It is highly contagious but usually self-limiting, predominantly affecting young children (1). Transmission of VZV is primarily acquired through the airborne route. Aerosolized VZV virions from lesions infect new hosts via the respiratory tract, almost exclusively in persons who have not had varicella or been vaccinated against the disease (2). Exposure has most commonly occurred from other persons with varicella but can also be from persons with herpes zoster rash (3,4). A primary viremia develops 4–6 days later, and approximately 14–16 days (range 10–21 days) after exposure, the onset of rash occurs. The infection manifests as a generalized, pruritic, maculopapular and vesicular rash, typically consisting of 250 to 500 skin lesions surrounded by an erythematous base (3).
Although VZV infections in children are often mild and resolve within 21 days, outbreaks in congregate settings such as schools can result in rapid transmission and significant absenteeism, cause anxiety and embarrassment. In rare cases, these cases can be associated with complications including aseptic meningitis, encephalitis, and acute flaccid paralysis (7). Therefore recognition of their common and atypical presentations is necessary to differentiate them from other skin conditions of similar morphology (8).
In July 2025, School X in the Greater Kampala Metropolitan Area (GKMA) reported an unusual rise in children presenting with an itchy rash, oral ulcers and fever. The Ministry of Health together with Kampala City Authority, initiated an investigation to determine the magnitude of the illness and recommend evidence-based prevention and control measures.
Methods
The outbreak occurred at a Primary School X in Ntinda Parish, Nakawa Division, Kampala, a mixed day and boarding school with 780 kindergarten and primary pupils. We defined a case as the onset of a papular, vesicular, or papulovesicular rash in a pupil between 1 July and 30 August 2025. We conducted active case search among all pupils and collected demographic, clinical, vaccination and exposure information from parents or guardians using an electronic case investigation form administered with support from school staff. Descriptive analysis was conducted by age, sex, clinical presentation and class. We also calculated attack rates using enrollment data obtained from the school administration. An environmental assessment was conducted to evaluate pupil density, shared play and resting areas and the availability of health education materials. We also collected laboratory samples including whole blood, lesion and oropharyngeal swabs from the first nine consenting cases and tested at the Uganda Virus Research Institute for Mpox virus, varicella-zoster virus, measles, rubella, enteroviruses and picornaviruses using standard national laboratory protocols.
This investigation was undertaken as part of a Ministry of Health and Kampala Capital City Authority outbreak response. The CDC Uganda Office of the Associate Director for Science determined that the activity constituted public health practice rather than human subjects research. Permission was obtained from the school administration, and verbal informed consent was secured from parents or guardians before interviews.
