
Factors associated with mpox severity in Mbarara City, October 2024–May 2025
Authors: Justine Wobusobozi1*, Sharon Namasambi1, Aminah Namwabira1 ,Pauline Achom1, Michael Mutegeki1, Irene Kyamiwine1, Benon Kwesiga1, Richard Migisha1 Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda. Correspondence*: Tel: +256 772 041876, Email: justinewobusobozi@uniph.go.ug
Summary
Background: Mpox, a zoonotic viral disease caused by monkeypox virus was confirmed in Uganda on 24th July,2024. In October 2024, Mbarara experienced a sustained mpox transmission with Nyamityobora Ward disproportionately burdened by severe cases. We identified factors associated with mpox severity in Nyamityobora Ward, Mbarara City, October 2024 to May 2025 to improve patient outcomes and guide control measures. Methods: We conducted a cross-sectional study among suspected cases in Nyamityobora Ward during April and May 2025. Suspected cases were defined as sudden onset of skin rash or genital lesions and ≥2 of the following symptoms: fever of 38.5°C, headache, general body weakness, muscle or body aches, back pain, genital discharge, swollen lymph nodes, or mucosal lesions in a person living in Nyamityobora Ward,Mbarara City from October 2024 to May 2025. We interviewed cases through house-to-house visits to collect data on health-seeking behavior, exposure history and severity. Severity was scored using an adapted Mpox Severity Scoring System (MPSS) tool; we dichotomized severity into severe (>20 points) and non-severe (≤20 points) for analysis. We identified factors associated with severity using modified Poisson regression. Results: We identified 106 suspected mpox cases with a median age of 29 years (range: 0–75 years). Of these, 23 (22%) had HIV co-infection, 28 (26%) reported delayed care-seeking (>5 days from symptom onset), and 20 (19%) were sex workers. Of the 106 suspected cases, 62 (59%) presented with severe disease, 30 (28%) with moderate disease, and 14 (13%) with mild disease. HIV coinfection (aPR=1.8, 95% CI: 1.2-2.7) and delayed care-seeking (>5 days; aPR=1.5, 95% CI: 1.1-2.1) were associated with severe illness.Conclusion: Severe mpox was associated with HIV co-infection and delayed care-seeking. We recommend targeted screening for mpox among HIV patients and awareness campaigns promoting early care-seeking and the availability of mobile testing units to facilitate early diagnosis.
Background
Uganda confirmed its first mpox cases in Kasese District on July 24, 2024, with transmission reaching Mbarara City by November 4, 2024. By April 16, 2025, Mbarara City had reported 420 confirmed cases, with an attack rate of 142 per 100,000 population, ranking it third among affected areas outside the Kampala Metropolitan Area according to the situation report from Ministry of Health (MoH) dated April 14,2025. Unlike other districts where case numbers declined, Mbarara’s epidemic curve continued to rise, indicating sustained community transmission. Mpox is a multisystemic disease affecting several organs of the body and in some cases leading to death. The clinical presentation of the disease differs by the route of exposure, immune status of the host, the strain of the virus and the dose of the virus. Additionally, the disease has variable clinical severity. People living with HIV(PLHIV) especially those with advanced disease, children <5 years of age, and pregnant women are more likely to develop severe disease and have higher case fatality rates. Clade Ib is more likely to cause severe disease compared to clade Ia and II (1). Severe cases may contribute to prolonged viral shedding, potentially amplifying transmission to close contacts (2). These challenges highlight the urgent need for early identification and targeted interventions to mitigate severe outcomes and reduce the public health burden. We determined the prevalence of mpox severity and identified factors associated with severe mpox infection in Nyamityobora Ward, Mbarara City, October 2024–May 2025.
Methods
Mbarara City is a growing urban and transit hub linking Uganda to Rwanda and the Democratic Republic of Congo, increasing its risk of disease spread. Nyamityobora Ward, in the Southern division, is an urban area with high population mobility due to traders, sex workers, and casual laborers.
We defined an mpox suspected case as acute onset of skin rash or genital lesions with at least 2 of the following symptoms: Fever, Headache, general body weakness, Myalgia, Back pain, Genital discharge, Lymphadenopathy and mucosal lesions in a resident of Nyamityobora Ward from October 2024 to May 2025.
