
Animal bite patterns and delays in initiating post exposure prophylaxis associated with vaccine stock outs at Arua Regional Referral Hospital, Arua District, Uganda: 2014-2018
Authors: Fred Monje1, Daniel Kadobera1, and Alex Riolexus Ario1: Affiliations: 1Uganda Public Health Fellowship Program, Ministry of Health, Kampala, Uganda
Summary
Although Northern Uganda had the highest incidence of animal bites at 76 per 100,000, among all the regions in 2001-2015 rabies surveil-lance data analysis, rabies Post Exposure Prophylaxis (PEP) usage was not indicated – whether timely or not. We described patterns of animal bite victims seeking PEP at Arua Regional Referral Hospital (ARRH), established proportions of timely initiation of PEP and predictors of delayed PEP initiation in Arua District. We identified 1,411 animal bites in Arua District during the period 2014-2018; with an overall incidence of 17/ 10,000population. Of 1,411 animal bites, 21% (294) had timely initiation of PEP at ARRH. 29% (275/952) of animal bite victims received timely PEP when there was availability of rabies vaccine compared to 4% (19/459) who received timely PEP when there was a stock out of rabies vaccine (AOR=8.8; 95%CI:5.4-14). There was low timely initiation of PEP among animal bite victims in Arua District associated with stock-outs of rabies vaccine at ARRH. We recommended increasing availability of rabies vaccine at ARRH guided by animal bites data from the veterinary department; and sensitization of the public about PEP to minimize the dangers of animal bites/rabies in humans.
Background
In Uganda, research indicate that 41% of patients exposed to rabies virus through animal bites do not complete their course of PEP (1). It is also possible that more animal bite victims do not initiate or delay to initiate PEP after an animal bite injury in Uganda. Further-more, descriptive rabies surveillance data analysis conducted from 2001-2015 in Uganda based on data routinely collected at health facilities revealed that Northern region in Uganda had the highest incidence (/100,000) of animal bites at 76, among all other regions, with significant increase in suspected deaths associated with rabies (2). Within Northern region, Arua District consistently reported high numbers of animal bites from 2014 – 2018 but without information regarding adherence and delays of PEP and associated factors at health facilities. We described patterns of animal bite victims seeking PEP at Arua Regional Referral Hospital (ARRH), established proportions of timely initiation of PEP and predictors of delayed PEP initiation in Arua District to guide control interventions.
Methods
We conducted a retrospective cohort study at ARRH located in Arua District, Northern Uganda. We reviewed Outpatient registers (HMIS 031) and extracted animal bites data at ARRH from 2014-2018. We also conducted Key informant interviews (KII) with the Outpatient Department head, Hospital Pharmacist, and the head of the Medicine stores at the Hospital. We abstracted data on timely initiation of PEP (Vaccine initiation < 48 hours) or delayed initiation of PEP (Vaccine initiation ≥ 48 hours or not receiving vaccine at all) as our dependent variable. The independent variables were date of initiating PEP, residence, age, sex, diagnosis, knowledge gap of the patients, rabies vaccines stock-out cost of the vaccine, and technical capacity. We described animal bite patterns by person, place, and time. Using QGIS, we drew a map of Arua District to show the spatial distribution of animal bites victims at ARRH based on their recorded areas of residences. Proportions of animal bite cases was generated and subjected to a Chi-Square test to test significant differences. We used logistic regression to identify predictors of delayed initiation of PEP. Qualitative data was summarized as themes and sub-themes.
Results
We identified 1,411 animal bites in Arua District during the period 2014-2018; with an overall incidence of 17 /10,000 population. Of 1,411 animal bites, 21% (294) had timely initiation of PEP. Among 294 animal bite victims who received timely PEP at ARRH, the majority were children aged 6-17 (Incidence/10,000=5.3). Dadamu sub-county was the most affected (Incidence/10,000=11) (Figure 1).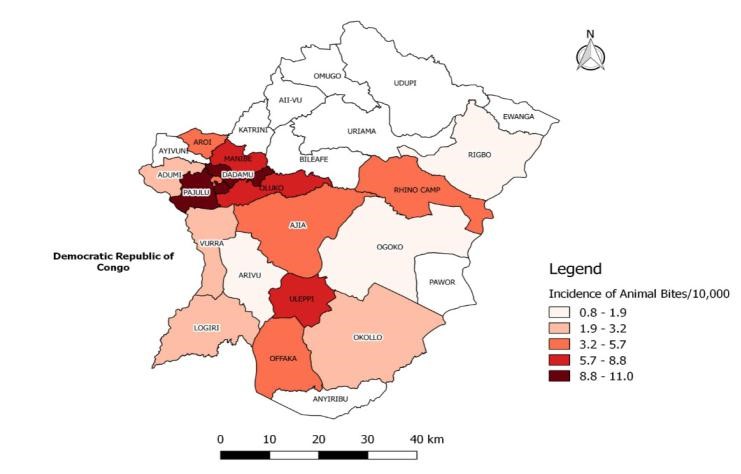
Figure 1: Map of Arua District showing incidence of animal bites among victims who sought healthcare at Arua Regional Referral Hospital, 2014-2018
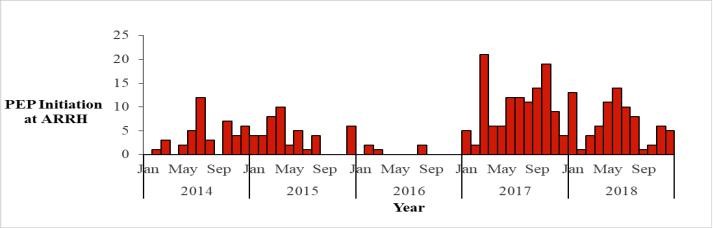
PEP initiation at ARRH showed variations in different years with the peaks occurring between March-October during the study period, 2014-2018. For instance, PEP initiation was highest in the month of July in 2014; highest in the month of April in 2015; highest in the month of August in 2016; highest in the months of March and October in 2017; and highest in the month of June in 2018 (Figure 2).
