
Mysterious Deaths Caused by Consumption of Alcohol Adulterated with High Concentrations of Methanol, Wakiso District-Uganda, June 2017
Authors: Doreen Birungi1, Patricia Eyu1, Denis Okethwangu1, Claire Biribawa1, Susan Kizito1, Benon Kwesiga1; Affiliation: 1Uganda Public Health Fellowship Program
Summary
On the 23rd June, 2017, Ministry of Health was notified of mysterious deaths in Wakiso District, Central Uganda. We conducted an epidemiological investigation to determine cause of mysterious deaths, identify risk factors for mysterious deaths, and recommend preventative measures. We identified 15 case-persons of which (12) twelve were males. The median age was 43.4 years (IQR: 36-55). 12 deaths and 3 survivors were registered (CFR; 80%). 13/15 (87%) cases re- ported having last drunk locally distilled alcohol (waragi) from a bar that was supplied by a salesman denoted as X before onset of symptoms compared to 15/84(18%) controls who had also drunk from the same (OR=29.9; 95% CI: 6.1- 146.6). 14/15 (93%) cases compared to 39/84 controls (46%) usually drunk waragi (OR; 16.2; 95% CI: 2.03-128.5). Toxicological findings on locally distilled alcohol revealed high levels of methanol above the recommended safe level of 50mg/l. Deaths in Wakiso district were caused by consumption of locally distilled alcohol adulterated with methanol. We recommended enforcement of laws and policies that governs sale of alcohol to the public.
Introduction
On the 23rd June, 2017, Ministry of Health through the Public Health Emergency Operations Centre was notified of mysterious deaths in Wakiso District, Central Uganda. Sudden deaths involving seven persons from Maganjo Parish in Nabweru sub-county were reported. The case-persons presented with history of sudden onset of headache, vomiting, loss of sight, sudden loss of consciousness resulting into death.
Following this alert, a team from Ministry of Health was constituted to conduct an epidemiological investigation to determine the cause of the mysterious deaths, identify risk factors for mysterious deaths, and recommend control measures for the outbreak
Methods
We defined a suspected case as onset of acute loss of sight, and any of the following symptoms: vomiting, headache, nausea, dizziness, loss of consciousness in a resident of Nabweru or Nangabo sub-counties, Wakiso District from 1st June, 2017 onwards. We carried out active case finding with the help of local council leaders and VHTs. We reviewed medical records at Ruth Gaylord Hospital in Kawempe B, Trinah Medical clinic in Ttula where the case- persons were admitted. We interviewed survivors, and persons at the homes where deaths occurred as well as held focus group discussions with the local leaders in the affected villages.
A total of 15 case-persons were line listed. We conducted descriptive analysis to generate a hypothesis as stated, “Consuming contaminated locally distilled alcohol was associated with the deaths in Wakiso district”. We conducted a case-control study to test the hypothesis in which one case was matched to 4 controls by residence, and alcohol drinking status. We defined a control person as an asymptomatic adult (>18years) living in Nabweru, and Nangabo sub-counties,
Wakiso district who consumes alcohol. We submitted samples of locally distilled alcohol from the implicated drinking joints, and from the supplier of the bars to the Government Analytical Laboratory (GAL) for toxicological analysis. In addition, we collected blood samples the three survivors and submitted to GAL for toxicological analysis. We also reviewed postmortem results for one of the cases. Together with the Police authorities, we collected locally distilled alcohol samples from supplier X, and from the implicated drinking joints. We followed the trail of the implicated alcohol to identify the source.
Results
A total of 15 cases were identified of which 12 were males. The median age was 43.4 years (IQR: 36-55). A total of 12 deaths and 3 survivors were registered (CFR; 80%). Attack rate was highest among males (7.6%) compared to females (2.1%).