We conducted a cross-sectional study applying active case search by movement from house to house in Nyamityobora Ward. Using a case investigation form, we obtained case sociodemographic characteristics, underlying conditions, and health-seeking behavior. To ascertain the degree of severity, we adapted the Mpox Severity Scoring System (MPSS) to construct a tool that would score severity for the sick, recovered and dead mpox cases. The adapted scoring tool scored 1 point per symptom, 0-6 points for pain, 1 point per body part with rash, 4 points for pus discharge, 0-8 points for outcome ranging from recovered, still sick to dead and 1-4 for healthcare utilization that is seeking care, hospitalization and an additional facility visit. The maximum score was 55 points. We scored the cases to ategorize them into 3 categories which were: Mild with a score of 0-10 points, Moderate with a score of 11-20 points and Severe with a score greater than 20 points. We then dichotomized the categories into severe for those having points greater than 20 and non-severe for those with points less than 20 points. We used Modified Poisson regression analysis to identify the factors associated with severe mpox. The Ministry of Health of Uganda gave the directive and gave approval to conduct this study. The Office of the Associate Director for Science at the US Centers for Disease Control and Prevention (CDC) Uganda determined that this research did not involve human subject research and that its primary intent was public health practice or disease control. Verbal informed consent was obtained from participants or, , if the interviewee was a minor, guardians before the start of each interview.
Results
We identified 106 suspected cases, of which one patient died (0.9%, 1/106). All cases (100%, 106/106) reported skin or genital rash. Cases were distributed across all ten cells, with Muti (20%, 21/106), Market and Lower (14%, 15/106) reporting the highest proportions. Of the 56 cases who reported underlying conditions, 41% (23/56) had HIV. The other underlying conditions included hypertension, diabetes, peptic ulcer disease, asthma, and pregnancy. Of the 106 cases, 54%
(57/106) were female, with a median age of 29 years (range: 8 months–75 years).
Table : Demographic characteristics of mpox cases in Nyamityobora ward, October 2024-May 2025 (n=106)
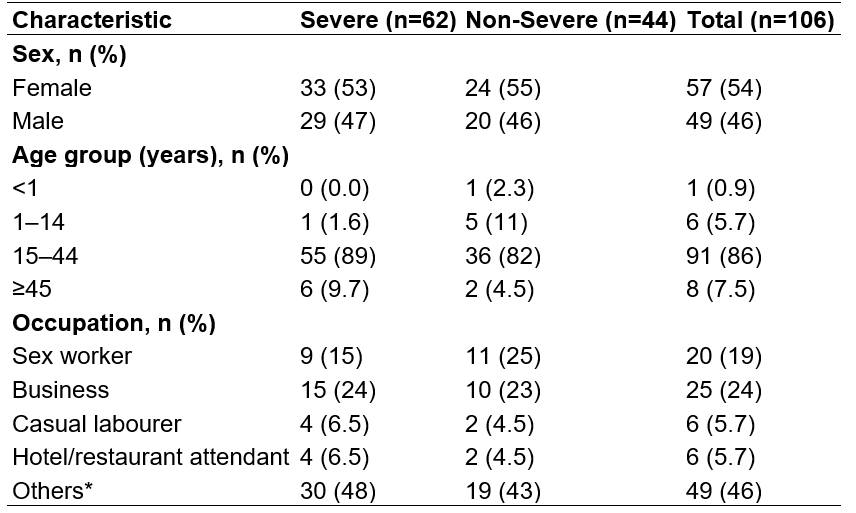
*Others in occupation include Bar attendant, Student, Builder, Driver. Farmer, Boda-Boda rider, others, * p-values are from chisquare tests comparing severe vs. non-severe cases. Prevalence of mpox severity in Nyamityobora Ward, Mbarara City, October 2024–May 2025 Of 106 cases, 62(59%) were severely ill, 30 (28%)
moderately ill, and 14 (13%) with mild illness. Among those severely ill, 33(53%) were female, most 55(89%) were aged 15-4 years followed by ≥45 of age who contributed 6(10%), and 1-14 years of age who contributed 1(2%).