Factors associated with timely initiation of PEP among animal bite victims
In logistic regression, 29% (275/952) of animal bite victims received timely PEP when there was availability of rabies vaccine compared to 4% (19/459) of animal bite victims who received timely PEP when there was a stock-out of rabies vaccine (AOR=8.8; 95%CI:5.4-14). Besides, 28% (106/375) of animal bite victims staying ≤ 20km away from ARHRH received timely PEP compared to 18% (188/1036) of animal bite victims staying > 20km away from ARRH (AOR=1.4, 95%CI: 1.1-2.0). Furthermore, one Key informant at ARRH said, “As a referral hospital, we could be having enough rabies vaccines all the time, but many times, patients for dog bites come here and don’t find vaccines”.
Discussion
Our epidemiologic investigation demonstrated that there was low timely initiation of PEP associated with stock-outs of rabies vaccine at ARRH and long distance of patient residence away from ARRH. Besides, most patients who sought for PEP at ARRH were Children aged 6-17 years during the study period.
The WHO recommends that all animal bite victims be given immediate PEP after rabies exposure (3). However, in our study, there was delayed initiation of PEP associated with stock-outs of rabies vaccine and long distance of patients away from ARRH. Previous studies have also pointed out that rabies vaccine stock-outs was associated with low uptake of rabies vaccine at health facilities among animal bite victims (4). Rabies vaccine stock- outs at health facilities may discourage animal bite victims seeking for PEP services from returning to health facilities for PEP due to the long distances and transport costs incurred by the poor farmers.
Past studies have indicated that following an animal bite, the majority of animal bite victims who received PEP services were children (5). In our study, most animal bite victims accessing rabies vaccine were children probably because this was a school going age-group who could have been bitten by stray dogs when going to school- hence prompting them to seek for PEP services.
Our study also showed that PEP initiation had peaks occurring between March-October during the study period, 2014-2018. The period March – October in the study period corresponds to the rainy season in Arua District and Uganda in general. Rainy seasons are associated with mating and breeding in dogs as indicated by a study in Kenya (6). Rainy seasons are usually associated with abundance of resources such as food possibly that’s why mating and breeding occurs in this season. In mating season, dogs’ instincts to multiply are at their sharpest and often lead to behavior-al changes- including the urge to bite in an attempt to protect the female dogs. Thus, any human who approaches or moves near such a pack is perceived to be a threat and bitten. The year 2016 was characterized by few people or the least number of people accessing PEP. However, it is not clear why few persons accessed during 2016.
Conclusion and Recommendations
Our investigation demonstrated that there was low timely initiation of PEP among animal bite victims in Arua District associated with stock-outs of rabies vaccine at ARRH. We recommended increasing availability of rabies vaccine at ARRH guided by animal bites data from the veterinary department; and sensitization of the public about PEP usage to minimize the dangers of animal bites/rabies in humans.
References
1. Fèvre EM, Kaboyo RW, Persson V, Edelsten M, Coleman PG, Cleaveland S. The epidemiology of animal bite injuries in Uganda and projections of the burden of rabies. Trop Med Int Health. 2005 Aug;10(8):790–8.
2. Masiira B, Makumbi I, Matovu JKB, Ario AR, Nabukenya I, Kihembo C, et al. Long term trends and spatial distribution ofanimal bite injuries and deaths due to human rabies infection in Uganda, 2001-2015. PLOS ONE. 2018 Aug 21;13(8):e0198568.
3. Crowcroft NS, Thampi N. The prevention and management of rabies. BMJ. 2015 Jan 14;350:g7827.
4. Changalucha J, Steenson R, Grieve E, Cleaveland S, Lembo T, Lushasi K, et al. The need to improve access to rabies post-exposure vaccines: Lessons from Tanzania. Vaccine [Internet]. 2018 Oct 8 [cited 2019 Aug 21]; Available from: http://www.sciencedirect.com/science/article/pii/S0264410X1831243X
5. Penjor K, Tenzin T, Jamtsho RK. Determinants of health seeking behavior of animal bite victims in rabies endemic South Bhutan: a community-based contact-tracing survey. BMC Public Health. 2019 Feb 27;19(1):237.
6. Digital S. Why dogs bite during the rainy seasons | Smart Farmer [Internet]. [cited 2019 Aug 22]. Available from: https://smartfarmerkenya.com/why-dogs-bite-during-the-rainy-seasons/
Comments are closed.