
An investigation of increasing Schistosomiasis cases in Oyam district, Northern Uganda, April 2017
Authors: Kizito Susan1, Eyu Patricia1, Adriko Moses2, Tukahebwa Edridah2, Kwesiga Benon1, Alex R. Ario1; Affiliations: 1Public Health Fellowship Program - Field Epidemiology Track, 2Vector Control Division - Ministry of Health
Summary
In March 2017, Oyam District Health Office reported to Ministry of Health an increased number of people suspected to be dying of Schistosomiasis in four sub-counties. We conducted an investigation to determine the scope and source of schistosomiasis infection; possible risk factors; and identify the challenges for schistosomiasis control so as to guide control measures. We identified a total of 82 suspected cases and confirmed 30. Males were more affected compared to females. Children between 5 and 14 years were most affected followed by children less than 5 years. Bathing and stepping in unsafe water sources without protective gear was a risk factor for schistosomiasis infection, as well as non-schooling among school age children. We recommended introduction of praziquantel to children younger than 5 years, provision of safer water sources like construction of more boreholes in the affected communities, more sensitization and health education about schistosomiasis and preventive chemotherapy with praziquantel.
Introduction
In March-2017, the Ministry of Health through the Emergency Operation Center received communication from Oyam District of increasing deaths of suspected schistosomiasis in 4 sub-counties of Otwal, Minakulu, Aleka and Myene in a period of 5 months.
Oyam district is located in Northern Uganda and is endemic for 2 schistosoma species: Schistosoma mansoni and S. heamatobium that causes intestinal and urinary schistosomiasis respectively.
The district has been conducting annual preventive chemotherapy through mass drug administration (MDA) using praziquantel since 2006 in both schools and communities as per World Health Organisation (WHO) recommendations, however treatment coverage was 60.8% in 2016 against the recommended 75% (2).
Praziquantel uptake had been resisted in many communities due the adverse side effects it causes yet majority of the population in the affected sub-counties have limited access to safe water sources like boreholes or piped water.
Methods
We defined a suspected schistosomiasis case as onset of ≥3 of the following symptoms: abdominal pain, abdominal distention, blood in urine, blood in stool, bloody diarrhea, vomiting blood, diarrhea, in a resident of Oyam district from 1st January 2001 onwards while a confirmed schistosomiasis case was defined as a suspected case with a positive rapid diagnostic test for circulating cathodic antigen in urine (CCA).
We actively identified cases from the affected communities and reviewed both health center records and Village Health Team (VHT) records in four sub- counties. We reviewed health center records from 3 health facilities and then generated hypotheses from descriptive epidemiology.
We conducted a case control study where cases and controls were frequency matched by age group. We collected urine samples for testing schistosomiasis and also carried out an environmental assessment in the community.
Results
We identified 82 suspected cases and con- firmed 30, with 12 recorded deaths from 2001 to April 2017. Children under 15 years made up 70% of cases of which 21% were below 5 years.
The median age was 8 years (range 2-72). Study population had 18 (42%) stay home children while 16 (37%) were pupils and 9 (21%) were farmers. Six out of 12 suspected schistosomiasis deaths occurred in the last 3 years alone.
Males were more affected with a prevalence of 0.1% compared to females (0.04%). Children between 5 and 14 years were most affected (prevalence = 0.11%) followed by children less than 5 years (prevalence = 0.07%) and people 15 years and above were least affected (prevalence= 0.04%).