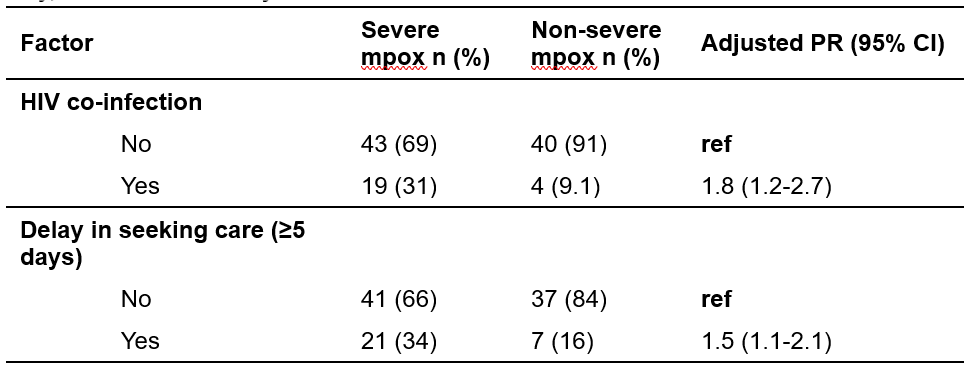
Factors associated with mpox severity in Nyamityobora Ward, Mbarara City, October 2024–May 2025
Individuals with HIV co-infection had an 80% higher prevalence of severe mpox compared to those without HIV. Also to note, delaying care by 5 or more days was associated with a 50% higher prevalence of severe mpox compared to those who sought care earlier.
Table 2: Factors associated with mpox severity, Nyamityobora Ward, Mbarara City, October 2024–May 2025
Discussion
Our findings contribute to further characterization of the current mpox pandemic, focusing on severity of the infection. We found a more than half prevalence of severe mpox infection and a low proportion of deaths among cases. The high prevalence of mpox severity was associated with HIV co-infection and delay in seeking care for 5 or more days. Other studies have found similar findings, with PLHIV more likely to have severe presentations of mpox compared to those
without HIV. Case-patients with HIV were also more likely to be hospitalized compared to those without HIV (3,4). Additionally, delayed care seeking has been linked to worsened outcomes in mpox, as early intervention can reduce viral load and complications, consistent with findings from similar outbreaks where timely treatment improved recovery rates (2).
Study limitations and strengths: We adapted the MPSSS tool since we needed to determine severity for the sick, recovered and dead cases and so could not primarily use the MPSSS tool. There could also have been an overestimation of the scores due to subjective or reported assessment of pain as well as recall bias for those that had recovered way back. Despite the limitations, the study demonstrated consistency in the clinical presentation and outcome of mpox cases with
their respective severity scores.
Conclusion
We found a more than half prevalence of severe mpox infection and mpox severity was associated with HIV co-infection and delay in seeking care for 5 or more days. when ill. We recommend targeted screening for mpox disease among HIV patients and sensitization of the community about the advantages of timely seeking of health care.
Conflict of interest: The authors declared no conflict of interest.
Authors’ contribution: All authors contributed to the write-up and review of the bulletin article. JW drafted the initial version of the article. JW, SN, AN, PA, and MM participated in the data collection and case investigations. RM, BK, and IK supervised the field data collection and reviewed the draft bulletin article for substantial intellectual content. All authors read and approved the final bulletin article.
Acknowledgements: We acknowledge the support of village health teams in Nyamityobora Ward who moved with us as we conducted data collection. We also acknowledge the logistical, financial, and technical support of the Ministry of Health, Uganda, in the entire outbreak response.
Copyright and licensing: All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Ogoina D, Damon I, Nakoune E. Clinical review of human mpox. Clinical Microbiology and Infection. 2023;29(12):1493-501.
- Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison LB, et al. Monkeypox virus infection in humans across 16 countries—April–June 2022. New England Journal of Medicine. 2022;387(8):679-91.
- Taha AM, Elrosasy A, Mahmoud AM, Saed SAA, Moawad WAET, Hamouda E, et al. The effect of HIV and mpox co‐infection on clinical outcomes: Systematic review and meta‐analysis. HIV medicine. 2024;25(8):897-909.
- Silva MS, Coutinho C, Torres TS, Peixoto EM, Bastos MO, Mesquita MB, et al. Mpox severity and associated hospitalizations among people with HIV and related immunosuppression in Brazil. AIDS. 2024;38(1):105-13.
Comments are closed.