Results
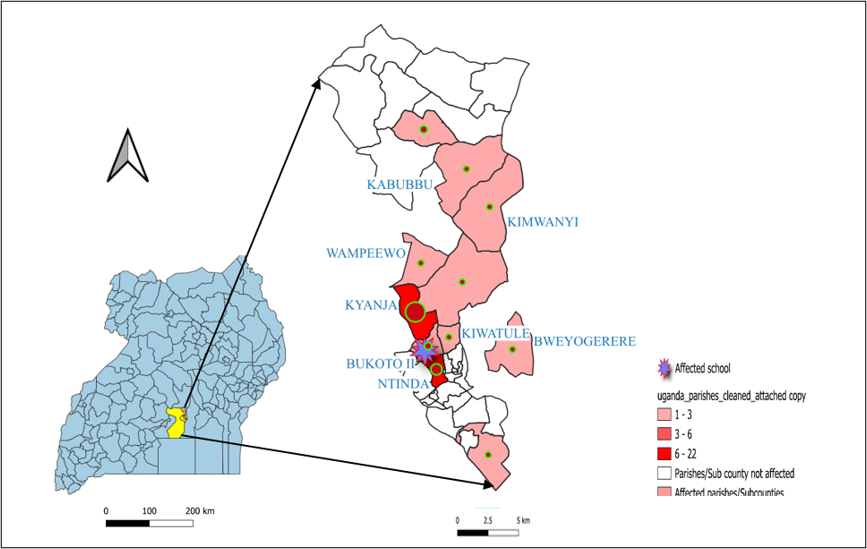
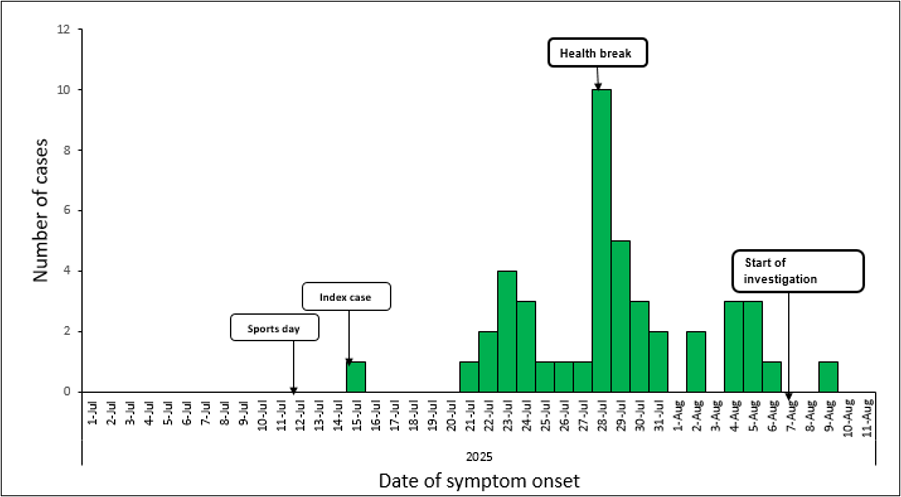
We identified 44 cases with no deaths yielding an overall attack rate (AR) of 56.4/1,000 pupils (Table 1). All (100%) of cases were not vaccinated against VZV. The median age of cases was 4 (IQR: 3-8 years) with 28/44(64%) in the 1-5year age category (Figure 2). Males (AR=57.8/1,000) and females (AR=54.8/1,000) were similarly affected (Table 1). Kindergarten pupils were the most affected (AR=112/1,000) (Table 1). All (100%) cases presented with a rash (Figure 1). The rash appeared on the hands in 41/44 (93%) and on the feet in 27/44 (61%) of cases. Papulo-vesicular type of rash was present in 25/44 (56%). We found 17/44(39%) of cases had an affected household member. Most cases originated from Ntinda and Kyanja parishes in Nakawa Division (Figure 3). Cases peaked in July and started to decline after the health break (Figure 4).
Table 1: Cases identified during the investigation of a chickenpox outbreak in school X, Greater Kampala Metropolitan Area, disaggregated by class and sex, August 2025
| Characteristic | No. of Pupils | No. of cases | AR/1000 |
| Class | |||
| Kindergarten | 242 | 27 | 112 |
| P.1 | 90 | 3 | 33.3 |
| P.2 | 88 | 3 | 34.1 |
| P.3 | 80 | 3 | 37.5 |
| P.4 | 91 | 5 | 54.9 |
| P.5 | 76 | 3 | 39.5 |
| P.6 | 52 | 0 | 0.0 |
| P.7 | 61 | 0 | 0.0 |
| Sex | |||
| Males | 398 | 23 | 57.8 |
| Females | 382 | 21 | 54.8 |
| Total | 780 | 44 | 56.4 |
Environmental assessment: We observed shared resting and play stations, and kindergarten children shared common napping spaces. There were no health promotion visuals, such as posters, to reinforce hygiene practices.
Laboratory results: Of the nine samples collected, 2/9 tested positives for chickenpox and all samples tested negative for viruses that cause measles, rubella, and HFMD.
Discussion
This investigation described a school-based outbreak of a febrile rash illness among primary school children in the Greater Kampala Metropolitan Area. The findings collectively describe a viral exanthematous due to Varicella zoster (Chicken pox) with all children not vaccinated against VZV. This is consistent with previous studies where VZV affect exclusively non vaccinated individuals (4,6).The outbreak primarily affected children aged 1–5 years especially those in kindergarten. This age distribution aligns with global and regional literature showing that the viral exanthematous illness primarily affects preschool-aged children due to limited prior immunity and close-contact behaviors common in early childhood settings (7,8). Similar age-specific clustering has been reported in school and daycare outbreaks in Asia and Europe, where attack rates are consistently highest among children under 10 years (9). The absence of cases in upper primary classes likely reflects reduced susceptibility, better hygiene practices and less frequent close physical contact among older pupils.
