
Strengthening Disease Surveillance in Rhino Camp Refugee Settlement-Arua District, Sept 2016
Authors: Emily Atuheire1, Leocadia Kwagonza1, Daniel Kadobera1 Alex R. Ario1; Affiliation: 1Uganda Public Health Fellowship Program
Summary
On 29 August 2016, we visited Rhino Camp Refugee Settlement in Arua District to ascertain capacity for timely detection and response to disease outbreaks and strengthen the surveillance system to ensure early warning and response to epidemic threats. This followed a looming threat of a cholera epidemic due to the sudden influx of refugees from South Sudan who had increased the settlement population by 50%. We interviewed staff from 4 Health Centres serving the Settlement and reviewed facility records. All Health Centres were adequately staffed. Two parallel Surveillance Systems were in place i.e. the National Health Mangement Information (HMIS) and Health Information (HIS) for United Nations High Commission for Refugees (UNCHR). The latter system was more active than the former despite deficiencies in case definitions and action thresholds. This coupled with lack of knowledge on and use of Integrated Disease Surveillance and Response (IDSR) guidelines, led to skewed data capture, irregular reporting and weak alert system. The District Health Team immediately intervened with training and mentorship of facility staff on case detection and reporting. We recommended training of Facility staff on IDSR implementation and harmonization of guidance on disease surveillance in Rhino Camp Refugee Settlement.
Introduction
By 28th August 2016 in a period of just one month, over 11,800 refugees from had reached Rhino Camp Refugee Settlement in Arua District following fresh political clashes in neighboring South Sudan.
The new arrivals accounted for over 50% increase in the existing refugee population. At least 500 people were received on a daily basis at Ocea Refugee Reception Centre in Rhino Camp, majority of them being women and children.
With this influx, there was a high risk of epidemic prone diseases such as cholera etc. due to challenges of inadequate and unsafe water, poor sanitation facilities, overcrowding and lack of shelter. At the time of this influx, cholera outbreaks were confirmed in Pagirinya Refugee Camp in neighboring Adjumani District as well as Nebbi District.
Thus there was urgent need for early detection and prompt response to disease outbreaks in Rhino Camp Refugee Settlement. At the invitation of the District Health Officer, we visited Rhino Camp Refugee Settlement on 29 Aug 2016, to ascertain capacity for timely detection and response to disease outbreaks and strengthen the surveillance system to ensure early warning and response to epidemic threats.
Methods
We visited 4 health centers and one refugee reception centre within 3 sub-counties housing the refugee settlement At the Health Centres we interviewed staff including HMIS/surveillance focal persons, nurses, clinicians and laboratory personnel and reviewed records to obtain information on the existing surveillance system.
We collected data on the core and support functions of the existing disease surveillance system including availability of human resource, staff training on IDSR, capacity for detection/identification of epidemic prone diseases, case definitions used, data capture and reporting, analysis and interpretation of surveillance data, capacity to investigate and confirm outbreaks, epidemic preparedness and feedback mechanisms.
Findings
Health Service Availability
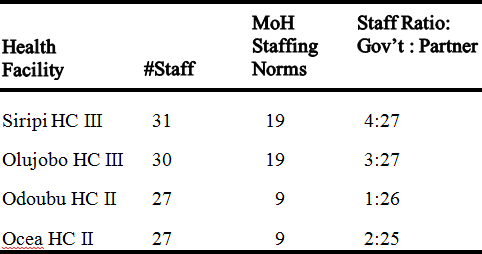
All Health Centres are well staffed above the MoH recommended standard. However, majority of the staff are not supported by Government of Uganda.
Surveillance systems in place
Parallel surveillance systems were in place: the National Health Management Information System (HMIS) and Health Information System (HIS) for the UNHCR.
Parallel surveillance systems were in place: the National Health Management Information System (HMIS) and Health Information System (HIS) for the UNHCR. These parallel systems provide different data capture, reporting tools and structures with varying timelines and requirements. There were different case definitions and thresholds for alert and action to guide detection and response to outbreaks. The HIS was more active, although deficient in case definitions and action thresholds, leading to skewed data capture and irregular reporting.
| Strengths | Gaps |
| – HMIS tools available
– Weekly and monthly reports were compiled & submitted – Some level of data analysis occurred – Feedback mechanisms exist, i.e. CMEs, performance review meetings and sup- port supervision |
– Irregular and inconsistent reporting
– Staff lacked knowledge on standard case definitions as per Integrated Disease Surveillance (IDSR) guidelines – Weak alert system – Staff lacked knowledge on notifiable diseases and action thresholds – Absence of standard case definition guidelines for use in case patient diagnosis – Lack of case based investigation forms for immediate reporting – Weak laboratory support, referral system for lab specimens |
Conclusion
Our review found 2 parallel surveil- lance systems being used in Rhino Camp Refugee Settlement, non-availability of guidelines on IDSR and lack of training on the same. There were several weaknesses in the core functions of IDSR system.
Public Health Actions
We disseminated our findings to the DHT and partners and immediate actions for improving early detection and response to alerts and outbreaks were agreed upon. We conducted a training of the District Front- line FETP team on IDSR after which they trained
health facility staff on prompt case detection and re- porting.
Strengths and Gaps identified in the existing Surveillance Systems
Mentorship visits to the facilities by the Frontline FETP team were conducted to reinforce the skills passed on in the training. A meeting was planned to strengthen the district coordination role in regard to Implementing Partner activities
Recommendations
We recommend training of health facility staff on IDSR guidelines and implementation. Minis- try of Health should urgently work with UNHCR to harmonize guidance on disease surveillance in Rhino Camp Refugee Settlement and other refugee settings. Arua District Local Government should coordinate the activities of the different partners to maximize efficient use of resource.
Comments are closed.