
Investigation of a cross-district measles outbreak in Nwoya District, Uganda, December, 2025–February, 2026
Authors: Pauline Achom1*, Richard Migisha1, Winfred Nakaweesi1, Justine Wobusobozi, Benon Kwesiga1, Emmanuel Mfitundinda1, Anne Loy Alupo1, James Okello2, Deogratious Munube3, Yasiini Nuwamanya4, Deogratious Migadde5. Institutional Affiliation:¹Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Nwoya District Local Government, Nwoya, Uganda, 3Makerere University, College of Health Sciences, Kampala, Uganda, 4Uganda National Expanded Program on Immunization, Ministry of Health, Kampala, Uganda, 5Ministry of Health, Kampala, Uganda Correspondence*: Email: achompauline@uniph.go.ug; Tel: +256785253791
Summary
Background: Measles is a major cause of vaccine-preventable morbidity and mortality in children. On February 5, 2026, the Uganda Ministry of Health was notified of a measles outbreak among residents in Nwoya District. We investigated to estimate the magnitude of the outbreak and risk factors for transmission to inform control and prevention measures.
Methods: We defined a suspected case as fever and maculopapular rash with ≥1 of cough, coryza, or conjunctivitis in a resident of Nwoya District from December 16, 2025–February 18, 2026. A confirmed case was a suspected case that had a positive measles IgM test. Cases were identified through health facility records review and active community search. We calculated attack rates (AR) by sub-county, sex, and age group. We conducted an unmatched case-control study (1:3) to identify risk factors for transmission. We also estimated vaccine effectiveness (VE) and vaccination coverage (VC).
Results: We identified 100 cases (95 suspected, 5 confirmed) with no deaths. The index case was a 17-year-old male returning from Amuru District, who was experiencing a concurrent measles outbreak. Overall AR was 145/100,000 population. The most affected areas were Koch-Goma Town Council (381/100,000 and Lii Sub-county (154/100,000), with the highest AR among children aged 9–59 months (165/100,000). Receiving at least one MR dose (aOR=0.25: 95%CI=0.11–0.55) and staying at home (aOR=0.05:95%CI: 0.0070–0.34) were protective. Travel to Nwoya District (aOR=5.2:95%CI=1.5–19), receiving visitors from neighbouring districts (aOR=5.1:95%CI=1.7–15), and crowding around swamp water (aOR=18:95%CI=2.7–118) increased risk. Vaccine Coverage was 64% (96/150), and VE was 75%.
Conclusion: The outbreak was likely from a spillover from neighbouring districts propagated by low VC, crowding around swamps, and the reception of visitors. We recommend increasing the number of outreach vaccinations and household screening of visitors through community engagement. Avoiding crowding and strengthening cross-district disease surveillance and coordination mechanisms to improve detection and response timeliness.
Background
Measles is a highly transmissible, vaccine-preventable viral disease caused by the measles virus (1). It is transmitted primarily through respiratory droplets or direct contact with an infected person. Without vaccination, >90% of individuals can get infected before their 10th birthday(1). The incubation period of measles is 7–21 days (2). Its typical symptoms are high-grade fever, cough, coryza (runny nose), and conjunctivitis with maculopapular rash (1). Complications of measles include diarrhea, otitis media, corneal ulceration, pneumonia, and death(3). Measles remains a major cause of morbidity and mortality, particularly among children under five years of age. Vaccination, being one of the most effective strategies, averted about 60 million deaths in 2000–2023 (4).
In Uganda, the first dose of the Measles Rubella Vaccine has remained suboptimally low at 85% despite efforts to reach every district and child by the Uganda National Expanded Programme on Immunization (5). Hence, Uganda has continued to experience outbreaks due to immunity gaps. On February 5, 2026, a measles outbreak was reported in Nwoya District, Uganda, following confirmation by the Uganda Virus Research Institute (UVRI) in Lii Sub-county, Nwoya District. We estimated the magnitude of the outbreak and identified risk factors for transmission to inform control and prevention measures.
Methods
Nwoya District, is located in Acholi Region, Uganda. The district has an estimated population of 220,593, with 11 sub-counties, 44 parishes, and 124 villages. The outbreak primarily affected the Koch-Goma Town Council and Lii Sub-county with a total population of 108,032.
