
Descriptive analysis of Rift Valley Fever Outbreaks, Uganda, 2016–2023
Authors: Mariam Komugisha1*, Benon Kwesiga1, Richard Migisha1, Irene Kyamwine 1, David Muwanguzi2, Stella Lunkuse2, Joshua Kayiwa2, , Alex Riolexus Ario1; Institutional affiliations: 1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda; 2Department of Integrated Epidemiology and Surveillance, Ministry of Health, Kampala, Uganda; Correspondence*: Tel: +256773822356, Email: mkomugisha@uniph.go.ug
Summary
Background: Rift Valley Fever (RVF) is a mosquito-borne viral zoonosis of public health concern. Several sporadic RVF outbreaks have been reported in Uganda. We described the trends and spatial distribution of RVF outbreaks in Uganda, March 2016–December 2023 to guide programming.
Methods: We analysed RVF surveillance data from the electronic Public Health Emergency Management (ePHEM) database, Uganda Ministry of Health (MoH). Using the Integrated Disease Surveillance and Response (IDSR) national technical guidelines, a confirmed RVF case was defined as any patient testing positive for either anti-RVF immunoglobulin M(IgM) Enzyme-Linked Immunosorbent Assay (ELISA) antibodies or Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) test. We analysed trends of outbreaks using the Mann-Kendall test and described spatial distribution by region and the cattle corridor district where livestock farming is predominant.
Results: During 2016–2023, a total of 43 RVF outbreaks were reported resulting in 340 cases (116 confirmed), 42 deaths with case fatality rate (CFR) of 12%. There was an increase in number of outbreaks from 2016 – 2023. However, the trend is not significant (p=0.73). Most outbreaks 13/43 (42%) were reported in 2018. RVF outbreaks occurred in all four regions of the country, with the highest number reported in the Western region, 27/43 (63%), followed by the Central region, 12/43 (28%). Sixty percent (26/43) of the outbreaks were reported in the cattle corridor districts. Mbarara 4/43 (9%) and Kiruhura 4/43 (9%) Districts reported the highest number of outbreaks in the cattle corridor. Most outbreaks 29/43 (67%) were reported during the dry season: January and June August.
Conclusion: Sporadic outbreaks of RVF were reported in Uganda every year from 2016–2023. Strengthening efforts to prevent and control RVF in Uganda could reduce the occurrence of RVF outbreaks, particularly in regions and districts with a high number of RVF outbreaks. We recommended MoH to enhance RVF surveillance throughout the year to understand the true burden of the disease. We additionaaly recommended further investigations to identify factors contributing to the occurrence of RVF outbreaks in Uganda.
Introduction
Rift Valley fever (RVF) is a zoonotic viral hemorrhagic fever (VHF) caused by the Rift Valley fever virus (RVFV). Humans commonly contract the infection through contact with sick animals or their products. However, transmission of RVFV from animals to humans can also occur through bites from infected mosquitoes (1).
According to the International Livestock Research Institute, approximately 70% of Uganda’s population is involved in livestock production which increases the risk of transmission of zoonotic diseases from animals to humans. Uganda has experienced several sporadic outbreaks of RVF in both humans and animals. According to the review of RVF on humans and animals, and a report by the Food and Agriculture Organisation (FAO), the disease causes severe illness, and human and animal deaths, and impacts the exportation of livestock and their products from the Horn of Africa where Uganda lies (2, 3).
Rift Valley Fever is among the notifiable diseases that require immediate reporting to the MoH. According to the National Technical Guidelines for Integrated Disease Surveillance and Response (IDSR) in Uganda, RVF is detected using Event Based Surveillance (EBS) which is implemented at community, health facility, district, and national level at the Public Health Emergency Operation Centre (PHEOC). The information on suspected or confirmed RVF is sent immediately within 24 hours to the PHEOC through a national hotline (4).
Despite the prolonged presence of RVF in Uganda, there is inadequate information on the distribution of RVF among humans in the country. We described the trends and spatial distribution of RVF outbreaks among humans, Uganda, 2016–2023 to inform programming.