Two sub-counties of Nabweru and Nangabo in Wakiso district were affected. Four zones (equivalent to a village), Ttula –Kidokolo, Kawempe A, Kawempe B and Kizingiza were affected. The most affected zone was Ttula-Kidokolo (AR 9.26/10,000). Ttula –Kidokolo had the lowest CFR (3/6) (50%), compared to Kawempe A (3/3) (100%), Kawempe B (4/4)(100%), Kizingiza (2/2) (100%).
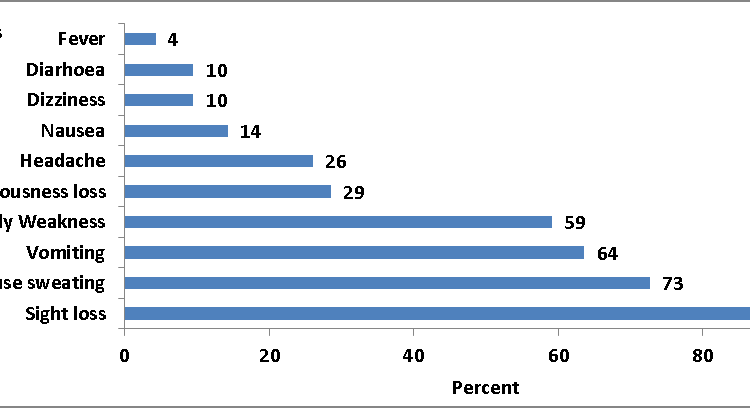
The symptoms were consistent with methanol poisoning. All cases had a history of acute loss of sight (Fig 1).
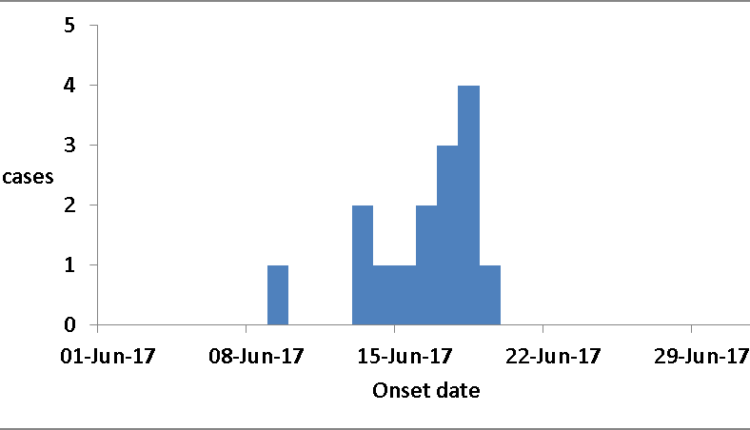
The first case developed symptoms on 9th June, 2017, followed by a sharp rise in cases from 13th June to 19th June, 2017. The average latent period (time between ingestion and development of symptoms) for all cases was one day. The median time between onset of symptoms and death was 19 hours (Fig 2).
Laboratory and Post Mortem results: The locally distilled alcohol contained methanol quantities above the recommended safe levels of 50mg/L. The average methanol in alcohol samples tested was 1200.27mg/L (77.16mg/L- 2711.2mg/L). In 20% (2/10) of the samples, Esters of 45.096 mg/L and 34.188mg/L which are above the recommended safe level of 30mg/L were detected. Similarly, volatile acidity of 86.76mg/L and 56.684mg/L which are also above the recommended safe level of 50mg/L were detected. Post mortem was carried from National Referral Hospital (Mulago) immediately after death occurrence and results for one of the case-person showed broncho-pneumonia.
