
Analysis of Surveillance data to determine distribution of Human Brucellosis in Uganda, July 2015 to June 2017
Authors: Patricia Eyu1, Edridah M. Tukahebwa2, Benon Kwesiga1, Alex R. Ario1; Affiliations: 1Uganda Public Health Fellowship Program, 2Neglected Tropical Diseases, Control Program, Ministry of Health
Summary
Brucellosis is a common zoonosis in Uganda with a human sero- prevalence of 17%. We analysed surveillance data reported from all levels of health facilities into the Health Management Information System (HMIS) to identify the populations at risk and evaluate geographical distribution of brucellosis in Uganda between July 2015 and June 2017. Monthly and annual district level aggregated data on brucellosis prevalence was obtained from HMIS for 112 districts. The prevalence of brucellosis was nearly twice as high among females (512/100,000) than among males (269/100,000). The age- group 60+ years (906/100,000) had a higher prevalence than other age groups. Northern Uganda had the highest prevalence (313/100,000) compared to Eastern (248/100,000), Central (278/100,000) and Western (228/100,000) regions. Kotido and Lyantonde districts had the highest prevalence of brucellosis over the years ranging between 350-1000/100,000 persons. We recommend increasing sensitisation about the mode of transmission and how to prevent brucellosis transmission targeting females, elderly and districts with high prevalence.
Introduction
Brucellosis is the most common bacterial zoonosis worldwide with more than 500 million estimated new cases each year. Brucellosis has major economic consequences due to time lost by patients from normal daily activities [5] and losses in animal production [6]. World Health Organisation (WHO) Global and Re- gional Disease Estimates done in 2015 showed that Brucella species resulted in 0.83 million illnesses with almost 333,000 chronic infections [7]. Possible risk factors for brucellosis include; consuming locally processed milk products, residing in rural areas, being elderly and being an agro pastoralist, among others [8, 9].
The Integrated Disease Surveillance and Response guidelines categorises the laboratory criteria for diagnosis of brucellosis into two; definitive (blood culture) and presumptive (Brucella total antibody titer or Brucella micro agglutination test) [10]. In Uganda, routine diagnosis of brucellosis in health facilities is mainly by serology using the Brucella Agglutination Test (BAT). There is scanty information on national level prevalence of human brucellosis in Uganda, and yet all health facilities and district level prevalence is re- ported in the District Health Information System (DHIS2) every month. We therefore conducted an analysis of surveillance data from all levels of health facilities reported in the DHIS2 to identify the populations at risk and determine the geographical distribution of human brucellosis in Uganda between July 2015 and June 2017.
Methods
Monthly and annual district level aggregated data on brucellosis prevalence was obtained from the district health information system (DHIS2) of Uganda from 112 districts. Brucellosis episodes are reported by age group (<5 years, 5-59years and 60 years), sex (male and female), period, region and districts from July 2015 to date. Brucellosis data was extracted from the Health Management Information System form 105 Out Patient Department (HMIS 105 OPD) from 2521 health facilities. The abstracted data was cleaned and exported to Epi-info version 7.2.0. The 2014 National Population and Housing Census data was extrapolated using an annual growth rate of 3.03% to carryout descriptive analysis on person, place and time characteristics. Prevalence was calculated per 100,000 persons and distribution of age and sex was carried out to describe the person characteristics. QGIS was used to map brucellosis in the districts of Uganda.
Findings
Distribution of brucellosis by sex between July 2015 and June 2017
Brucellosis prevalence is nearly twice as high among females com- pared to males.
| Sex | Cases | Population | Prevalence/100,000 |
| Male | 35,597 | 18,353,190 | 194 |
| Female | 69,557 | 18,905,034 | 367 |
| Total | 105,154 | 37,258,224 | 282 |
Table 1: Distribution of brucellosis by sex between July 2015 and June 2017
Distribution of brucellosis by age between July 2015 and June 2017
The prevalence of brucellosis increases with increase in age with children (<5 years) having the lowest prevalence at 55/100,000 and adults above 60 years with the highest prevalence of 889/100,000.