Methods
Study setting
Uganda is divided in four regions: Western, Eastern, Northern, and Central. These regions are then subdivided into 146 districts. As of 2022, the projected population of Uganda stood at 44,212,800, with an annual growth rate of 3.3% (5). The majority of the households constituting 58%, depend on livestock as a source of livelihood (2). Notably, most of livestock rearing occurs within the cattle corridor districts of Uganda. The country experiences two rainy seasons (March–May and September–December).
Study design and data source
We analysed event-based surveillance data reported through the electronic Public Health Emergency Management (ePHEM) database of the MoH, 2016–2023. As per IDSR guidelines, a confirmed RVF case was as any patient who, after clinical screening, with positive for either anti-RVF immunoglobulin M(IgM) Enzyme-Linked Immunosorbent Assay (ELISA) antibodies or Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) test. Any RVF case not linked to another known RVF case was considered an RVF outbreak (6).
Study variables and data abstraction
We abstracted data on number of RVF cases, fatalities, confirmed cases, affected districts, onset and end date of the outbreak, as well as the month and year.
Data management and analysis
We conducted a descriptive analysis of RVF outbreaks by time and place using Microsoft Excel 2019. We conducted univariate analysis to obtain frequencies and proportions of outbreaks, cases, deaths, districts affected, and regions affected. We calculated the Case Fatality Rate (CFR) as the proportion of people who died from RVF among all indivuduals diagnosed with RVF over a certain period of time (2016-2023). We used Quantum Geographic Information System (QGIS) version 3.22 to generate maps to show the distribution of RVF outbreaks.
Ethical considerations
The Ministry of Health Uganda provided administrative clearance to conduct this investigation. In addition, we received a non-research determination clearance from the US Centers for Disease Prevention and Control (US CDC). This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy. § §See e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. No informed consent from participants was sought since secondary data was used.
Results
Rift valley fever outbreaks, Uganda, 2016–2023
During 2016–2023, a total of 43 RVF outbreaks were reported through the EBS system, ePHEM with an average of five outbreaks annually. These outbreaks resulted in 340 reported cases averaging 43 cases each year, with an average of 7.9 cases per outbreak. Over the study period, 42 deaths (average of five deaths annually), yielding a CFR, of 12.4%. Of the 340 cases, 116 (34.1%) were confirmed. On average, RVF outbreaks lasted for 72 days (10 weeks) with a range of 24–127 days from the time of reporting to the public health facilities to the time when the response was completed.
Rift Valley Fever outbreaks have been reported across all regions in Uganda. Western region reported the highest number of RVF outbreaks (27/43, 63%), cases (302/340, 89%) and deaths (31/42, 73.8%) with CFR of 10%, followed by Central Uganda which reported 12 outbreaks, 34 cases and 9 deaths with CFR of 27%. Eastern Uganda reported the least number of outbreaks, with no recorded deaths (Table 1). However, there was no significant difference in the number of outbreaks by region (p=0.213).
Table 1: Percentage of rift valley fever outbreaks, cases, and deaths by region, Uganda, 2016-2023
| Region | Outbreaks | Cases | Deaths | CFR% | |||
| Number | % | Number | % | Number | % | ||
| Western | 27 | 63 | 302 | 89 | 31 | 73.8 | 10 |
| Central | 12 | 28 | 34 | 10 | 9 | 21.4 | 27 |
| Northern | 3 | 7 | 3 | 0.9 | 2 | 4.8 | 67 |
| Eastern | 1 | 2 | 1 | 0.3 | 0 | 0 | 0 |
| Total | 43 | 100 | 340 | 100 | 42 | 100 | 12 |
Rift valley fever outbreaks and cases by year, Uganda, 2016–2023
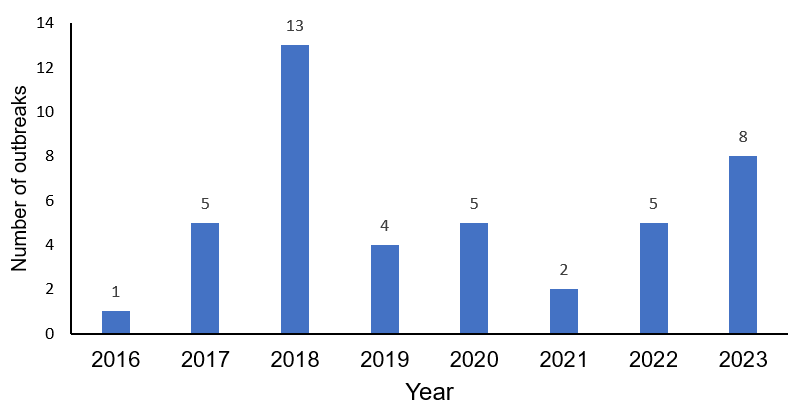
The number of outbreaks reported per year ranged from 1 in 2016 to 13 in 2018 (Figure 1). The average number of RVF outbreaks was 5.4 outbreaks per year. The highest number of RVF outbreaks was reported in 2018 (n=13, 30.2%), followed by 2023 (n=8, 18.6%). The least number of RVF outbreaks were reported in 2016 (n=1, 2.3%).