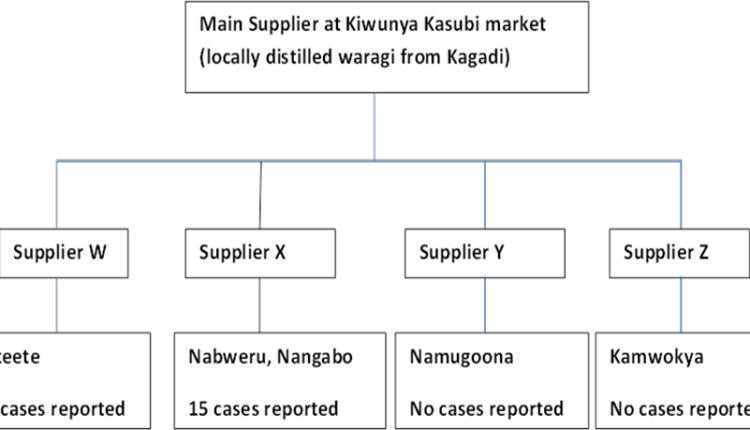
Environment Assessment: The implicated alcohol was locally distilled from Kagadi district and brought to Kiwunya Kasubi for sale. It was sold to various parts of Kampala and Wakiso districts which did not report any cases of methanol poisoning, apart from Nabweru and Nangabo supplied by supplier X (Fig 2).
Case-control study findings: 13/15 (87%) cases re- ported that they had last drunk local waragi from a bar that was supplied by salesman X, before onset of symptoms compared to 15/84(18%) controls who had also drunk from the same (OR=29.9; 95% CI: 6.1- 146.6).
In addition, 14/15 (93%) cases, compared to 39/84 (46%) controls usually drink locally distilled gin (waragi), (OR; 16.2; 95% CI: 2.03-128.5). 14/15(93%) cases drunk alcohol packed in sachets compared to 49/84 (58%) controls, (OR; 10; 95% 1.3-79.6). Drinking beer was not a significant risk factor (OR; 0.3; 95% CI: 0.1-1.1).
Discussion
Methanol poisoning is a relatively rare but potentially serious medical emergency. Toxicity results when methanol is oxidized to formaldehyde and formic acid. In Uganda, deaths over years have been caused by methanol poisoning some of which include; 7 deaths in Kasana, Kampala in 2009, 5 deaths in 2005 in Kasese, 40 deaths in 2007 in Kampala (ProMED-EAFR, 2009). Drinking locally distilled alcohol was a risk factor for this outbreak.
Though still uncertain how locally distilled alcohol was contaminated, amounts of methanol that are toxic were found in the implicated alcohol. Trace amounts of methanol are usually found naturally in fruit juices and this is non-toxic (WHO, 2014). Methanol is also a product of fermentation and is found in both alcoholic and non-alcoholic drinks in concentrations that are not harmful. Problems arise when high- er concentrations are formed during incorrectly managed distillation processes, but more particularly when methanol is deliberately added to fortify informally-produced spirits and illicit alcoholic drinks (WHO, 2014). In this outbreak, there is a high suspicion that industrial methanol which was added to alcohol intended for sale.
The case fatality rate for this outbreak was 80%, this is above rates of other outbreaks that see a case fatality rate of 30%. This can be attributed to the fact that victims sought medical care after a significant delay. Late medical care contributes to the high level of morbidity and mortality seen in many methanol poisoning outbreaks. (Hovda, 2005).
Conclusions and Recommendations
Sudden deaths in Wakiso District were caused by consumption of locally distilled alcohol adulterated with high concentrations of methanol. We suspect supplier X to have adulterated the alcohol. We recommended enforcement of laws governing alcohol distillation and production.
Public health campaigns should be put in place to promote awareness of the dangers of informally produced and illicit alcoholic drinks. Uganda National Bureau of Standards should conduct impromptu quality control checks of locally distilled alcohol.
References
- Kraut, 2016 Approach to the Treatment of Methanol Intoxication. American Journal of Kidney diseases
- Hantson P, WitteboleX , Haufroid V . Ethanol therapy for methanol poisoning: duration and problems. Eur J Emerg Med 2002; 9: 278 – 279
- Hovda, KE et al. Methanol outbreak in Norway 2002- 2004: epidemiology, clinical features and prognostic Journal of Internal Medicine. 2005; 258:181-190.
- ProMED-EAFR. (2009). Undiagnosed fatalities – Uganda – Methanol poisoning WHO. (2014). Methanol Poisoning Outbreaks. World Health Organization
Comments are closed.