
A 31.9% Laboratory Test Menu Fulfillment Rate in District Health Information System Version 2 (DHIS-2), July 2022-June 2023, Uganda
Authors: Shem Mwebaza* 1,2, Samuel Gidudu1, Bannet Muwanguzi2, Lilian Bulage1, Lali William1, Alex Riolexus Ario1 Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Mildmay Uganda, Kampala, Uganda Correspondence*: Tel: +256702987664, Email: smwebaza@uniph.go.ug
Summary
Background: In 2011, the Uganda Ministry of Health (MoH) and National Health laboratory and Diagnostic Services (NHLDS) launched the national test menu guidelines to standardize the number of testing techniques conducted by medical laboratories at each tier of the health system. Since the launch of the said guidelines, the percentage of laboratory tests or procedures on a laboratory’s menu that are actually performed (test menu fulfillment rate) has not been evaluated. We evaluated the laboratory test menu fulfillment rate at the various health center levels in Uganda, July 2022-June 2023.
Method: We abstracted and analyzed laboratory testing data (July 2022 to June 2023) reported in District Health Information System-2 (DHIS2) by 2,278 health facilities. Test menu fulfillment rate was calculated by dividing reported number of test techniques with that expected per the national test menu at each health facility level. We assessed ability to enter specific tests in DHIS-2 by screening and comparing various test nomenclatures in laboratory diagnostics reference materials (A total of 146 testes should be provided at RRH level and below in Uganda). Results: A total of 28,190 out of 88,234 test techniques were reported to have been conducted by the health facilities, resulting in a national laboratory test menu fulfillment of 31.9%. Regional Referral Hospitals had the highest test menu Fulfillment rate of 35.7 % (834/2336) followed by GHs with a rate of 35.3% (5374/15215), HCIIIs at 30.2% (17298/57288) and HCIVs at 29.6% (3966/13395). A total of 68 of the specific 146 tests (46.5%) had No Specific area for Entry (NSE) into DHIS2.
Conclusion: A sub-optimal national laboratory test menu fulfillment rate for the period July 2022 to June 2023 was noted.
Background
The Ministry of Health (MoH) strategic plan 2020/21 – 2024/25 (1) and Health Sector Strategic and Investment Plan (HSSIP) 2015/16-2019/20 (1) identify laboratory services as a key driver for effective delivery of the Uganda National Minimum Health Care Package (UNMHCP) (2); and as a critical component for effective disease control and prevention. Uganda health laboratory services are designed to support UNMHCP at various levels of healthcare, with the complexity of tests performed rising in accordance with the level of healthcare. Strategic objective III of the National Health Laboratory Services Strategic Plan III (2021-2025) (2) sets out ensure provision of quality and equitable laboratory services at all levels to support clinical care, public health services, and research.
An efficient laboratory system strategically identifies laboratory diagnostic tests and procedures that could be conducted at various health care levels and those that need to be outsourced. This results in cost savings without negatively impacting patient care. Using data analytics, monthly or annual test volume can be evaluated to inform such decisions with careful consideration being given to the downstream impact on patient care as well as overall healthcare expenditures to identify opportunities for cost savings without compromising clinical efficacy. Ministry of Health through National Health Laboratory and Diagnostic services (NHLDS) formerly referred to as Central Public Health Laboratory (CPHL) developed the first set of national laboratory test menus, test techniques, supplies, and laboratory equipment for each type of test and each level in the health system in 2011. This was in line with the 2008 Maputo Declaration on Strengthening of Laboratory Systems (3). These were later revised in 2013 and in 2017 to reflect the changes in technologies and treatment guidelines.
The Uganda National standard test menu, techniques, and supplies list for laboratories (4) specifies the range of laboratory services provided at the various levels ranging from basic services at health center III (HCIII) laboratory, through health center IV (HCIV) laboratory increasing in complexity in General Hospital (GH) laboratory, Regional Referral Hospital (RRH) laboratory, and to highly specialized testing at national referral laboratory. A total of 146 testes should be provided at RRH level and below in Uganda. The MOH with support of her partners has equipped these laboratories with required commodities, functioning equipment, trained personnel, information systems, and infrastructure coupled with regular technical support supervision using a regionalized approach.
Despite efforts to standardize the Uganda National laboratory test menu, techniques and supplies there has not been an evaluation of the fulfillment rate of the standard. The evaluation findings are critical in providing an insight on access and utilization of laboratory services in the country and hence inform programming for equitable access to laboratory services. We evaluated the fulfillment rate for the Uganda National standard test menu, and techniques in the period July 2022 to June 2023 to inform programming.