Rift valley fever cases and deaths during rift valley fever outbreaks, Uganda, 2016–2023
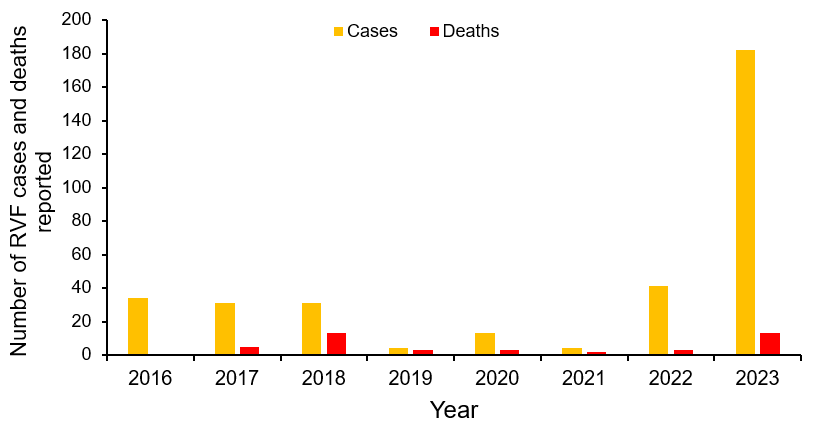
The highest number of RVF cases were reported in 2023 (n=182, 53.5%), followed by 2022 (n=41, 12.1%). The highest number of deaths were reported in 2023 (n=13, 31%) and 2018 (n=13, 31%). The highest number of deaths were reported in 2018 and 2023 (Figure 2).
Monthly distribution of rift valley fever outbreaks, Uganda, 2016–2023
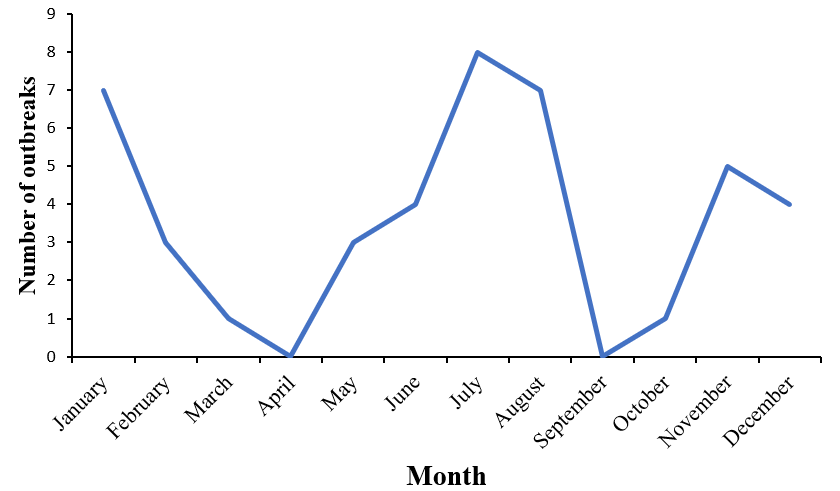
The majority (29/43) of RVF outbreaks were reported in the dry season (June–August and January– February) compared to the rainy season (March–May and September–December). The highest number of outbreaks were reported between June and August. From 2016– 2023, most outbreaks were reported in July (8/43, 19%). No outbreaks were reported in April and September over a period of 8 years. In 2018, most outbreaks were reported in July (n=5), followed by June (n=3), and August (n=3). In 2017, most RVF outbreaks were reported in November (n=3) and December (n=2). In 2023, most outbreaks were reported in January (Figure 3).