Figure1: Distribution of symptoms of schistosomiasis among cases
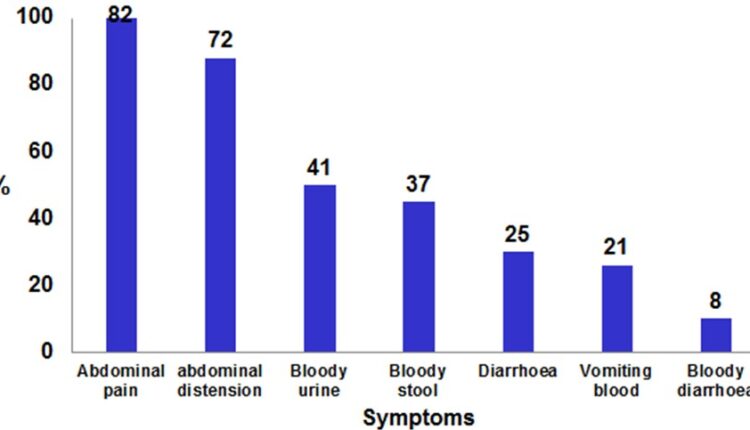
Figure 2: Map showing attack rates/10,000 of schistosomiasis cases in Oyam District, April 2017
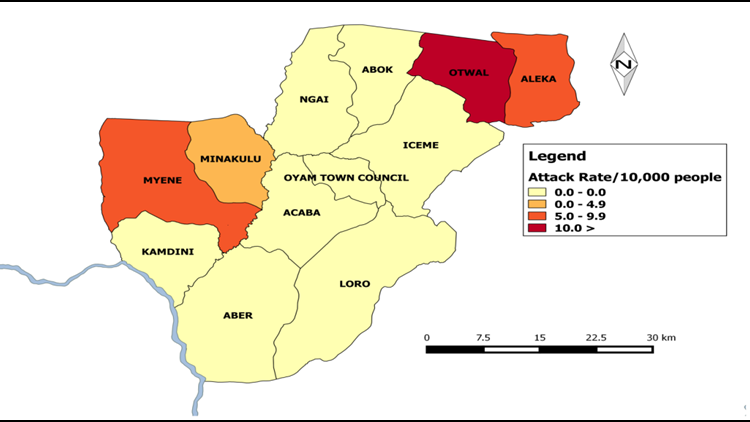
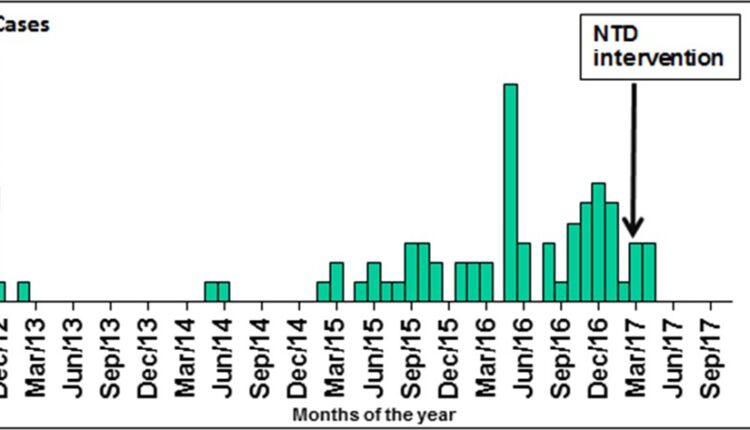
Figure 3: Increasing number of cases over time with a peak in May 2016.
Laboratory findings
36 urine samples were collected and 30 tested positive using the CCA rapid test kit.
Environmental assessment
The streams, wells and the dams here referred to as unsafe water sources were infested with water snails. Residents who were mostly barefooted stood in these water sources while bathing, washing clothes, fetching of water for home use.
Case control findings
The risk factors for schistosomiasis morbidity were bathing from unsafe water sources, (OR: 19, 95% CI: 8.4 – 40.6), comparing 49/21cases/controls; fetching water from unsafe water sources (OR: 3.9, CI: 2.0 – 7.5) comparing 42/42 cases/ controls and not going to school among school-age children (OR:3.7, CI: 95% CI 1.7 – 7.8) among 43/102 cases/control.
Discussion
This investigation documents an upsurge of schistosomiasis infection in the district over the last 5 years. During the political insurgency in northern Uganda between 1987 and 2007 (2), Oyam district was largely an internally displaced people’s camp. Many people were forced into the area and were living in water- stressed conditions. Rescue missions constructed valley dams (2) to improve on water supply for domestic animals but the dams are now reservoirs for fresh-water snails that are schistosomiasis vectors.