We defined a suspected case as the onset of fever and maculopapular rash plus ≥1 of the following symptoms: cough, coryza (runny nose), or conjunctivitis (red eyes), in a resident of Nwoya District from December 16, 2025–February 18, 2026; and a confirmed measles case was defined as a suspected case with laboratory confirmation of measles-specific IgM antibodies. We reviewed records and line-listed cases from Koch-Lii HC III, Koch-Goma HC III, Todora HC III, Anaka General Hospital, and Goro Medical Center in Nwoya District. Data on their demographics, clinical characteristics, vaccination status, exposure history, vitamin A supplementation, and outcome were collected. We conducted active case search through household visits and community register reviews. Immunization records were also reviewed. Blood samples from the first five suspected case-patients were tested for measles IgM antibodies.
We generated attack rates (AR) by age, sex, and sub-county. We drew choropleth maps using QGIS to illustrate attack rates by Sub-county. We described cases by time of symptom onset using an epidemiological curve. Hypothesis-generating interviews were conducted among 20 case-patients to identify potential exposures associated with infection, including vaccination status, recent arrival into the area, attendance at gatherings, contact with symptomatic persons at health facilities, and use of communal water points. We conducted an unmatched case-control study with 50 cases and 150 controls (1:3 ratio) to identify the risk factors for transmission. We defined a control as a resident of Koch Goma or Koch Lii Sub-counties, with no history of fever nor rash from December, 01 2025 to February 18, 2026. Vaccine coverage was estimated using vaccination status among controls, while VE was calculated as VE = (1 − aOR) × 100%.
The outbreak investigation was conducted as part of the public health emergency response and was classified as non-research/public health practice by the Uganda Ministry of Health and the US CDC. It was approved and reviewed by the US CDC in accordance with applicable federal laws, CDC policy, and the Declaration of Helsinki. Informed consent was obtained from participants aged ≥18 years, whereas parental/guardian consent and participant assent were obtained for those under 18 years.
Results
Descriptive epidemiology