Spatial distribution of rift valley fever cases and outbreaks, Uganda, January 2016–2023
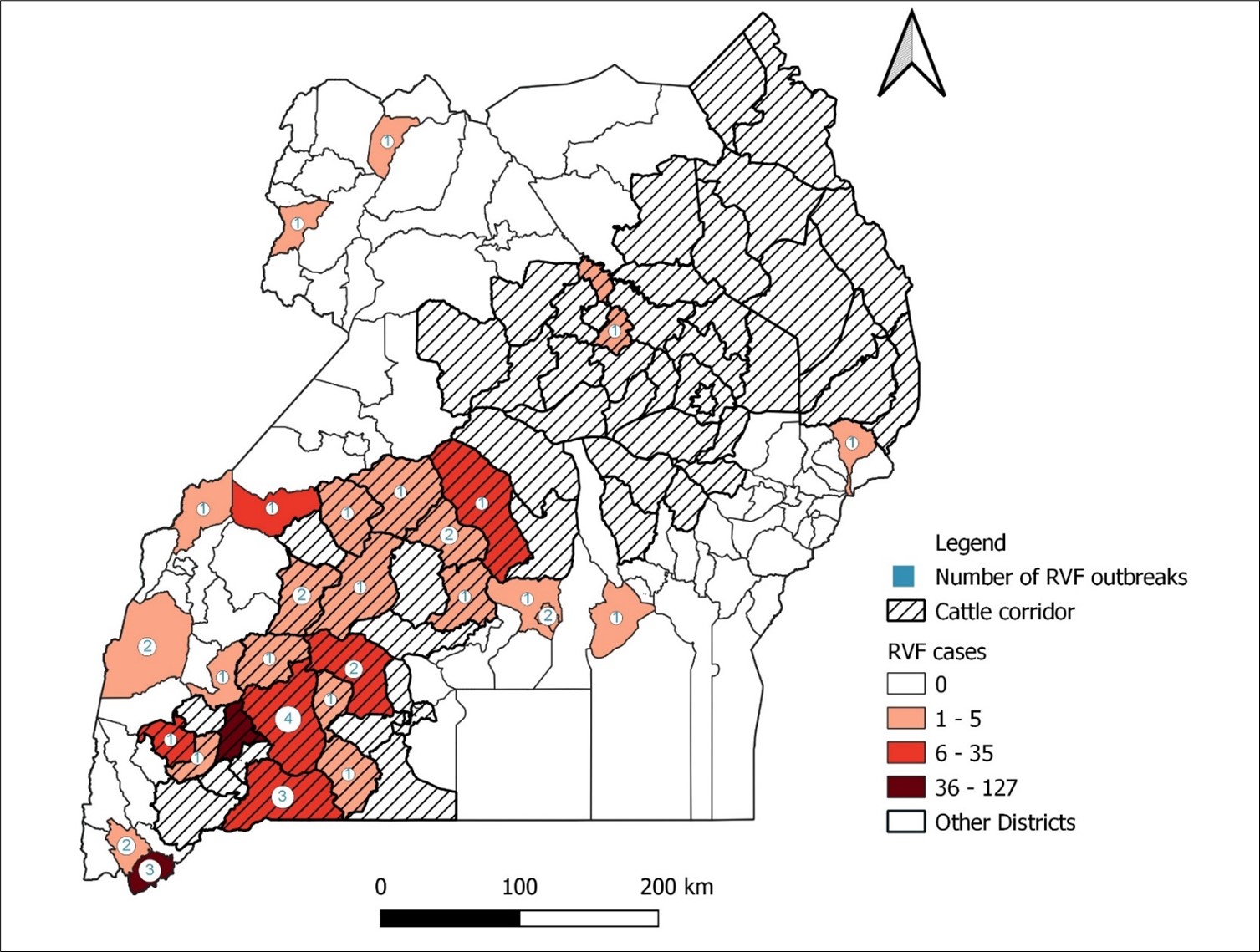
Out of 146 districts, 29 (19.9%) reported at least an outbreak of RVF affecting humans between 2016–2023 (Figure 4). Most of these outbreaks were reported in Mbarara (n=4, 13.8%), and Kiruhura (n=4, 13.8%), followed by Isingiro (n=3, 10.3%) and Kabale (n=3, 10.3%) districts. The highest number of RVF cases were reported in Mbarara (n=127, 37.4%) and Kabale districts (n=49, 14.4%) . Most outbreaks (60%) were reported in the cattle corridor districts (Figure 3).
