
Cutaneous and Gastrointestinal Anthrax Out-break Caused by Handling Meat from Infected Carcass, Makutano Village, Kween District, Uganda, May 2018
Authors: Kenneth Bainomugisha*1, Esther Kisaakye1, Lilian Bulage1, Alex R. Ario1; Affiliation: 1 Uganda Public Health Fellowship Program, Kampala, Uganda
Summary
On 15th May 2018, the District Health Officer (DHO) of Kween notified Ministry of health of a suspected case of anthrax in Ma- kutano, a nearby village to Kaplobotwo where an anthrax out- break had been confirmed in April, 2018. Both Makutano and Kaplobotwo villages are located in Ngenge sub-county, Kween District along Moroto highway. We investigated to confirm the existence of the outbreak, estimate the magnitude of the out- break and identify exposure factors for evidence-based control measures. We identified four case-persons of which 4/4 had cutaneous anthrax and ¼ had both cutaneous and gastrointestinal anthrax, with no deaths. ¾ case-persons reported having participated in skinning and dissecting of cows that died suddenly on 1st May 2018 and 8th May 2018. The fourth case, a child, played around the site where the dead cow was slaughtered on the 8th May 2018. We recommended treatment of sick animals, vaccination of all healthy animals, in Ngenge sub-county, safe burial of carcasses, community mobilization and sensitization about anthrax.
Background
Anthrax is a zoonotic disease caused by Bacillus anthracis. On 15th May 2018, the District Health Officer (DHO) of Kween notified Ministry of health of a suspected case of anthrax in Makutano, a nearby village to Kaplobotwo where an anthrax outbreak had been confirmed in April, 2018. Both Makutano and Kaplo- botwo villages are located in Ngenge sub-county, Kween District along Moroto highway. Makutano village is approximately
8Kms away from Kaplobotwo. The suspected case, a 30 year old male, presented with swelling on the skin on the left hand, edema, and, a swollen chest (left side) at Ngenge Health centre three. We investigated, to confirm the existence of the out- break, estimate the magnitude of the outbreak, identify expo- sure factors for evidence-based control and prevention measures.
Methods
We defined a probable cutaneous anthrax case as acute onset of skin lesions (e.g., papule, vesicle or eschar) in a person re- siding in Makutano village; Kween District from 15th April onwards. A probable gastrointestinal anthrax case as acute onset of abdominal pain and any of the following: non bloody and bloody diarrhea, vomiting. Pharyngitis, oesopharygeal lesions and lymphadenopathy. A confirmed anthrax case as a suspected case with PCR-positivity for Bacillus anthracis from a clinical sample i.e. swab from skin lesions/vesicles and blood. We actively searched for cases in Makutano village and conducted in- depth interviews with chairman Local Council 1of Makutano village and the owners of the cows. We conducted environmental assessments to obtain information; on presence of sick cows in the area. We had in-depth interviews with the owners of the dead cows, and the area police officer on how the meat from the dead cows was distributed and how the remains were dis- posed off. Because the case-persons had taken antibiotics we did not carry out laboratory diagnosis. Additionally, an anthrax outbreak had already been confirmed in the same month in Kaplobotwo village, located within the same sub-county (Ngenge) as Makutano.
Findings
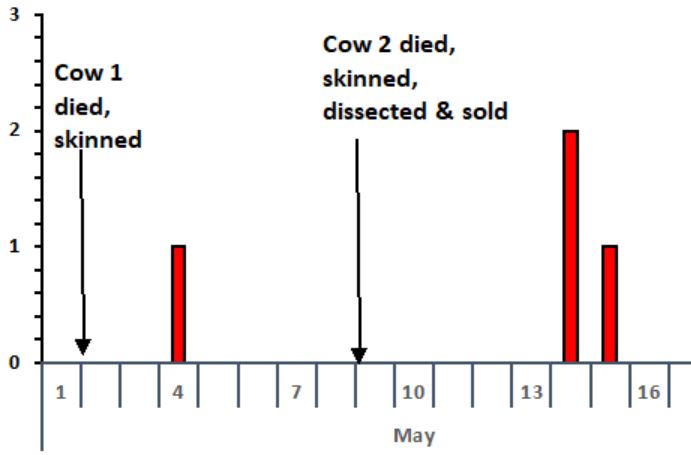
We line listed 4 cases. All four case-persons developed symptoms of cutaneous anthrax and one of the four case-persons had gastrointestinal anthrax. 3/4 case-persons reported having participated in skinning and dissecting of cows that died suddenly on 1st May 2018 and 8th May 2018. The fourth case, a child, played around the site where the dead cow was slaughtered on the 8th May 2018. All case-persons were males, median age 29 years, range 5-50 years. No deaths were recorded during the period of our investigation. The epidemic curve showed two point source anthrax outbreaks. The first point source outbreak had one case that occurred on 4th May 2018 while the second point source outbreak had three cases that occurred from 14th to 15th May 2018 (Figure 1). 2/4 carcasses tested positive for Bacillus anthracis by Rapid Diagnostic Test (RDT).

Discussion
This was a cutaneous and gastrointestinal anthrax outbreak likely associated with handling with cows that died suddenly. The out- break in Makutano village happened barely three weeks after an- other outbreak in Kaplobotwo village both in Ngenge sub-county. Anthrax is a known zoonotic disease that affects both livestock and wild animals and is acquired through handling and eating meat from infected animals. This outbreak occurred after the village members handled and ate meat from infected animals. This illustrated the need for village cross-border surveillance and prompted actions to avert export of disease from one geographical area to another. Meat from both carcasses under this study was sold and transported to a neighboring district of Bulambuli creating a risk of spread across districts.
Conclusions and recommendations
These were two point source outbreaks of both cutaneous and gastrointestinal anthrax likely associated with handling meat of cows that died suddenly. We recommended treatment of sick animals, vaccination of all healthy animals, in Ngenge sub-county and surrounding areas, safe burial of carcasses, community mobilization and sensitization about anthrax.
References
1. Anthrax disease – Google Search [Internet]. [Cited 2018 Jun 11]. Available from: https://www.google.com/search?
q=anthrax+disease&oq=Anthrax&aqs=chrome.4.69i59j0l5.48 02j0j8&sourceid=chrome&ie=UTF-8
2. Vieira AR, Salzer JS, Traxler RM, Hendricks KA, Kadzik ME, Marston CK, et al. Enhancing Surveillance and Diagnostics in Anthrax-Endemic Countries. Emerg Infect Dis. 2017 Dec; 23 (Suppl 1):S147–53.
3. Kelly K. Medicine Becomes a Science: 1840-1999. Infobase Publishing; 2010.
4. Manchee RJ, Broster MG, Stagg AJ, Hibbs SE. Formaldehyde solution effectively inactivates spores of Bacillus anthracis on the Scottish island of Gruinard. Appl Environ Microbiol. 1994; 60(11):4167–4171.
5. Siegel JD, Rhinehart E, Jackson M, Chiarello L, Committee HCICPA. 2007 guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007; 35(10):S65–S164.
6. Manguvo A, Mafuvadze B. The impact of traditional and religious practices on the spread of Ebola in West Africa: time for a strategic shift. Pan Afr Med J. 2015; 22(Suppl 1).
Comments are closed.