| Age in
years |
Cases |
Population |
Prevalence/ 100,000 |
| 0 to 4 | 3,622 | 6,631,964 | 55 |
| 5 to 59 | 88,280 | 29,135,932 | 303 |
| 60+ | 13,252 | 1,490,329 | 889 |
| Total | 105,154 | 37,258,225 | 282 |
Table 2: Distribution of brucellosis by age between July 2015 and June 2017
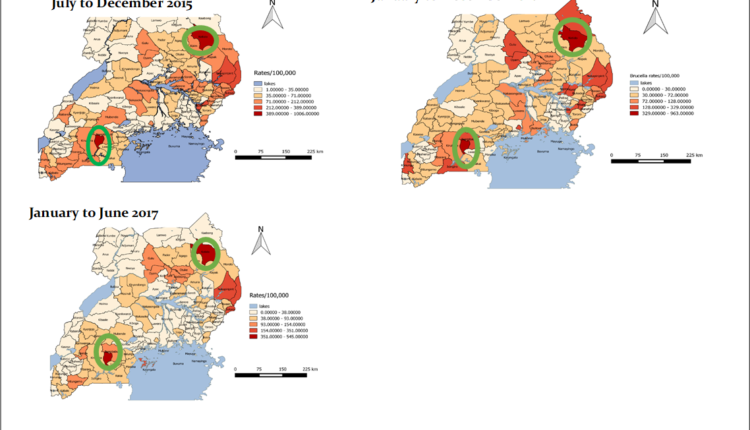
Distribution of brucellosis by region between July 2015 and June 2017
The prevalence of brucellosis between July 2015 and June 2017 is highest in the Northern region of Uganda. Lyantonde () and Kotido () Districts had the highest prevalence of Brucellosis over the years .
| Region | Cases | Population | Prevalence/ 100,000 |
| Central | 28,487 | 10,251,066 | 278 |
| East | 24,168 | 9,727,385 | 248 |
| North | 24,185 | 7,732,640 | 313 |
| West | 21,790 | 9,547,133 | 228 |
Table 3: Distribution of brucellosis by region between July 2015 and June 2017
Discussion
This analysis shows that females are almost three times more affected than males with human brucellosis. These findings contradict findings of a study carried out in Central Greece that showed that males had a higher incidence compared to females [11]. Also another cross sectional study carried out in Kiboga district of Uganda showed that the prevalence of brucellosis was higher among males compared to females [8]. Another cross sectional study carried out in Volta region of Ghana also showed a brucellosis prevalence of 88.9% in males [12]. The prevalence of brucellosis in our study could be higher in females compared to males because the data set is obtained from health facility records and it is known that women have better health care seeking behaviour and could surely have higher reporting compared to males [13]. The findings of these three studies could also contradict our findings because they were carried out in cattle keeping communities which increase the risk in males since they are the ones involved in handling cattle.
This analysis also shows that persons aged 60years and above have a high- er prevalence compared to persons aged 5-59years and 0-4years. This is consistent with a study carried out in Kiboga district in Uganda which showed an increased risk in the elderly above 60years [8]. These are in line with findings from another study in Bangladesh which showed an increasing risk among older persons [14]. The higher prevalence in the elderly could also be because of the traditional role of the elderly in cattle keeping in Ugandan communities.
Kotido and Lyantonde districts had the highest prevalence of brucellosis over the years. These are districts whose habitats are mainly cattle keepers. It is also known that Karimojong who also inhabit Kotido have cultural practices of consuming raw milk mixed with raw blood as a delicacy [15].
Conclusion and recommendations
The prevalence of brucellosis is higher among females compared to males. Elderly persons above 60years of age had a higher prevalence of brucellosis compared to younger people while Kotido and Lyantonde districts had the highest prevalence of brucellosis over the years. We recommended further studies to be conducted to identify risky behaviours for brucellosis among most affected groups and increased awareness about prevention of brucellosis transmission targeting females, elderly and districts with high prevalence.
References
- WHO, WHO recommended standards and strategies for surveillance, prevention and control of communicable diseases., in Zoonoses and Veterinary Public Health. 2017: Geneva
- CDC, Infectious Diseases Related to Travel: Brucellosis, C.f.D.C.a. Prevention, 2017: Atlanta, USA.
- Makita, K., et al., Spatial epidemiology of hospital-diagnosed brucellosis in Kampala, International Journal of Health Geographics, 2011. 10: p. 52-52.
- David, L., Heymann., Control of Communicable Diseases manual. Vol. 20th Edition. 2015, Washington: American Public Health Associ Corbel, M., J., Brucellosis in humans and animals. 2006: Geneva 27, p. 102.
- Felix, R., et al., Human health benefits from livestock vaccination for brucellosis: case 2003: p. 17.
- Kirk, M.D., et al., World Health Organization Estimates of the Global and Regional Disease Burden of 22 Foodborne Bacterial, Protozoal, and Viral Diseases, 2010: A Data Synthesis. PLoS Medicine, 12(12): p. e1001921.
- Tumwine, G., et al., Human brucellosis: sero-prevalence and associated risk factors in agro-pastoral communities of Kiboga District, Central BMC Public Health, 2015. 15(1): p. 900.
- CDC, Brucellosis 2010 Case Definition, in National Notifiable Diseases Surveillance System (NNDSS). 2010: Atlanta, USA.
Comments are closed.