Method
We conducted a descriptive study using surveillance data on laboratory test types conducted by health center facilities at health center level III, IV, general hospital, and regional referral hospital that report to MOH through the District Health Information System-2 (DHIS-2) in Uganda.
We abstracted data on laboratory test types from DHIS-2 for the period July 2022 to June 2023; dis-aggregated into test category and health facility level. We obtained information on required test types to be conducted by each health facility level from the Uganda National standard test menu, techniques and supplies list (4).
We assessed ability to enter specific tests in DHIS-2 by screening and comparing the test nomenclature of the expected 146 testes at RRH level and below in laboratory diagnostics reference materials with what is indicated in DHIS2.
We defined test menu fulfillment rate as the percentage of laboratory tests or procedures on a laboratory’s menu that are performed. The fulfillment rate was calculated by dividing the number of test types reported in DHIS2 over the number of expected test types as stated in the national laboratory test menu. Table 1 below details the health facilities (16 regional referral hospitals, 179 general hospitals, 235 health center IVs and 1,848 health center IIIs) considered for the study and the total expected test counts for the different facility levels.
Table 1: Study facilities by level and expected tests
| Health facility level | N (2,278) | Tests on Menu | Total expected test counts (88,234) |
| Regional referral hospital | 16 | 146 | 2,336 |
| General hospital | 179 | 85 | 15,215 |
| Health centre IV | 235 | 57 | 13,395 |
| Health center III | 1,848 | 31 | 57,288 |
The test type was considered based on the following assumptions; health facility conducted all the tests on the national menu at least once in the review period (none reporting and a total of 0 tests done in the review period indicated test type not done), a reported value of 1 and above indicated specific test type as being conducted, test types not expected at the health facility level excluded from the study, combined tests were split up and each counted separately. We also reviewed laboratory parameters reported in DHIS-2 comparing them with the national test menu to identify areas of improvement in the laboratory report section.
This study was reviewed by the US CDC and was conducted consistent with applicable federal law and the US CDC policy. We obtained administrative clearance from the Ministry of health. Since the study didn’t involve human subjects and used publicly available data, we did not seek approval of institutional review boards. All generated records were kept confidential, and password protected.
Results
Laboratory test menu fulfillment rate, Uganda, July 2022-June 2023
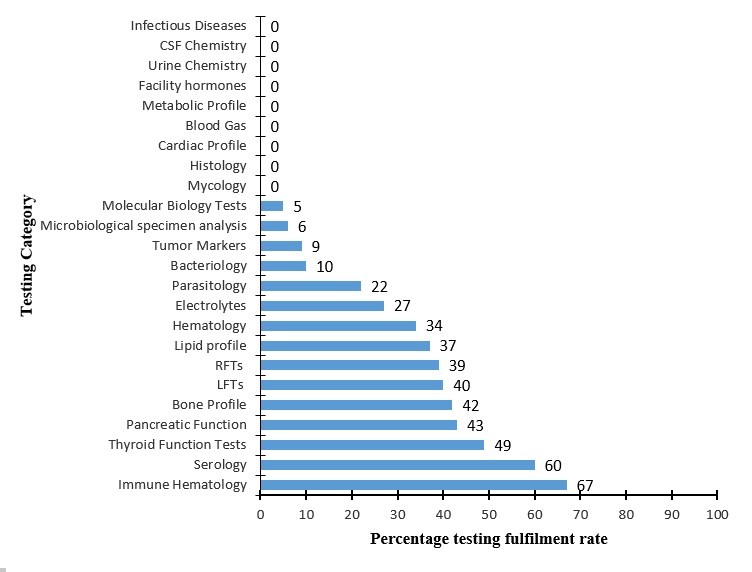
The overall national laboratory test menu Fulfillment rate was 31.9% (28190/88,234). Regional Referral Hospitals had the highest test menu Fulfillment rate of 35.7 % (834/2336) followed by GHs with a rate of 35.3% (5374/15215), HCIIIs at 30.2% (17298/57288), and HCIVs at 29.6% (3966/13395). A total of 68/146 (46.5%) test types had no Specific provision for Entry (NSE) into DHIS-2. Immune hematology (67%), Serology (60%) and Thyroid function (47%), tests were the most performed tests nationally (Figure 1).