Despite the annual provision and distribution of free praziquantel, drug uptake is still low. The lack of sufficient safe water sources as well as the difficulty of having to make long queues at the few and distant boreholes compel residents to opt for the unsafe water sources. At the open streams, dams and wells, mostly male children were seen swimming or bathing in the water bodies (1). We did not ob- serve any toilets built near these water bodies and we assumed that the community uses the same water bodies or bushes around them as toilets. An infected person urinating and defecating in or near the water bodies completes the life cycle of schistosomiasis.
It is this pro- longed and recurrent exposure to unsafe water that permitscercariae from the snail vector to enter the human host and thus poses a great risk to their families to ac- quire schistosomiasis. Since the integration of Neglect- ed Tropical Disease programs with Ministry of Health activities in 2007, there has been increased countrywide distribution of Mass Drug Administration at the community level for the control of schistosomiasis but coverage still remains below 75% recommended by WHO (2).
Children below five years are at very high risk of infection yet Uganda has no policy on administration of praziquantel to children below 5 years. If these children continuously get new or recurrent schistosomiasis infections at such an early age they are even more prone to developing complications like anemia, malnutrition, poor mental development etc. This will lead to frequent school absenteeism which affects performance.
The access to alternative safer water sources is a big challenge and the provision of protective wear as a barrier method in contaminated water sources is unaffordable. We how- ever think that the provision of a child palatable formulation (3) as well as clinical involvement in addressing schistosomasis among children less than 5 years from the sub-county level and above will go a long way in targeting control among this age group and contribute towards breaking the viscous cycle.
Much as the application of chemical molluscides was the key strategy for schistosomiasis control in the 1950s and 1970s in many parts of Africa, S. America and Asia, it is not environmentally friendly to the eco-system and not feasible in our large fresh water bodies (4).
Conclusions and Recommendations
There was an increase in cases of Schistosomiasis reported in 4 sub- counties in Oyam district. Children under 15 years were most affected because of their frequent entry into streams barefoot while swimming/bathing. Water sources used by the affected villages were infested with water snails believed to be intermediate hosts for schistosomiasis worms.
Stepping in unsafe water sources (dams, streams and wells) without protective gear; bathing from unsafe water sources and not going to school increased the risk of acquiring schistosomiasis infection. Schistosomiasis was not being routinely diagnosed among the patients who had visited the health facilities.
We recommended introduction of praziquantel to children younger than 5 years, provision of safer water sources like construction of more boreholes in the affected communities, more sensitization and health education about schistosomiasis and preventive chemotherapy with praziquantel.
References
- Update of Mass Drug Administration Program for Schistosomiasis Control in Koome Islands, Central Uganda. Doreen Tuhebwa, James Bagonza, Elizabeth Ekirapa Kiracho, Adoke Yeka,Alison M Elliot, Fred s.l. : PLOS One, 2015.
- Roots of the Conflict in Northern Kisekka-Ntale, Fredrick. s.l. : The Journal of Social, Political and Economic Studies, 2007, Vol. 32.
- Impact of human schistosomiasis n sub-Saharan Abio- la Fatimah Adenowo, Babatnji Emmanuel Oyinloye, Bolajoko Idiat Ogunyinka, Abidemi Paul Kappo. s.l. : The Brazilian Journal of Infectious Diseases, 2015, Vol. 19.
- Safety and efficacy of praziquantel syrup (Epiquantel) against Schistosoma heamatobium and Schistosoma mansosni in pre- school-aged children in Niger. Amadou Garda, Mariama S. Lamine, Ali Djibo, Almoustrapha Tahirou,Madamadou Abou- bacar Aouami, Aichatou Alfari, Anna E. Phillips, Alan Fenwick, Jurg Niger : Elservier, 2012.
Comments are closed.