We identified 100 case-patients (95 suspected, 5 confirmed, and no deaths). The overall attack rate was 45/100,000 population. All the cases were Ugandan nationals. The majority of cases were females (n=56, 54%) with an AR of 50/100,000 population (Table 1). Most (54%) case-patients were aged 9-59 months and were the most affected (AR 165/100,000 population). All cases presented with a fever and a rash followed by cough (92%) and coryza (90%).
Table 1: Attack rate by sex and age per 100,000 population December, 2025–February, 2026 (n=100)
| Category | No. of cases | Population at risk | Attack rates per 100,000 population |
| Sex | |||
| Male | 44 | 107,748 | 41 |
| Female | 56 | 112,845 | 50 |
| Overall | 100 | 220,593 | 45 |
| Age | |||
| <6months | 5 | 6,838 | 73 |
| 6-8months | 8 | 5,735 | 140 |
| 9-59months | 54 | 32,648 | 165 |
| 5-15years | 25 | 47,207 | 53 |
| ≥15 years | 8 | 127,944 | 6 |
| Overall | 100 | 220,593 | 45 |
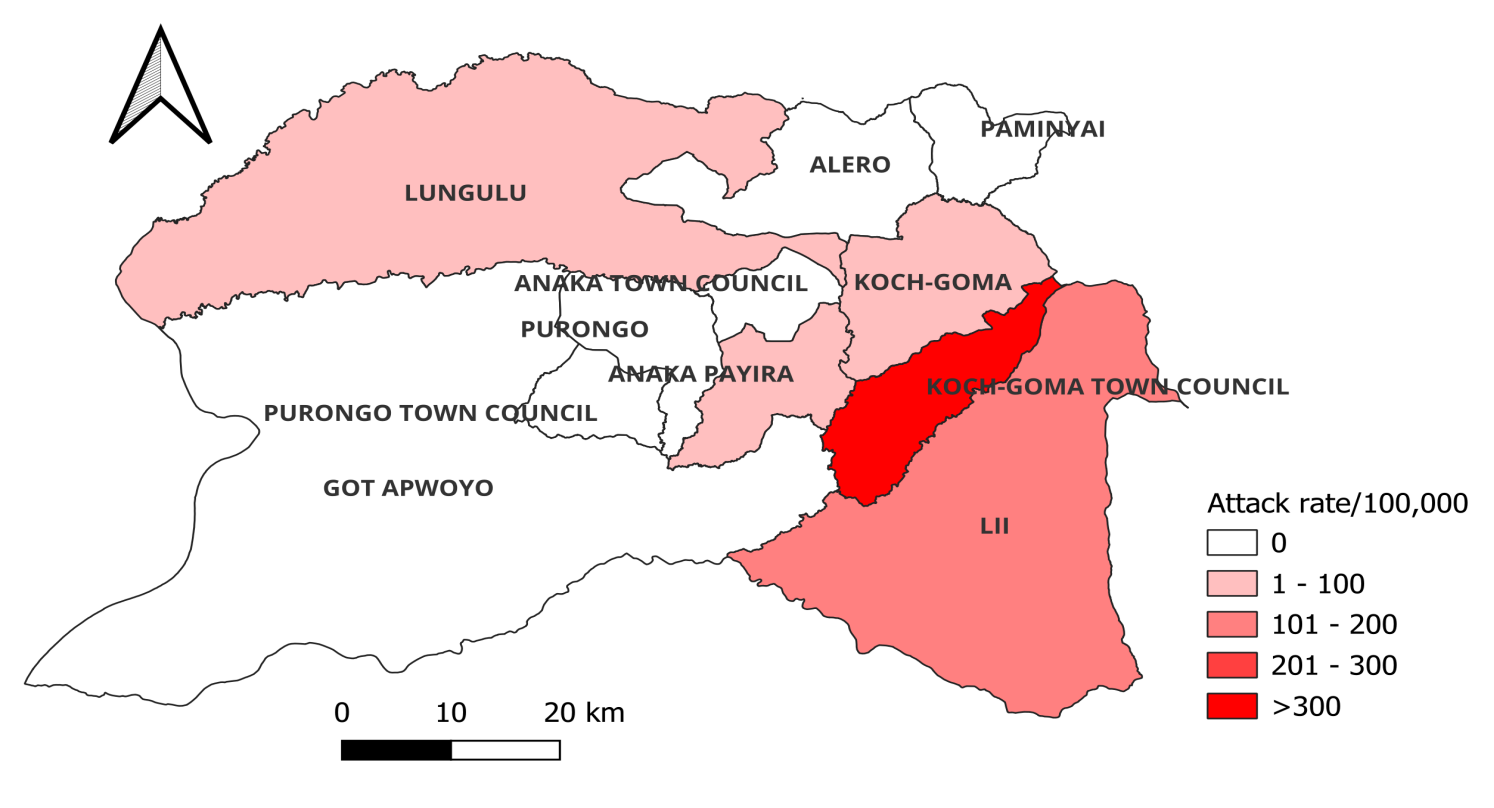
Among the Sub-counties that reported cases, Koch-Goma Town Council was the most affected with an AR of 381cases/100,000 population, followed by Lii with 154/100,000 (Figure 1).
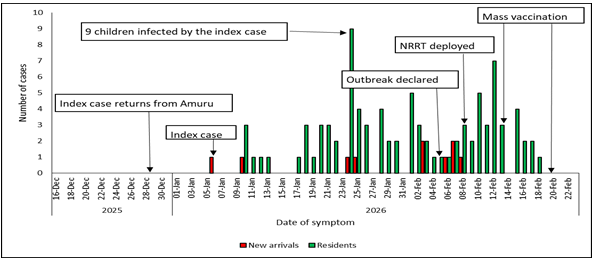
The epidemic curve indicated a propagated outbreak with peaks on January 24 and February 12, 2026, suggesting person-to-person transmission. The outbreak began in early January and persisted for over a month, likely fueled by movement from neighboring districts experiencing measles outbreaks. The index case, a 17-year-old male who returned from Amuru District on December 28, 2025, went to church, playgrounds, and water collection points while symptomatic and subsequently infected household and community contacts. He had received only one measles vaccine dose. The outbreak was declared on January 5, 2026, the National Rapid Response Team was deployed three days later, and a mass vaccination campaign was conducted on January 19, 2026 (Figure 2).
Hypothesis generation findings: Among the 20 cases interviewed, 14 (70%) were unvaccinated, 12 (60%) had attended social gatherings, 10 (50%) had visited a health facility, 10 (50%) had used communal water points, and 6 (30%) had recently arrived in the community. We hypothesized that unvaccinated children aged 9–59 months and those exposed to social gatherings or symptomatic visitors were at increased risk of measles infection.