Clinically, all cases presented with rash, with predominant involvement of the hands and feet and limited trunk involvement. The predominance of papulo-vesicular and papular lesions, associated with pruritus and oral sores in nearly half of cases does not mirror classic VZV presentations described in the literature. In contrast, varicella typically presents with generalized trunk-predominant vesicular rash occurring in multiple stages, a pattern observed in only a minority of cases(10). However atypical presentations have been documented(11). This could suggest mixed viral etiologies as seen in some studies (12).
Household transmission was observed in nearly two-fifths of cases, particularly involving pre-school siblings, underscoring the high transmissibility of viral rash illnesses and the role of households in sustaining transmission beyond school settings. Similar household secondary attack rates have been reported in Varicella and HFMD outbreaks, especially where young children share caregivers and sleeping spaces (13).
The epidemic curve demonstrated a gradual rise and peak followed by decline after a school health break, suggesting propagated person-to-person transmission with interruption following reduced contact. This temporal pattern is characteristic of varicella and other directly transmitted viral infections and has been widely documented in school-based outbreaks (14).
Environmental assessment findings indicated shared play equipment and communal napping spaces among kindergarten pupils likely facilitated transmission, consistent with evidence linking shared fomites and close-contact activities to varicella and other viral diseases spread (15).
Laboratory findings confirmed of varicella-zoster virus in two cases. These findings highlight the complexity of rash outbreaks, where timing of testing is crucial, and underscore the limitations of relying solely on laboratory confirmation in resource-limited settings.
Study limitation: We were not able to identify how the primary case acquired the infection and we were not able to test all the cases due to resource constraints.
Conclusion: The febrile rash illness outbreak among primary school children in the Greater Kampala Metropolitan Area was most likely due to varicella Zoster (Chicken pox) with atypical presentation and was fueled by shared playing and napping spaces and lack of VZV vaccination.
Public health actions: To stop the propagation of the outbreak, we sensitized school administrators and teachers on the modes of transmission, early recognition of symptoms, and the importance of prompt reporting and isolation of suspected cases. Teachers were actively engaged in daily classroom-based screening and monitoring of pupils for fever, rash, and oral lesions. We also conducted health education sessions for pupils using age-appropriate messages focusing on hand hygiene, avoidance of close contact when ill, and proper respiratory etiquette.
Recommendations: To prevent spread to other schools, we recommended that, the Ministry of Health issue an advisory to all schools in the Greater Kampala Metropolitan Area to strengthen surveillance and early reporting of febrile rash illnesses. We also recommend incorporation of VZV vaccine in routine immunization schedule for children. We further recommended to Kampala City Council Authority to develop and disseminate clear public information materials for parents and caregivers on symptoms, transmission, and prevention of the illness through schools, health facilities, and digital platforms.
Conflict of interest: The authors declare that they have no conflict of interest.
Authors’ contributions: MM, WJ, NA, NE, RT and NA designed the study and contributed to data collection and analysis. MM led the writing of the bulletin. BL, RM, and BK participated in the writing of the bulletin and review to ensure scientific integrity. All authors contributed to the final draft of the bulletin.
Acknowledgments: The authors would like to thank the administration of school X, Kampala Capital City Authority department of Public Health, Kiswa Health Centre IV and Ministry of Health for their support in active case search and line listing of cases during this investigation.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source; however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Freer G, Pistello M. Varicella-zoster virus infection: natural history, clinical manifestations, immunity and current and future vaccination strategies. New Microbiol. 2018 Apr;41(2):95–105. PubMed PMID: 29498740.