Discussion
The evaluation of laboratory test menu fulfilment rates is crucial for lower health center level(downstream) impact on patient care as well as overall healthcare expenditures. It provides an opportunity to identify opportunities for system improvement and cost saving without compromising clinical efficacy. As such, it is imperative that as a country we continue to assess and update test menu to allow for inclusion of the latest diagnostic technologies and methodologies that align with current medical standards, enhance operational efficiencies by identifying redundant tests or outdated methodologies and allow laboratories to optimize workflow and resource utilization, and to identify tests with very low volume that can result in reagent and supply wastage. This study has demonstrated a low laboratory test menu fulfillment rate across facilities, declining from higher health facility levels (RRHs) to lower facilities generally.
Many HCIVs and HCIIIs primarily rely on DHIS-2 for reporting their data to the national level. This inevitably means that a lot of laboratory testing data is not being well captured for use in informed decision marking. The most performed tests, i.e., Immune hematology (CD4, CD8), Serology (HIV, Syphilis, Pregnancy test, Hepatitis B test, Cryptococcal Antigen) are also supported by donors’ hence likely affected by low availability of resources (reagents, equipment and infrastructure)(5). The large number of tests (68) with NSE into DHIS2 had a negative effect on test menu fulfilment rates. In essence, the rates could improve with the updating of the system to capture all tests being conducted.
Study limitations
This study presented findings as reported in DHIS-2 only. There could be variations in test menu fulfillment rates in laboratory data from other systems.
Conclusion
A sub-optimal national laboratory test menu fulfillment rate for the period July 2022 to June 2023 was noted according to data extracted from DHIS-2. In addition, a large number of laboratory tests (46.5%) have no specific area for entry into DHIS2. There is need for additional studies with a longer review period to consolidate these findings.
Recommendations
We recommended the updating of the DHIS2 to be consistent in test categorization and nomenclature of laboratory tests with the laboratory national test menu to streamline tests names for example TB genexpert/TB DNA PCR. Secondly, for facilities that are not using ALIS or use DHIS-2 and the primary database, it is paramount that we ensure all the test menu is fully captured in DHIS-2. This will ensure that no laboratory data is missed out. Furthermore, because of the difference in testing techniques and requirements, it is important to Indicate test platforms and techniques used to inform supply chain and planning activities. There is need for streamlining and standardisation laboratory testing data reporting in line with who reports what, where, in DHIS2 or ALIS. This will guide on where to look for what and will aid data utilisation for research and decision making.
Conflict of interest
The authors declare that they have no conflict of interest.
Authors Contribution
SM, SG conceived and designed the analysis. SM, BM abstracted and analyzed data. SM, SG, BM, and LW wrote the bulletin. SM, LB, LW, and AA reviewed the bulletin to ensure scientific integrity.
Acknowledgements
We acknowledge the Uganda Public Health Fellowship Program, Central Public Health Laboratories Ministry of Health (CPHL) Uganda, Makerere University School of Public Health. Mildmay Uganda and Baylor Uganda for the technical support and oversight of this project. We also acknowledge the US Centers for Disease Control and Prevention Uganda for implementation support.
Copyright and licensing
All materials in the Uganda Public Health Bulletin is in the public domain and may be used and reprinted without permission; citation as to source; however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- Health sector development plan 2015/16 – 2019/20.
- Uganda National Health Laboratory Services Policy – Thomas-Pizaro-Gaspard signed23Mar2018.pdf [Internet]. [cited 2023 Oct 5]. Available from: https://www.cphl.go.ug/sites/default/files/2019-06/UG%20NHLS%20Policy%20%20LTC%20Final%20draft%20-%20Thomas-Pizaro-Gaspard%20signed23Mar2018.pdf
- The Maputo Declaration on Strengthening of Laboratory Systems [Internet]. [cited 2023 Oct 5]. Available from: https://www.who.int/publications/m/item/the-maputo-declaration-on-strengthening-of-laboratory-systems
- National Standard Test Menu, Techniques and Supplies List for Laboratories.pdf [Internet]. [cited 2023 Oct 5]. Available from: https://www.cphl.go.ug/sites/default/files/2019-06/NSTMT%20TEST%20MENU.pdf
- PEPFAR 2023 Country and Regional Operational Plan (COP/ROP) Guidance for all PEPFAR-Supported Countries [Internet]. 2022. Available from: https://www.state.gov/wp-content/uploads/2023/02/PEPFAR-2023-Country-and-Regional-Operational-Plan.pdf
Comments are closed.