Case Control findings
Unvaccinated children were nine times more likely to develop measles than vaccinated children (aOR=9, 95%CI:1–80). Children who had recently received visitors were five times more likely to develop measles (aOR=5.07, 95%CI:1.7–15). Recent travel from districts with active outbreaks also increased risk fivefold (aOR=5, 95%CI:1.5–19). Collecting water from swamps increased odds 18-fold (aOR=18, 95%CI:2.7–118). In contrast, children who played at home were less likely to develop measles (aOR=0.05, 95%CI:0.007–0.34) (Table 2).
Table 2: Risk factors for measles outbreak in Koch-Goma Town council and Lii Sub-County District, Uganda, December 2025–February 2026 (n=200)
| Risk factor | n(%) Cases(n=50) | n(%) Controls(n=150) | OR (95% CI) | p-value | aOR (95% CI) | p-value |
| Vaccination status | ||||||
| ≥ one MR dose | 17(34) | 108(72) | 0.2 (0.10–0.4) | <0.005 | 0.25(0.11–0.55) | 0.001 |
| No vaccination | 33(66) | 42(28) | Ref | |||
| Vaccination doses | ||||||
| No vaccination | 33(66) | 42(28) | 9.4(1.2–76) | 0.035 | 9(1.0–80) | 0.05 |
| 1st dose only | 16(32) | 96(64) | 2(0.24–17) | 0.52 | 2.4(0.27–22) | 0.43 |
| Two doses | 1(2) | 12(8) | Ref | |||
| Source of water | ||||||
| Swamp | 8(16) | 2(1) | 20(3.7–104) | <0.001 | 18(2.7–118) | 0.003 |
| Borehole | 29(58) | 84(56) | 1.7(0.82–3.5) | 0.16 | 1.5(0.6–3.7) | 0.38 |
| Well | 13(26) | 64(43) | Ref | |||
| Play area 3 weeks before | ||||||
| Home | 11(22) | 52(35) | 0.05(0.01–0.28) | 0.001 | 0.05(0.007–0.34) | 0.002 |
| Neighborhood | 31(62) | 96(64) | 0.081(0.016–0.4) | 0.002 | 0.17(0.028–1.1) | 0.06 |
| Away from home | 8(16) | 2(1) | Ref | |||
| Travelled to Nwoya | ||||||
| Yes | 10(20) | 8(5) | 4.4(1.6–12) | 0.003 | 5.2(1.5–19) | 0.011 |
| No | 40(80) | 142(95) | Ref | |||
| Received a visitor in the last 3 weeks | ||||||
| Yes | 15(30) | 22(15) | 2.5(1.2–5.3) | 0.02 | 5.1(1.7–15) | 0.003 |
| No | 35(70) | 128(85) | Ref |
1 Water collection point, playground
Measles vaccine coverage and effectiveness: The vaccine coverage was 64% while the estimated effectiveness was 75% (aOR:0.25 (95% CI: 0.11–0.55, p=0.001)).
Discussion
Lack of measles vaccination, use of swamp water, recent travel to Nwoya, and receiving visitors at home were associated with measles transmission. However, vaccination and playing at home were protective against measles infection. These findings are consistent with the established epidemiology of measles and highlight both immunity gaps and opportunities for transmission within the community. Children who had not received any measles vaccination were nine times more likely to develop measles compared to those who had received two doses. This strong association reinforces the well-documented protective effect of measles-containing vaccines and aligns with evidence from outbreaks in similar settings where vaccination protects up to about 95% of children (6-8). Despite the availability of routine immunization services through the Ministry of Health and global guidance from the World Health Organization, immunity gaps persist, particularly among unvaccinated children. This trend suggests incomplete protection with a single dose, supporting the two-dose strategy recommended under the Uganda Expanded Programme on Immunization. The findings underscore the importance of achieving and sustaining high coverage with two doses to prevent outbreaks and interrupt transmission.