Discussion
We found that a total of 43 outbreaks were reported from 2016–2023 resulting in 340 cases and 42 deaths. RVF outbreaks occurred in all four regions of the country, with the highest number reported in the Western region. Sixty percent of the outbreaks were reported in the cattle corridor districts.
Since 2016, Uganda has grappled with sporadic outbreaks of RVF. Between 2016–2023, 43 RVF outbreaks involving 340 individuals were reported. The number of outbreaks and cases were likely under-estimated due to under-reporting; because RVF often manifests with either as mild or asymptomatic constraining its diagnosis (1). The disease is often misdiagnosed with other endemic diseases such as malaria. Moreover, RVF commonly affects individuals residing in rural areas where health centers may be far (7). Given that the definitive diagnosis for RVFV can only be achieved through laboratory, there is an urgent need to build the capacity of regional laboratories to test for RVF.
The RVF outbreaks were reported in all regions of Uganda across the study period, potentially attributed to animal movements during trade (7). Notably, the Western and Central regions reported high numbers of RVF cases and outbreaks. This finding is consistent with a study conducted in 2023 that utilized national seroprevalence data from cattle, goats, and sheep to map the risk of RVF in Uganda (8). The Western region and the cattle corridor districts emerged as hotspots for RVF outbreaks and cases. Particularly, Mbarara and Kiruhura districts stood out for reporting the highest number of RVF outbreaks. This trend could be attributed to the predominant livestock farming in the cattle corridor stretching across South-Western Uganda where Mbarara and Kiruhura lies (2). Consequently, increased livestock-human interaction contributes to the transmission of RVFV from animals to humans.
The majority of the outbreaks occurred following the dry season and end-of-year festive season, this could be as a result of increased slaughter and trade in animal and animal products (7). The increase in outbreaks during the festive season indicates a possible increase in human activities, including slaughter and trade of animals and animal products. This heightened activity may contribute to the transmission of the RVF virus from animals to humans. These findings highlight the need for targeted interventions during specific times of the year to effectively control and prevent RVF outbreaks, safeguarding both animal and human health.
The highest number of outbreaks were reported in 2018 and January 2023. This could be explained by the enhanced surveillance during the Ebola virus disease (EVD) outbreak that occurred in 2018 in the Democratic Republic of Congo and the 2022–2023 EVD outbreak that occurred in Uganda, leading to a high index of suspicion of RVF (9)
The study found a higher overall CFR of 12.4%. This is higher than that <1% documented by the World Health Organisation (1). This could be attributed to the under-detection of RVF cases since the majority of the RVF case-patients may present with no or mild symptoms. The high CFR could be because only the patients with severe RVF disease present to health facilities and are detected late by the disease surveillance system (10).The majority of the patients presenting with mild symptoms may then remain undetected by the surveillance system. The high case fatality rate could also be attributed to the late detection of RVF cases which is as a result of low suspicion index among clinicians. The disease is suspected by some clinicians when the patients start to experience hemorrhagic signs which are usually present in the terminal stages of the severe disease (11).