- Dooling K, Marin M, Gershon AA. Clinical Manifestations of Varicella: Disease Is Largely Forgotten, but It’s Not Gone. The Journal of Infectious Diseases. 2022 Oct 21;226(Supplement_4):S380–4. doi:10.1093/infdis/jiac390
- Nelson WE. Nelson textbook of pediatrics. 20th edition. Kliegman R, Stanton B, St Geme JW, Schor NF, Behrman RE, editors. Philadelphia, Pennsylvania: Elsevier; 2016.
- Abendroth A, Arvin AM, Moffat JF, editors. Varicella-zoster Virus [Internet]. Vol. 342. Berlin, Heidelberg: Springer Berlin Heidelberg; 2010 [cited 2026 May 20]. (Current Topics in Microbiology and Immunology). Available from: https://link.springer.com/10.1007/978-3-642-12728-1 doi:10.1007/978-3-642-12728-1
- Barry R, Prentice M, Costello D, O’Mahony O, DeGascun C, Felsenstein S. Varicella Zoster Reactivation Causing Aseptic Meningitis in Healthy Adolescents: A Case Series And Review Of The Literature. Pediatric Infectious Disease Journal. 2020 Sep;39(9):e278–82. doi:10.1097/INF.0000000000002759
- Lopez AS, LaClair B, Buttery V, Zhang Y, Rosen J, Taggert E, et al. Varicella Outbreak Surveillance in Schools in Sentinel Jurisdictions, 2012–2015. Journal of the Pediatric Infectious Diseases Society. 2019 May 11;8(2):122–7. doi:10.1093/jpids/piy010
- Yang Z, Zhang Q, Cowling BJ, Lau EHY. Estimating the incubation period of hand, foot and mouth disease for children in different age groups. Sci Rep. 2017 Nov 28;7(1):16464. doi:10.1038/s41598-017-16705-7
- Chan DYW, Edmunds WJ, Chan HL, Chan V, Lam YCK, Thomas SL, et al. The changing epidemiology of varicella and herpes zoster in Hong Kong before universal varicella vaccination in 2014. Epidemiol Infect. 2018 Apr;146(6):723–34. doi:10.1017/S0950268818000444
- Civen R, Lopez AS, Zhang J, Garcia‐Herrera J, Schmid DS, Chaves SS, et al. Varicella Outbreak Epidemiology in an Active Surveillance Site, 1995–2005. J INFECT DIS. 2008 Mar;197(s2):S114–9. doi:10.1086/522144
- Meng Q, Wang B, Zhang X, Li Z, Wang W, Yao K. Case Report: Various Clinical Manifestations Caused by Varicella-Zoster Virus in a Family. Front Pediatr. 2022 Jun 6;10:876250. doi:10.3389/fped.2022.876250
- Dagrosa AT, Collins LK, Chapman MS. Atypical herpes zoster presentation in a healthy vaccinated pediatric patient. Cutis. 2017 Nov;100(5):303–4. PubMed PMID: 29232420.
- Onyango C, Hines JZ, Ochieng M, Amon D, Lidechi S, Anguko E, et al. High Prevalence of Varicella Zoster Virus Infection among Persons with Suspect Mpox Cases during an Mpox Outbreak in Kenya, 2024. The American Journal of Tropical Medicine and Hygiene. 2025 Dec 3;113(6):1411–4. doi:10.4269/ajtmh.25-0308
- Ryu S, Han C, Ali ST, Achangwa C, Yang B, Pei S. Association of public health and social measures on the hand-foot-mouth epidemic in South Korea. Journal of Infection and Public Health. 2023 Jun;16(6):859–64. doi:10.1016/j.jiph.2023.03.029
- Zhao J, Hu X. The complex transmission seasonality of hand, foot, and mouth disease and its driving factors. BMC Infect Dis. 2019 Dec;19(1):521. doi:10.1186/s12879-019-4153-6
- Azuma K, Yanagi U, Kagi N, Kim H, Ogata M, Hayashi M. Environmental factors involved in SARS-CoV-2 transmission: effect and role of indoor environmental quality in the strategy for COVID-19 infection control. Environ Health Prev Med. 2020 Dec;25(1):66. doi:10.1186/s12199-020-00904-2