Use of swamp water was independently associated with a markedly increased risk of measles infection. While measles is primarily transmitted via respiratory droplets rather than water, this association may reflect underlying socioeconomic and environmental vulnerabilities. Households relying on swamp water may represent more remote or under served communities with reduced access to health services, including immunization. Such settings may also facilitate clustering of susceptible individuals, increasing the likelihood of outbreak propagation. These findings are similar to those from Mayuge District in Uganda (9). This finding highlights the importance of addressing broader social determinants of health in measles prevention strategies.
Children who played at home were significantly less likely to develop measles compared to those who played away from home; this is similar to findings from Ssemuto (2). This shows that social interactions among susceptible individuals increase the chances of measles transmission. Likewise, those who had received visitors at home had five times higher odds of infection.
Receiving visitors may have introduced the virus into households, particularly in communities with low immunity levels. These results are consistent with the known high basic reproduction number (R₀) of measles, which is about 12-18 susceptible individuals infected during an outbreak, where even brief contact with an infectious person can result in transmission among susceptible individuals. These findings are similar to findings in Australia, where the role of travel was significant in measles outbreaks (10).
Study limitations: The study may have been limited by recall bias, as some exposures like contact with a case and attendance at crowded social gatherings, were self-reported. This may have resulted in exposure misclassification and inaccurate reporting of risk factors. Conclusion: The outbreak was driven by low vaccination coverage, social mixing, and population movement. We recommend strengthening two-dose measles vaccination, expanding targeted outreach services, and improving surveillance as critical to preventing future outbreaks. Also, community engagement to identify symptomatic new arrivals, and training health workers and Village Health Teams on case detection and timely reporting.
Conflict of interest: The authors declare no conflict of interest.
Authors’ contribution: PA drafted the initial version of the manuscript. RM, WN, JW, BK, EM, ALA, JO, DM, SPK, YN, and DM revised the article for substantial intellectual content. WN, JW, and EM participated in the outbreak investigation. RM also supervised the field data collection and reviewed the draft article for substantial intellectual content. All authors read and approved the final article.
Acknowledgements: We appreciate the District Health Team of Nwoya District Local for providing VHTs and conducting mass vaccination and risk communication. We also acknowledge the Ministry of Health, through the Uganda National Expanded Program for Immunization (UNEPI) and the Public Health Fellowship Program, for their technical support.
Copyrighting and licensing: All material in the Uganda Public Health Bulletin is in the public domain and may be used and printed without permission. However, citation as to source is appreciated. Any article can be reprinted or republished. If cited as a reprint, it should be referenced in the original form.
References
- Rewar S. Measles virus: a perpetual challenge. Indian Journal of Research in Pharmacy and Biotechnology. 2015;3(3):196.
- Nsubuga EJ, Morukileng J, Namayanja J, Kadobera D, Nsubuga F, Kyamwine IB, et al. Measles outbreak in Semuto Subcounty, Nakaseke District, Uganda, June–August 2021. IJID regions. 2022;5:44-50.
- Organization WH. Measles vaccines: WHO position paper, April 2017—Recommendations. Vaccine. 2017.
- Minta AA. Progress toward measles elimination—worldwide, 2000–2023. MMWR Morbidity and Mortality Weekly Report. 2024;73.
- Mfitundinda E, Namusisi A, Wenani D, Ayeerwot R, Korobe E, Ssekandi D, et al. Measles outbreak imported through the porous border in Moroto District, Uganda, March–July, 2024.
- Bester JC. Measles and measles vaccination: a review. JAMA Pediatrics. 2016;170(12):1209-15.
- Zipprich J, Winter K, Hacker J, Xia D, Watt J, Harriman K, et al. Measles outbreak—California, december 2014–february 2015. MMWR Morb Mortal Wkly Rep. 2015;64(6):153-4.
- Control CfD, Prevention. Vaccines and immunizations. Preparing for the Potential Management of Anaphylaxis Available online: https://www cdc gov/vaccines/covid-19/clinical-considerations/managing-anaphylaxis html (accessed on 16 October 2022). 2014.
- Majwala RK, Nakiire L, Kadobera D, Ario AR, Kusiima J, Atuhairwe JA, et al. Measles outbreak propagated by children congregating at water collection points in Mayuge District, eastern Uganda, July–October, 2016. BMC infectious diseases. 2018;18(1):412.
- Macintyre CR, Karki S, Sheikh M, Zwar N, Heywood A. The role of travel in measles outbreaks in Australia–An enhanced surveillance study. Vaccine. 2016;34(37):4386-91.