Study limitations
This study had some limitations. First, the outbreaks whose data we analysed primarily focused on reported RVF cases by the health facilities. the symptoms of RVF mimic many other endemic infections in Uganda such as malaria and other arboviral fevers. As a result, human cases are diagnosed and observed only late during outbreaks or not diagnosed at all. These factors contribute to reporting bias likely leading to an underestimation of the magnitude of of RVF during the study period. Secondly, we used secondary data associated with missing data on several variables hence limited on a detailed exploration of the RVF outbreaks/cases during the reporting period.
Conclusion
Uganda has experienced increasing sporadic outbreaks of RVF since March 2016. Strengthening efforts to prevent and control RVF in Uganda could reduce the occurrence of RVF outbreaks, particularly in regions and districts with the high number of RVF outbreaks. We recommend MoH to enhance RVF surveillance throughout the year to understand the true burden of the disease. We further recommended investigations to identify factors contributing to the occurrence of RVF outbreaks in Uganda. By addressing the shortfalls reported in this study, Uganda can strengthen its preparedness and response mechanisms to better combat the threat of RVF.
Conflict of interest
The authors declare that they have no conflict of interest.
Authors contribution
All authors contributed to the write-up and review of the bulletin. MK wrote the drafts of the bulletin and revised the paper for substantial intellectual content. BK, RM, DM, SL,, IK, and ARA reviewed the paper for substantial intellectual content. MK and JK participated in the abstracting of the secondary data. All the authors read and approved the final version of the bulletin.
Acknowledgements
The authors thank the staff of the Uganda Public Health Fellowship Program for the technical support and guidance offered during this study. The authors also extend their appreciation to the management and staff of the Public Health Emergency Operation Centre under MoH for the techical support they offered during this study. Finally, we thank the US-CDC for funding this activity.
Copyright and licensing
All materials in the Uganda Public Health Bulletin are in the public domain and may be used and reprinted without permission; citation as to source; however, is appreciated. Any article can be reprinted or published. If cited as a reprint, it should be referenced in the original form.
References
- World Health Organization. Rift Valley Fever 2018 [23/August/2023:[
- Food and Agriculture Organization. The future of livestock in Uganda. Opportunities and Challenges in the fac of uncertainity.; 2019.
- Kasye M, Eshetu A, Gebeyehu D. A Review on Rift Valley Fever on Animal, Human Health and its Impact on Live Stock Marketing. 2016;3:8.
- Ministry Of Health, editor. National Technical Guideliness for Integrated Disease Surveillance and Response. Third Edition ed2023.
- Uganda Bureau of Statistics. Summary of National Population Projections (2015–2040) 2019 [Available from: https://www.ubos.org/?pagename=explore-publications&p_id=20.
- Ministry of Health. National Technical Guidelines for Integrated Disease Surveillance and Response. Third ed2023.
- Chevalier V, Pépin M, Plée L, Lancelot R. Rift Valley fever–a threat for Europe? Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2010;15(10):19506.
- Tumusiime D, Isingoma E, Tashoroora OB, Ndumu DB, Bahati M, Nantima N, et al. Mapping the risk of Rift Valley fever in Uganda using national seroprevalence data from cattle, sheep and goats. PLoS Negl Trop Dis. 2023;17(5):e0010482.
- Nyakarahuka L, Whitmer S, Klena J, Balinandi S, Talundzic E, Tumusiime A, et al. Detection of Sporadic Outbreaks of Rift Valley Fever in Uganda through the National Viral Hemorrhagic Fever Surveillance System, 2017-2020. The American journal of tropical medicine and hygiene. 2023;108(5):995-1002.
- Nyakarahuka L, Whitmer S, Klena J, Balinandi S, Talundzic E, Tumusiime A, et al. Detection of Sporadic Outbreaks of Rift Valley Fever in Uganda through the National Viral Hemorrhagic Fever Surveillance System, 2017–2020. The American journal of tropical medicine and hygiene. 2023;108(5):995-1002.
- Hassan A, Muturi M, Mwatondo A, Omolo J, Bett B, Gikundi S, et al. Epidemiological Investigation of a Rift Valley Fever Outbreak in Humans and Livestock in Kenya, 2018. The American journal of tropical medicine and hygiene. 2020;103(4):1649-55.
Comments are closed.